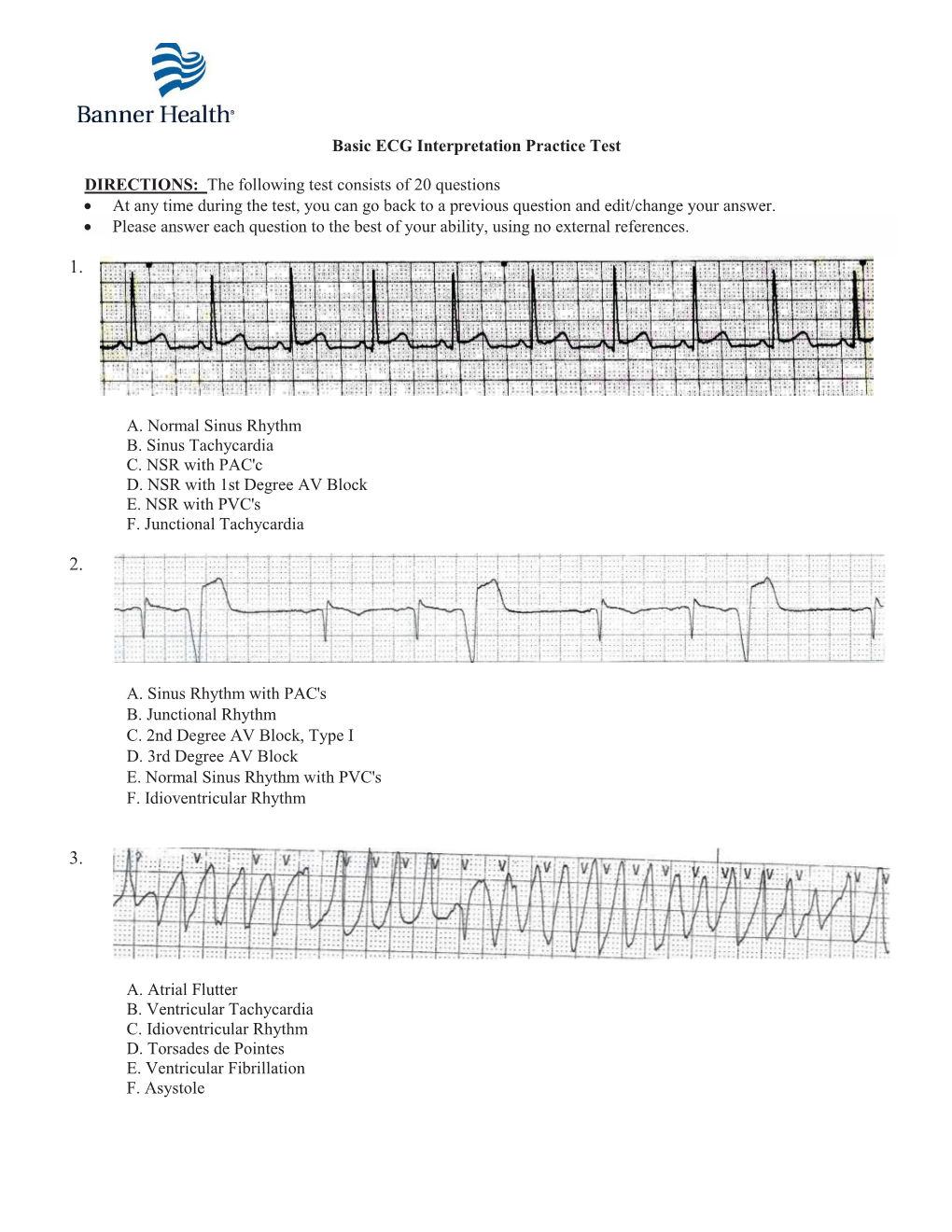
Basic ECG Interpretation Practice Test DIRECTIONS
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Clinical Significance of Exit Block*
Clinical Significance of Exit Block* IRANY M. DE AZEVEDO, M.D. YOSHIO WATANABE, M.D. LEONARD S. DREIFUS, M.D. From the Departments of Medicine, Physiology, and Biophysics, Hahnemann Medical College, Philadelphia, Pennsylvania The confinement of an ectopic discharge to its ily reserved for ectopic pacemakers, rather than the focus, and its consequent inability to invade the ad sinus node. jacent myocardium when falling outside of the re High Grade Atrioventricular Block. In vi rtu fractory period of the heart, is a well established ally all instances, exit block occurs in the presence phenomenon called "exit block." This cardiac ar of higher degrees of A-V block. Failure of the rhythmia was originally described by Kaufmann impulse to propagate from the subsidiary ectopic and Rothberger ( 8) to explain the failure of a para focus to either the ventricles, atria, or both is char systolic focus to activate the heart. All pacemakers acteristic of this form of exit block. Several exam are subject to exit block (9, 13, 15, 14, 11 , 16, 12, ples are illustrated. In figure 2, there is high grade 3, 10, 7, 1), however, by convention, conduction A-V block causing A-V dissociation. The atria are disturbances involving the sinus node (S-A block) under the control of the sinus node at a rate of 71 are usually excluded from this concept, and the term per minute, and the ventricles are controlled by a is reserved for ectopic pacemakers. Recent electro subsidiary ectopic pacemaker, probably originating physiological and clinical studies have shown that in the right bundle branch at a rate of approximately exit block may complicate reentrant arrhythmias and 40 per minute. -

Non Commercial Use Only
Cardiogenetics 2017; volume 7:6304 Sudden death in a young patient with atrial fibrillation Case Report Correspondence: María Angeles Espinosa Castro, Inherited Cardiovascular Disease A 22-year-old man suffered a sudden Program, Cardiology Department, Gregorio María Tamargo, cardiac arrest without previous symptoms Marañón Hospital, Dr. Esquerdo, 46, 28007, María Ángeles Espinosa, while he was at rest, waiting for a subway Madrid, Spain. Víctor Gómez-Carrillo, Miriam Juárez, train. Cardiopulmonary resuscitation was Tel.: +34.91.586.82.90. immediately started using an Automated E-mail: [email protected] Francisco Fernández-Avilés, External Defibrillation that identified the Raquel Yotti Key words: KCNQ1; mutation; channelopa- presence of ventricular fibrillation and thy; sudden cardiac death; atrial fibrillation. Inherited Cardiovascular Disease delivered a shock. Return of spontaneous Program, Cardiology Department, circulation was achieved after three Contributions: MT, acquisition and interpreta- Gregorio Marañón Hospital, Madrid, attempts, being atrial fibrillation (AF) the tion of data for the work, ensuring that ques- Spain patient’s rhythm at this point (Figure 1). tions related to the accuracy or integrity of any He was admitted to our Cardiovascular part of the work is appropriately investigated Intensive Care Unit and therapeutic and resolved; MAE, conception of the work, hypothermia was performed over a period critical revision of the intellectual content, final approval of the version to be published, Abstract of 24 h. After completing hypothermia, ensuring that questions related to the accuracy rewarming, and another 24 h of controlled of any part of the work is appropriately inves- Sudden cardiac death (SCD) in young normothermia the patient awakened with no tigated and resolved; VG-C, acquisition and patients without structural heart disease is residual neurologic damage. -
