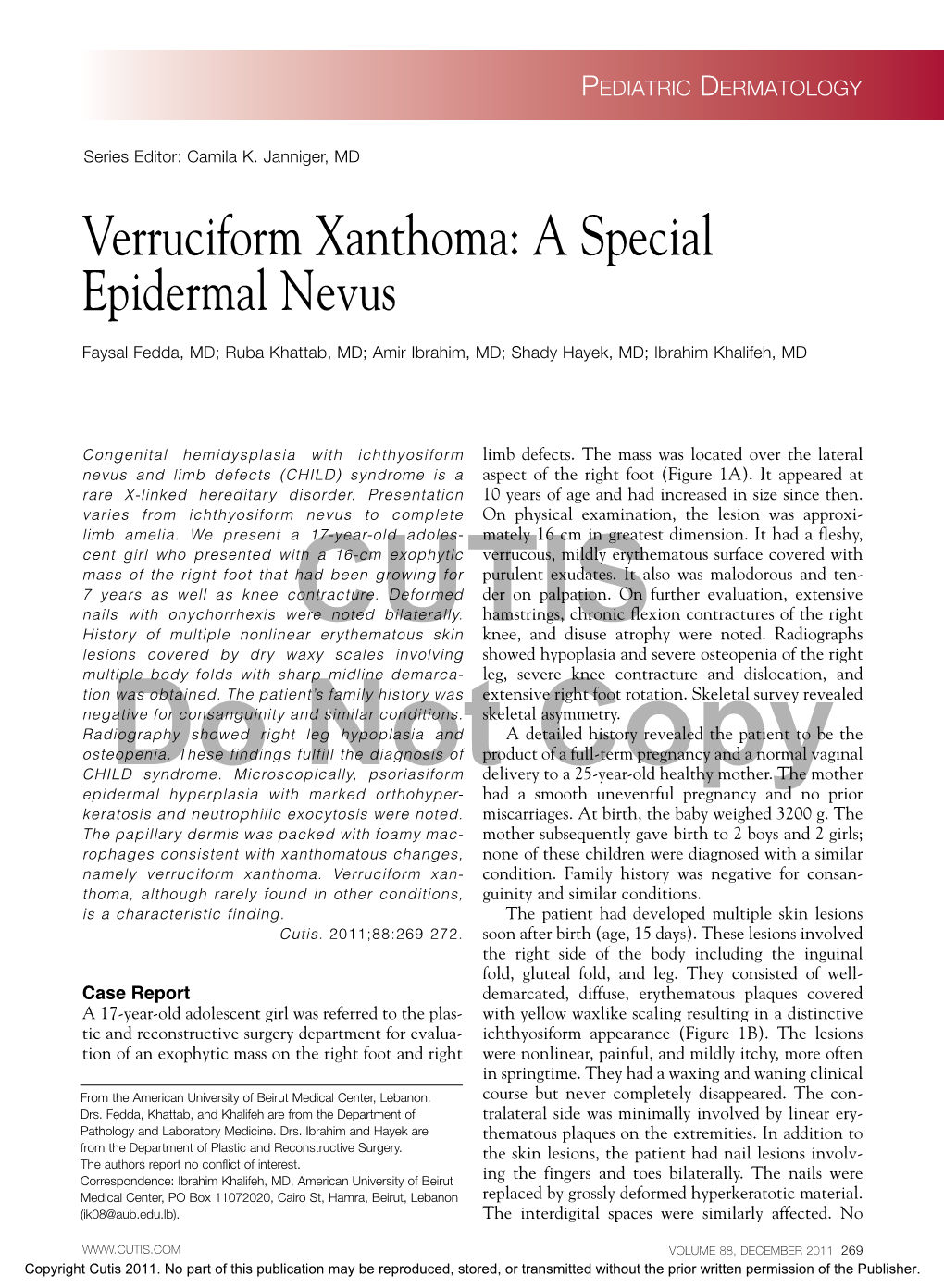
Verruciform Xanthoma: a Special Epidermal Nevus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary for Narrative Writing
Periodontal Assessment and Treatment Planning Gingival description Color: o pink o erythematous o cyanotic o racial pigmentation o metallic pigmentation o uniformity Contour: o recession o clefts o enlarged papillae o cratered papillae o blunted papillae o highly rolled o bulbous o knife-edged o scalloped o stippled Consistency: o firm o edematous o hyperplastic o fibrotic Band of gingiva: o amount o quality o location o treatability Bleeding tendency: o sulcus base, lining o gingival margins Suppuration Sinus tract formation Pocket depths Pseudopockets Frena Pain Other pathology Dental Description Defective restorations: o overhangs o open contacts o poor contours Fractured cusps 1 ww.links2success.biz [email protected] 914-303-6464 Caries Deposits: o Type . plaque . calculus . stain . matera alba o Location . supragingival . subgingival o Severity . mild . moderate . severe Wear facets Percussion sensitivity Tooth vitality Attrition, erosion, abrasion Occlusal plane level Occlusion findings Furcations Mobility Fremitus Radiographic findings Film dates Crown:root ratio Amount of bone loss o horizontal; vertical o localized; generalized Root length and shape Overhangs Bulbous crowns Fenestrations Dehiscences Tooth resorption Retained root tips Impacted teeth Root proximities Tilted teeth Radiolucencies/opacities Etiologic factors Local: o plaque o calculus o overhangs 2 ww.links2success.biz [email protected] 914-303-6464 o orthodontic apparatus o open margins o open contacts o improper -

Bilateral Lower Extremity Hyperkeratotic Plaques: a Case Report of Ichthyosis Vulgaris
Faculty & Staff Scholarship 2015 Bilateral lower extremity hyperkeratotic plaques: a case report of ichthyosis vulgaris Hayley Leight Zachary Zinn Omid Jalali Follow this and additional works at: https://researchrepository.wvu.edu/faculty_publications Clinical, Cosmetic and Investigational Dermatology Dovepress open access to scientific and medical research Open Access Full Text Article CASE REPORT Bilateral lower extremity hyperkeratotic plaques: a case report of ichthyosis vulgaris Hayley Leight Abstract: Here, we report a case of a middle-aged woman presenting with severe, long-standing, Zachary Zinn hyperkeratotic plaques of the lower extremities unrelieved by over-the-counter medications. Omid Jalali Initial history and clinical findings were suggestive of an inherited ichthyosis. Ichthyoses are genetic disorders characterized by dry scaly skin and altered skin-barrier function. A diagnosis Department of Dermatology, West Virginia University, of ichthyosis vulgaris was confirmed by histopathology. Etiology, prevalence, and treatment Morgantown, WV, USA options are discussed. Keywords: filaggrin gene, FLG, profilaggrin, keratohyalin granules, hyperkeratosis Introduction For personal use only. Inherited ichthyoses are a diverse group of genetic disorders characterized by dry, scaly skin; hyperkeratosis; and altered skin-barrier function. While these disorders of cutaneous keratinization are multifaceted and varying in etiology, disruption in the stratum corneum with generalized scaling is common to all.1–4 Although not entirely known -

1 Structure and Function of the Skin