Common Arrhythmias� Disclosures
Common Arrhythmias Disclosures • I work for Virginia Garcia Memorial Health Center. • And I am a medical editor for Jones & Bartlett Publishing. Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor What a 12-Lead ECG can help you do • Diagnose ACS / AMI • Interpret arrhythmias • Identify life-threatening syndromes (WPW, LGL, Long QT synd., Wellens synd., etc) • Infer electrolyte imbalances • Infer hypertrophy of any chamber • Infer COPD, pericarditis, drug effects, and more! Arabic, Somali, Mai Mai, Pashtu, Urdu, ASL, and more! For example… WPW with Atrial Fib 55 66 Wolff-Parkinson-WhiteWPW Graphic synd. Same pt, converted to SR Drs. Wolff, Parkinson, & White 77 Another example: Dr. William Stokes—1800s 71 y.o. man with syncope This patient is conscious and alert! Third Degree Block 9 Treatment: permanent pacemaker 10 Lots of ways to read ECGs… Limitations of a 12-Lead ECG • QRSs wide or narrow? • Is it sinus rhythm or not? • Truly useful only ~40% of the time • Regular or irregular? • If not, is it atrial fibrillation? • Each ECG is only a 10 sec. snapshot • Fast or slow? • BBB? • P waves? • MI? • Serial ECGs are necessary, especially for ACS • Other labs help corroborate ECG findings (cardiac markers, Cx X-ray) • Confounders must be ruled out (LBBB, dissecting aneurysm, pericarditis, WPW, Symptoms: digoxin, LVH, RVH) • Syncope is bradycardia, heart blocks, or VT • Rapid heart beat is AF, SVT, or VT Conduction System Lead II P wave axis …upright in L II II R T P R U Q S …upright in L II R wave axis SA Node AV Node His Bundle BBs Purkinje Fibers 14 13 Q S Normal Sinus Rhythm Triplicate Method: 6-second strip: 6 seconds 300, 150, 100, Count PQRST cycles in a 6 75, 60, 50 second strip & multiply x 10 Quick, easy, sufficient Easy, & more accurate 300 150 100 75 60 6 seconds What is the heart rate? Horizontal axis is time (mS); vertical axis is electrical energy (mV) 16 1. -

Prolonged Asystole During Hypobaric Chamber Training
Olgu Sunumları Anadolu Kardiyol Derg 520 Case Reports 2012; 12: 517-24 contraction/ventricular tachycardia’s originating from mitral annulus contractions arising from the mitral annulus: a case with a pure annular are rarely reported (1). origin. Pacing Clin Electrophysiol 2009; 32: 680-2. [CrossRef] PVCs arising from the mitral annulus frequently originate from 5. Kimber SK, Downar E, Harris L, Langer G, Mickleborough LL, Masse S, et al. anterolateral, posteroseptal and posterior sites (2). It has been reported Mechanisms of spontaneous shift of surface electrocardiographic configuration that 2/3 of the PVCs arising from the mitral annulus originate from during ventricular tachycardia. J Am Coll Cardiol 1992; 15: 1397-404. [CrossRef] anterolateral site (2). Furthermore, small part of these arrhythmias origi- Address for Correspondence/Yaz›şma Adresi: Dr. Ömer Uz nates from the anteroseptal site of the mitral annulus. Ablation of this Gülhane Askeri Tıp Akademisi Haydarpasa, Kardiyoloji Kliniği, İstanbul-Türkiye site may be technically very challenging. Cases have been reported that Phone: +90 216 542 34 65 Fax: +90 216 348 78 80 successful catheter ablation of the premature ventricular contraction E-mail: [email protected] origin from the anteroseptal site of the mitral annulus can be performed Available Online Date/Çevrimiçi Yayın Tarihi: 22.06.2012 either by a transseptal or transaortic approach in literature (3, 4). ©Telif Hakk› 2012 AVES Yay›nc›l›k Ltd. Şti. - Makale metnine www.anakarder.com web Anterolateral site of the mitral annulus is in close proximity to anterior sayfas›ndan ulaş›labilir. of the right ventricle outflow tract, left ventricular epicardium near to ©Copyright 2012 by AVES Yay›nc›l›k Ltd. -

Wide Flbs & QRS Tachycardias
Wide FLB’s and QRS Tachycardias Reading Assignment (p30-41 and 42-44) Welcome to the “5-Step Method” ECG #: Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= PR= QRS= QT= Axis= 1. Compute the 5 basic measurements: HR, PR interval, QRS duration, QT interval, Axis 2. What’s the basic rhythm and other rhythm statements (e.g., PACs and PVC’s) 3. Any conduction abnormalities (SA blocks, AV blocks (Types I or II), and IV blocks 4. Waveform abnormalities beginning with P waves, QRS complexes, ST-T, and U waves 5. Final interpretations: Normal ECG or Borderline or Abnormal ECG (list final conclusions) 44 Year old man in the ER with palpitations and lightheadedness 7-1 rsR’ Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V=210 Wide QRS tachycardia • IVCD • rsR‘ in V1 Abnormal ECG: • Late S (rightward forces) in 1. High probability SVT with RBBB PR= I, aVL, V6 Clues: classic triphasic (rsR‘) RBBB QRS=1120 morphology in V1 is very unlikely to be VT. The most likely SVT mechanism in this QT=240 ECG is AVNRT with RBBB. 7-1 Axis= indeterminate 65 Year old man in the ICU with hypotension 7-2 qR in V1 rS in V6 Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V=140 Wide QRS tachycardia • IVCD • Northwest quadrant axis Abnormal ECG: (lead I and II both negative) • Left ventricular tachycardia PR= • qR pattern in V1 • rS pattern in V6 ECG Clues for VT in this case: 1) NW QRS=150 quadrant axis; 2) qR in V1; rS in V6. QT=340 Clinical clues: hypotension 7-2 Axis= -120 (NW Quadrant) I II III 7-3 75 Year old man in the ICU with recent acute coronary syndrome Mearurements: Rhythm (s): Conduction: Waveform: Interpretation: A= V= 135 Wide QRS tachycardia • IVCD • fat R in V1 (red arrows) Abnormal ECG: • Notch on downstroke of S 1. -

Atrial Arrhythmia Triggering Electromechanical Dissociation And
EP CASE REPORT ....................................................................................................................................................... Atrial arrhythmia triggering electromechanical dissociation and ventricular fibrillation in a patient with atrial switch operation Nicolas Combes1,2,3*, Stefano Bartoletti1,2,Se´bastien Hascoet€ 3, Olivier Vahdat2, Franc¸ois Heitz2, and Victor Waldmann 4,5 1Electrophysiology Unit, Clinique Pasteur, Toulouse, France; 2Pediatric and Adult Congenital Heart Disease Department, Clinique Pasteur, 45, Avenue de Lombez, 31076 Toulouse, France; 3Pediatric and Adult Congenital Heart Disease Department, Hoˆpital Marie Lannelongue, Le Plessis-Robinson, France; 4Cardiology Department, Electrophysiology Unit, European Georges Pompidou Hospital, Paris, France; and 5Cardiology Department, Adult Congenital Heart Disease Unit, European Georges Pompidou Hospital, Paris, France * Corresponding author. Tel: 133 562213131; fax: 133 562211641. E-mail address: [email protected] A 26-year-old man with D- transposition of the great arteries (D-TGA) and pre- vious Mustard atrial switch surgery was referred for catheter ablation of a recur- rent symptomatic paroxys- mal atrial flutter. The arrhythmia was easily induci- ble (Figure 1A, cycle length 310 ms, rate 194 b.p.m.), with rapid conduction to the ventricles. While mapping flutter, simultaneous record- ing of endocardial signals and invasive blood pressure monitoring showed haemo- dynamic deterioration with intermittent electromechan- ical dissociation (Figure 1B) and then pulseless electrical activity (Figure 1C). After ini- tiation of cardiopulmonary resuscitation, several electric shocks failed to restore sinus rhythm and atrial flutter transitioned a few minutes later into ventricular tachy- cardia and then ventricular fibrillation (Figure 1D); this was ultimately terminated by defibrillation after an Figure 1 (A) Atrial flutter on 12-lead ECG induced by atrial bursts (240 ms), average ventricular response adrenaline bolus. -