Go Back to the Top To Order, Visit the Purchasing Page for Details 1 Chapter 1 Structure and Function of the Skin The skin is the human body’s its largest organ, covering 1.6 m2 of surface area and accounting for approximate- ly 16% of an adult’s body weight. In direct contact with the outside environment, the skin helps to maintain four essential bodily functions: ① retention of moisture and prevention of permeation or loss of other molecules, ② regulation of body temperature, ③ protection of the body from microbes and harmful external influences, and ④ sensation. To understand cutaneous biology and skin diseases, it is very important to learn the structure and functions of normal human skin. A. Skin surface The skin surface is not smooth, but is laced with multiple net- works of fine grooves called sulci cutis. These can be deep or shallow. The slightly elevated areas that are surrounded by shal- lower areas of sulci cutis are called cristae cutis. Sweat pores fed crista cutis by the sweat glands open to the cristae cutis (Fig. 1.1). The orientation of the sulci cutis, which differs depending on body location, is called the dermal ridge pattern. Fingerprints and sulcus cutis patterns on the palms and soles, which are unique to each person, are formed by the sulci cutis. Elastic fibers also run in specific directions in deeper parts of the skin, with the direction depend- aabcdefg h i j klmnopqr ing on the site. Some skin diseases, such as epidermal nevus, are known to occur along specific lines distributed over the body, the Blaschko lines (Fig. -

Dermoscopy of Aplasia Cutis Congenita: a Case Report and Review of the Literature
Dermatology Practical & Conceptual Dermoscopy of Aplasia Cutis Congenita: A Case Report and Review of the Literature Rasna Neelam1, Mio Nakamura2, Trilokraj Tejasvi2 1 University of Michigan Medical School, Ann Arbor, MI, USA 2 Department of Dermatology, University of Michigan, Ann Arbor, MI, USA Key words: aplasia cutis congenita, alopecia, dermoscopy, trichoscopy Citation: Neelam R, Nakamura M, Tejasvi T. Dermoscopy of aplasia cutis congenita: a case report and review of the literature. Dermatol Pract Concept. 2021;11(1):e2021154. DOI: https://doi.org/10.5826/dpc.1101a154 Accepted: September 28, 2020; Published: January 29, 2021 Copyright: ©2021 Neelam et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License BY-NC-4.0, which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original author and source are credited. Funding: None. Competing interests: The authors have no conflicts of interest to disclose. Authorship: All authors have contributed significantly to this publication. Corresponding author: Trilokraj Tejasvi, MD, Department of Dermatology, University of Michigan, 1910 Taubman Center, 1500 E. Medical Center Dr, Ann Arbor, MI 48109, USA Email: [email protected] Introduction throbbing, and point tenderness in one of the patches of alo- pecia. The alopecic patch had been present on the right pari- Aplasia cutis congenita (ACC) is a rare heterogeneous con- etal-occipital scalp since birth and has been stable in size and genital disorder characterized by focal or widespread absence appearance for years. Three other round patches of alopecia of the skin. had also been present since birth and remained asymptomatic. -

Ichthyosis Hystrix