Constrictive Pericarditis Causing Ventricular Tachycardia.Pdf
EP CASE REPORT ....................................................................................................................................................... A visually striking calcific band causing monomorphic ventricular tachycardia as a first presentation of constrictive pericarditis Kian Sabzevari 1*, Eva Sammut2, and Palash Barman1 1Bristol Heart Institute, UH Bristol NHS Trust UK, UK; and 2Bristol Heart Institute, UH Bristol NHS Trust UK & University of Bristol, UK * Corresponding author. Tel: 447794900287; fax: 441173425926. E-mail address: [email protected] Introduction Constrictive pericarditis (CP) is a rare condition caused by thickening and stiffening of the pericar- dium manifesting in dia- stolic dysfunction and enhanced interventricu- lar dependence. In the developed world, most cases are idiopathic or are associated with pre- vious cardiac surgery or irradiation. Tuberculosis remains a leading cause in developing areas.1 Most commonly, CP presents with symptoms of heart failure and chest discomfort. Atrial arrhythmias have been described as a rare pre- sentation, but arrhyth- mias of ventricular origin have not been reported. Figure 1 (A) The 12 lead electrocardiogram during sustained ventricular tachycardia is shown; (B and C) Case report Different projections of three-dimensional reconstructions of cardiac computed tomography demonstrating a A 49-year-old man with a striking band of calcification around the annulus; (D) Carto 3DVR mapping—the left hand panel (i) demonstrates a background of diabetes, sinus beat with late potentials at the point of ablation in the coronary sinus, the right hand panel (iii) shows the hypertension, and hyper- pacemap with a 89% match to the clinical tachycardia [matching the morphology seen on 12 lead ECG (A)], and cholesterolaemia and a the middle panel (ii) displays the three-dimensional voltage map. -

The Syndrome of Alternating Bradycardia and Tachycardia by D
Br Heart J: first published as 10.1136/hrt.16.2.208 on 1 April 1954. Downloaded from THE SYNDROME OF ALTERNATING BRADYCARDIA AND TACHYCARDIA BY D. S. SHORT From the National Heart Hospita. Received September 15, 1953 Among the large number of patients suffering from syncopal attacks who attended the National Heart Hospital during a four-year period, there were four in whom examination revealed sinus bradycardia alternating with prolonged phases of auricular tachycardia. These patients presented a difficult problem in treatment. Each required at least one admission to hospital and in one case the symptoms were so intractable as to necessitate six admissions in five years. Two patients had mitral valve disease, one of them with left bundle branch block. One had aortic valve sclerosis while the fourth had no evidence of heart disease. THE HEART RATE The sinus rate usually lay between 30 and 50 a minute, a rate as slow as 22 a minute being observed in one patient (Table I). Sinus arrhythmia was noted in all four patients, wandering of TABLE I http://heart.bmj.com/ RATE IN SINus RHYTHM AND IN AURICULAR TACHYCARDIA Rate in Case Age Sex Associated Rate in auricular tachycardia heart disease sinus rhythm Auricular Venliicular 1 65 M Aortic valve sclerosis 28-48 220-250 60-120 2 47 F Mitral valve disease 35-75 180-130 90-180 on September 26, 2021 by guest. Protected copyright. 3 38 F Mitral valve disease 22-43 260 50-65 4 41 F None 35-45 270 110 the pacemaker in three, and periods of sinus standstill in two (Fig. -
Atrial Flutter Patient Information
AF A Atrial flutter patient information Providing information, support and access to established, new or innovative treatments for atrial fibrillation www.afa-international.org Registered Charity No. 1122442 Glossary Antiarrhythmic drugs Drugs used to restore the Contents normal heart rhythm Introduction Anticoagulant A group of drugs which help to thin the blood and prevent AF-related stroke What is atrial flutter? Arrhythmia A heart rhythm disorder What causes atrial flutter? Atrial flutter A rhythm disorder characterised by a rapid but regular atrial rate although not as high as What are the atrial fibrillation symptoms of atrial flutter? A therapy to treat arrhythmias Cardioversion How do I get to which uses a transthoracic electrical shock to revert see the right doctor the heart back into a normal rhythm to treat my atrial flutter? Catheter ablation A treatment by which the small area inside the heart which has been causing atrial What are the risks flutter is destroyed of atrial flutter? Echocardiogram An image of the heart using Diagnosis and echocardiography or soundwave-based technology. treatment An echocardiogram (nicknamed ‘echo’) shows a three-dimensional shot of the heart Treatment of atrial flutter Electrocardiogram (ECG) A representation of the heart’s electrical activity in the form of wavy lines. Drug treatments An ECG is taken from electrodes on the skin surface Stroke prevention The inability (failure) of the heart to Heart failure Non-drug treatments pump sufficient oxygenated blood around the body to meet physiological requirements 2 Introduction Atrial flutter is a relatively common heart rhythm The heart disturbance encountered by doctors, although not and normal as common as atrial fibrillation (AF). -

Unstable Angina with Tachycardia: Clinical and Therapeutic Implications
Unstable angina with tachycardia: Clinical and therapeutic implications We prospectively evaluated 19 patients with prolonged chest pain not evolving to myocardiai infarction and accompanied with reversible ST-T changes and tachycardia (heart rate >lOO beats/min) in order to correlate heart rate reduction with ischemic electrocardiographic (ECG) changes. Fourteen patients (74%) received previous long-term combined treatment with nifedipine and nitrates. Continuous ECG monitoring was carried out until heart rate reduction and at least one of the following occurred: (1) relief of pain or (2) resolution of ischemic ECG changes. The study protocol consisted of carotid massage in three patients (IS%), intravenous propranolol in seven patients (37%), slow intravenous amiodarone infusion in two patients (lo%), and intravenous verapamil in four patients (21%) with atrial fibrillation. In three patients (16%) we observed a spontaneous heart rate reduction on admission. Patients responded with heart rate reduction from a mean of 126 + 10.4 beats/min to 64 k 7.5 beats/min (p < 0.005) and an ST segment shift of 4.3 k 2.13 mm to 0.89 k 0.74 mm (p < 0.005) within a mean interval of 13.2 + 12.7 minutes. Fifteen (79%) had complete response and the other four (21%) had partial relief of pain. A significant direct correlation was observed for heart rate reduction and ST segment deviation (depression or elevation) (f = 0.7527 and 0.8739, respectively). These patients represent a unique subgroup of unstable angina, in which the mechanism responsible for ischemia is excessive increase in heart rate. Conventional vasodilator therapy may be deleterious, and heart rate reduction Is mandatory. -

What Are Premature Ventricular Contractions?