Case Report Ichthyosis hystrix Surajit Nayak, Basanti Acharjya, Prasenjit Mohanty Department of Skin ABSTRACT and VD, MKCG Medical College and Hospital, The present report describes the condition in a three day old male child with bilateral ,linear, hyperpigmented and Berhampur, Orissa, India hyperkeratotic verrucous plaques and patchy alopecia over scalpe without any nail and skeletal abnormalities. It was suggestive of ichthyosis hystrix type of epidermal nevus,and is being reported in view of the rarity of this condition. Key words: Icthyosis hystrix, epidermal nevus syndrome, etretinate INTRODUCTION most part of the face. Nails were normal. In the lower limbs, in addition to the nevus, there were Ichthyosis hystrix the nomenclature comes unilateral hyperpigmented [Figure 1] macular from the Greek word and condition was first patches encircling right upper thigh and complete described in England in early 18th century. left thigh, sparing a band-like zone. The term ichthyosis hystrix is used to describe several rare skin disorders in the ichthyosis On physical examination, we could not observe family of skin disorders characterized by massive any defects, especially in skeletal or central hyperkeratosis with an appearance like spiny nervous systems. Routine laboratory examination scales. The term has also been employed to including complete blood count, urine analysis, describe localized and linear warty epidermal nevi liver function test and chest X-ray were all within sometimes associated with mental retardation, normal limits. The parents did not permit a biopsy. seizures or skeletal anomalies. Alopecia and hair and nail abnormalities as well as inner ear Based on the above constellation of clinical deafness were also seen in these patients. -
Abstract Book
Abstract Book First World Conference on Ichthyosis August 31 – September 2, 2007 Münster, Germany Organized by Network for Ichthyoses and related keratinization disorders (NIRK) together with Selbsthilfe Ichthyose e.V. and EU-Coordination Action GENESKIN Contacts: H. Traupe, Münster, Email: [email protected] B. Willis, Münster, Email: [email protected] Barbara Kleinow, Email: [email protected] Geske Wehr, Email: [email protected] Location: Lecture Hall Location:Department of Dermatology University Hospital Von Esmarch-Str. 58 48149 Münster Germany Friday, August 31, 2007 page Workshop on clinical diversity and diagnostic standardization D. Metze, Münster Histopathology of ichthyoses: Clues for diagnostic standardization ..................................... 19 I. Hausser, Heidelberg Ultrastructural characterization of lamellar ichthyosis: A tool for diagnostic standardization 13 H. Verst, Münster The data base behind the NIRK register: a secure tool for genotype/phenotype analysis 34 V. Oji, Münster Classification of congenital ichthyosis ................................................................................... 20 M. Raghunath, Singapore Congenital Ichthyosis in South East Asia ............................................................................. 25 Keratinization disorders and keratins I. Hausser, Heidelberg Ultrastructure of keratin disorders: What do they have in common? ................................... 12 M. Arin, Köln Recent advances in keratin disorders ................................................................................. -

A Case of Acquired Smooth Muscle Hamartoma on the Sole