What Are Premature Ventricular Contractions? Premature ventricular contractions (VPCs or PVCs) are irregular beats that originate from the heart’s pumping chambers (ventricles). These beats interrupt the normal regular (sinus) rhythm, and result in irregularity to the heart rhythm. Although single PVCs are not life- threatening, they may indicate the presence of underlying heart disease, or when they become more severe can cause rapid and dangerous increases in heart rate (ventricular tachycardia). WHAT CAUSES PREMATURE VENTRICULAR CONTRACTIONS? PVCs can occur secondary to a variety of causes, most concerning being cardiac disease. PVCs are most commonly seen in dogs with Dilated Cardiomyopathy, but can also occur in the later stages of disease with Myxomatous Mitral Valve Degeneration. PVCs and other ventricular arrhythmias can also with no evidence of underlying structural heart disease. The workup for PVCs can be frustrating, because PVCs can also occur secondary to conditions unrelated to the heart. Most commonly they can occur secondary to gastrointestinal disease, systemic disease, and pain. HOW ARE PREMATURE VENTRICULAR CONTRACTIONS DIAGNOSED? Most commonly, your veterinarian will hear an irregular heart rhythm and recommend an electrocardiogram (ECG) to assess the heart rhythm. The ECG will enable your veterinarian to determine whether the irregular rhythm is due to PVCs. Following this diagnosis, there are several additional recommended tests. TESTING Following this diagnosis, there are several additional recommended tests. ECHOCARDIOGRAPHY Echocardiography (heart ultrasound) is recommended to make sure that there is no evidence of structural cardiac disease causing the abnormal heart rhythm. 24-HOUR HOLTER Single PVCs usually do not require treatment, however a Holter monitor will determine whether the frequency or severity of the MONITOR PVCs warrant anti-arrhythmic medication, and make sure that there is no evidence of ventricular tachycardia, which is a life threatening heart rhythm. -

Sick Sinus Syndrome in Children
Arch Dis Child: first published as 10.1136/adc.51.2.100 on 1 February 1976. Downloaded from Archives of Disease in Childhood, 1976, 51, 100. Sick sinus syndrome in children OLIVE SCOTT, FERGUS J. MACARTNEY, and PHILIP B. DEVERALL From the Department of Paediatric Cardiology,Killingbeck Hospital, Leeds Scott, O., Macartney, F. J., and Deverall, P. B. (1976). Archives of Disease in Childhood, 51, 100. Sick sinus syndrome in children. The ages of 6 male patients with the sick sinus syndrome ranged from 10-15 years when their symptoms began. At rest all had a heart rate of 60/min or less. Two had syncopal attacks which threatened life; 1 had only attacks of dizziness; the other 3 had no syncopal attacks but had recurrent attacks of supraventricular tachycardia ('brady-tachycardia syndrome') which were more resistant to drug therapy than is usual in childhood. They were not controlled or suppressed by digoxin when it was given. Substernal pain occurred in 2 patients who had syncope. In all patients the heart rate remained inappropriately slow after exercise and atropine. Cardiac pacemakers were used in the 2 patients with life-threatening syncope. Any patient who has dizziness or syncopal attacks and an inappropriately slow heart rate should have electrocardiograms recorded at rest and after excerise to record the heart rate and to look for abnormal P-waves. Dysfunction of the sinoatrial node has been sudden death in childhood than has been previously copyright. increasingly recognized over the past few years. recognized. An awareness of the condition may Most reported cases have been in adults and only a result in more cases being diagnosed.