Ann Dermatol (Seoul) Vol. 21, No. 1, 2009 CASE REPORT A Case of Acquired Smooth Muscle Hamartoma on the Sole Deborah Lee, M.D., Sang-Hyun Kim, M.D., Soon-Kwon Hong, M.D., Ho-Suk Sung, M.D., Seon-Wook Hwang, M.D. Department of Dermatology, Busan Paik Hospital, College of Medicine, Inje University, Busan, Korea A smooth muscle hamartoma is a benign proliferation of INTRODUCTION smooth muscle bundles within the dermis. It arises from smooth muscle cells that are located in arrector pili muscles, Smooth muscle hamartomas (SMH) are a result of benign dartos muscles, vascular smooth muscles, muscularis proliferation of smooth muscle bundles in the dermis. SMH- mammillae and the areolae. Acquired smooth muscle associated smooth muscle cells originate from arrector hamartoma (ASMH) is rare, with only 10 such cases having pili-, dartos-, vulvar-, mammillary- and vascular wall- been reported in the English medical literature to date. Most muscles1-3. SMH is characterized by slightly pigmented of these cases of ASMH were shown to have originated from plaques that contain vellus hairs, and SMH is subdivided arrector pili and dartos muscles. Only one case was reported into two types: congenital smooth muscle hamartoma to have originated from vascular smooth muscle cells. A 21 (CSMH) and acquired smooth muscle hamartoma (ASMH)1-3. year-old woman presented with a tender pigmented nodule, ASMH is a very rare form of SMH that was first described with numbness, on the sole of her foot, and this lesion had by Wong and Solomon1 in 1985, with only such 10 cases developed over the previous 18 months. -

Epidermolytic Hyperkeratosis with Ichthyosis Hystrix Geromanta Baleviciené, MD, Vilnius, Lithuania Robert A
pediatric dermatology Series Editor: Camila K. Janniger, MD, Newark, New Jersey Epidermolytic Hyperkeratosis With Ichthyosis Hystrix Geromanta Baleviciené, MD, Vilnius, Lithuania Robert A. Schwartz, MD, MPH, Newark, New Jersey Epidermolytic hyperkeratosis (EH) is a congenital, autosomal-dominant genodermatosis characterized by blisters.1,2 Shortly after birth, the infant’s skin becomes red and may show bullae. The erythema regresses, but brown verrucous hyperkeratosis persists, particularly accentuated in the flexures. This condition is also known as bullous ichthyosiform erythroderma. The disorder of keratinization has varied clinical manifestations in the extent of cutaneous involve- ment, palmar and plantar hyperkeratosis, and evi- dence of erythroderma. We describe 5 patients, 4 with EH (one of whom had it in localized form and one of whom had an unusual type of ichthyosis hystrix described by Curth and Macklin3-7). Case Reports FIGURE 1. Seven-year-old girl with EH, demonstrating Patient 1—A 7-year-old girl with a cutaneous erup- erythema and verrucous hyperkeratosis (Patient 1). tion since birth characterized by flaccid bullae vary- ing in size. The palms and soles had intense diffuse keratosis from 1 year of age. Her nails, hair, teeth, and mental state were normal. The patient’s mother (Pa- tient 2) had a similar disorder. Skin biopsy specimens showed the changes of EH, with pronounced cellular vacuolation of the middle and upper portions of the malpighian stratum and large, clear, irregular spaces. Cellular boundaries were indistinct. A thickened granular layer was evident with large, irregularly shaped keratohyalin granules. Ultrastructural study showed tonofilament clumping of the malpighian layer and cytolysis. -

Gen Anat-Skin
SKIN • Cutis,integument • External covering • Skin+its appendages-- -integumentary system • Largest organ---15 to 20% body mass. LAYERS • Epidermis •Dermis Types • Thick and thin(1-5 mm thick) • Hairy and non hairy Thick skin EXAMPLES • THICK---PALMS AND SOLES BUT ANATOMICALLY THE BACK HAS THICK SKIN. REST OF BODY HAS THIN SKIN • NON HAIRY----PALMS AND SOLES,DORSAL SURFACE OF DISTAL PHALANX,GLANS PENIS,LABIA MINORA,LABIA MAJORA AND UMBLICUS FUNCTIONS • Barrier • Immunologic • Homeostasis •Sensory • Endocrine • excretory EPIDERMIS(layers) • Stratum basale or stratum germinativum • Stratum spinosum • Stratum granulosum • Stratum lucidum • Stratum corneum Type of cells in epidermis and keratinization • Keratinocytes • Melanocytes • Langerhans • Merkels cells DERMIS LAYERS---- 1.PAPILLARY • Dermal papillae • Complementary epidermal ridges or rete ridges • Dermal ridges in thick skin • Hemidesmosomes present both in dermis and epidermis RETICULAR LAYER •DENSE IRREGULAR CONNECTIVE TIISUE Sensory receptors • Free nerve endings • Ruffini end organs • Pacinian and • Meissners corpuscles Blood supply • Fasciocutaneous A • Musculocutaneous A • Direct cutaneous A APPENDAGES • Hair follicle producing hair • Sweat glands(sudoriferous) • Sebaceous glands • Nails Hair follicle • Invagination of epidermis • Parts---infundibulum, isthmus, inferior part having bulb and invagination HAIR follicle layers • Outer and inner root sheath • Types of hair vellus, terminal, club • Phases of growth— anagen, catagen and telogen Hair shaft • Cuticle •Cortex • Medulla -

Oral Verruciform Xanthoma: Report of 13 New Cases and Review of the Literature
Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e429-35. Oral verruciform xanthoma Journal section: Oral Medicine and Pathology doi:10.4317/medoral.22342 Publication Types: Review http://dx.doi.org/doi:10.4317/medoral.22342 Oral verruciform xanthoma: Report of 13 new cases and review of the literature Paris Tamiolakis 1, Vasileios I. Theofilou 1, Konstantinos I. Tosios 2, Alexandra Sklavounou-Andrikopoulou 3 1 DDS, Postgraduate Student, Department of Oral Medicine and Oral Pathology, School of Dentistry, National and Kapodistrian University of Athens, Greece, 2 Thivon Str, 115 27 Athens, Greece 2 DDS, PhD, Assistant Professor, Department of Oral Medicine and Oral Pathology, School of Dentistry, National and Kapodis- trian University of Athens, Greece, 2 Thivon Str, 115 27 Athens, Greece 3 DDS, MSc, PhD, Professor, Head of Department of Oral Medicine and Oral Pathology, School of Dentistry, National and Ka- podistrian University of Athens, Greece, 2 Thivon Str, 115 27 Athens, Greece Correspondence: Department of Oral Medicine and Oral Pathology School of Dentistry National and Kapodistrian University of Athens Greece, 2 Thivon Str, 11527, Goudi, Athens, Greece [email protected] Tamiolakis P, Theofilou VI, Tosios KI, Sklavounou-Andrikopoulou A. Oral verruciform xanthoma: Report of 13 new cases and review of the literature. Med Oral Patol Oral Cir Bucal. 2018 Jul 1;23 (4):e429-35. http://www.medicinaoral.com/medoralfree01/v23i4/medoralv23i4p429.pdf Received: 05/01/2018 Accepted: 09/05/2018 Article Number: 22342 http://www.medicinaoral.com/ © Medicina Oral S. L. C.I.F. B 96689336 - pISSN 1698-4447 - eISSN: 1698-6946 eMail: [email protected] Indexed in: Science Citation Index Expanded Journal Citation Reports Index Medicus, MEDLINE, PubMed Scopus, Embase and Emcare Indice Médico Español Abstract Background: Oral verruciform xanthoma (OVX) is a rare lesion. -

Oral and Maxillo-Facial Manifestations of Systemic Diseases: an Overview
medicina Review Oral and Maxillo-Facial Manifestations of Systemic Diseases: An Overview Saverio Capodiferro *,† , Luisa Limongelli *,† and Gianfranco Favia Department of Interdisciplinary Medicine, University of Bari Aldo Moro, Piazza G. Cesare, 11, 70124 Bari, Italy; [email protected] * Correspondence: [email protected] (S.C.); [email protected] (L.L.) † These authors contributed equally to the paper. Abstract: Many systemic (infective, genetic, autoimmune, neoplastic) diseases may involve the oral cavity and, more generally, the soft and hard tissues of the head and neck as primary or secondary localization. Primary onset in the oral cavity of both pediatric and adult diseases usually represents a true challenge for clinicians; their precocious detection is often difficult and requires a wide knowledge but surely results in the early diagnosis and therapy onset with an overall better prognosis and clinical outcomes. In the current paper, as for the topic of the current Special Issue, the authors present an overview on the most frequent clinical manifestations at the oral and maxillo-facial district of systemic disease. Keywords: oral cavity; head and neck; systemic disease; oral signs of systemic diseases; early diagnosis; differential diagnosis Citation: Capodiferro, S.; Limongelli, 1. Introduction L.; Favia, G. Oral and Maxillo-Facial Oral and maxillo-facial manifestations of systemic diseases represent an extensive and Manifestations of Systemic Diseases: fascinating study, which is mainly based on the knowledge that many signs and symptoms An Overview. Medicina 2021, 57, 271. as numerous systemic disorders may first present as or may be identified by head and https://doi.org/10.3390/ neck tissue changes. -

Vulvar Verruciform Xanthoma Ten Cases Associated with Lichen Sclerosus, Lichen Planus, Or Other Conditions
OBSERVATION ONLINE FIRST Vulvar Verruciform Xanthoma Ten Cases Associated With Lichen Sclerosus, Lichen Planus, or Other Conditions Charlotte Fite, MD; Franc¸oise Plantier, MD; Nicolas Dupin, MD, PhD; Marie-Franc¸oise Avril, MD; Micheline Moyal-Barracco, MD Background: Verruciform xanthoma (VX) is a rare be- acanthosis without atypia, and elongated rete ridges. nign tumor that usually involves the oral cavity. Since Xanthomatous cells were aggregated in the papillary the first report of this tumor in 1971, only 9 cases have dermis. been reported on the vulva, and 3 of these were associ- ated with another vulvar condition. We describe the clini- Conclusions: Vulvar VX is a benign tumor with mis- copathologic features of 10 patients with vulvar VX and leading clinical features. All 10 cases were associated with focus on their associated conditions. a vulvar condition, mainly a lichen sclerosus. There- fore, VX might represent a reaction pattern induced by Observation: The mean age of the patients was 68 years different conditions, mainly characterized by damage to (range, 51-80 years). The VX lesions were asymptom- the dermoepidermal junction. When confronted with the atic, yellowish-orange verrucous plaques. The diagno- diagnosis of vulvar VX, clinicians may look for an asso- sis was clinically suspected in 2 cases; other suggested ciated vulvar condition. diagnoses were condyloma or squamous cell carci- noma. All of the patients had an associated vulvar con- dition: lichen sclerosus (6 patients), lichen planus (2 Arch Dermatol. 2011;147(9):1087-1092. patients), Paget disease, or radiodermatitis. Under mi- Published online May 16, 2011. croscopy, the VX lesions displayed parakeratosis, doi:10.1001/archdermatol.2011.113 ERRUCIFORM XANTHOMA location, histologic findings, history of dyslip- (VX) is a rare benign tu- idemia, treatment, follow-up, and associated mor which was first vulvar conditions.