Volume and Its Relationship to Cardiac Output and Venous Return S
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Integration of Detailed Modules in a Core Model of Body Fluid Homeostasis and Blood Pressure Regulation
Integration of detailed modules in a core model of body fluid homeostasis and blood pressure regulation. Alfredo Hernández, Virginie Le Rolle, David Ojeda, Pierre Baconnier, Julie Fontecave-Jallon, François Guillaud, Thibault Grosse, Robert Moss, Patrick Hannaert, Randall Thomas To cite this version: Alfredo Hernández, Virginie Le Rolle, David Ojeda, Pierre Baconnier, Julie Fontecave-Jallon, et al.. Integration of detailed modules in a core model of body fluid homeostasis and blood pres- sure regulation.. Progress in Biophysics and Molecular Biology, Elsevier, 2011, 107 (1), pp.169-82. 10.1016/j.pbiomolbio.2011.06.008. inserm-00654821 HAL Id: inserm-00654821 https://www.hal.inserm.fr/inserm-00654821 Submitted on 27 Dec 2011 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Integration of detailed modules in a core model of body fluid homeostasis and blood pressure regulation Alfredo I. Hernández1,2, Virginie Le Rolle1,2, David Ojeda1,2, Pierre Baconnier3, Julie Fontecave-Jallon3, François Guillaud4, Thibault Grosse5,6, Robert G. Moss5,6, Patrick Hannaert4, S. Randall Thomas5,6 1INSERM, U642, Rennes, F-35000, France; 2Université de Rennes 1, LTSI, Rennes, F-35000, France; 3 UJF-Grenoble 1 / CNRS / TIMC-IMAG UMR 5525 (Equipe PRETA), Grenoble, F-38041, France 4INSERM U927. -

Regulation of the Systemic Circulation*
CIRCULATORY PHYSIOLOGY SECTION 6: REGULATION OF THE SYSTEMIC CIRCULATION* Summary: This set of notes integrates what we have learned about vascular and cardiac function into a whole so that we can see how the entire circulation is regulated. These are very important concepts and their mastery will move you a long way towards a real understanding of the operation of the circulatory system. I. The Systemic Vascular System -- The influence of cardiac output on the partition of blood between the venous and arterial sides of the systemic circulation. A. Earlier we have indicated that at rest most of the blood in the systemic circulation is located in the venous side. This is in part due to the relatively high capacitance of the venous system when compared to the arterial system. This gives a reserve of blood that can be used when demands for respiratory gas circulation increase as in exercise. B. When there is no circulation (death or experimental interruption of the cardiac output), there is still a blood pressure in both the arterial and venous systems. 1. As we indicated earlier, this is due to the elastic forces stored in the walls of the vessels -- since in the absence of a hemorrhage the vessels contain enough fluid to increase their volume beyond resting volume, there must be a pressure even if the blood is not moving. 2. This low pressure is referred to as the mean circulatory pressure (Guyton) and for normal blood volumes is about 7mmHg (know this value). 3. Due to the greater compliance of the venous system, the greatest relative proportion of the total blood volume will reside in the venous system when operating at the mean circulatory pressure (i.e., when the heart is stopped). -
Ventricular End-Diastolic Volume (Ml)
Stroke Volume and Heart Failure Black/Blue: text. Red: very important. Green: Doctor’s notes. Pink: formulas. Yellow: numbers. Gray: notes and explanation. Physiology Team 436 – Cardiovascular Block Lecture 9 Lecture: If work is intended for initial studying. Review: If work is intended for revision. 1 Objectives Study Smart: focus on mutual topics. From the students’ guide: Explain how cardiac contractility affect stroke volume. Calculate CO using Fick’s principle equation. Explain pathophysiology of heart failure and differentiate between left and right failure. Explain how the pathophysiology associated with heart failure results in typical signs and symptoms. 2 Stroke Volume Stroke volume: is the volume of blood pumped (ejected) by each ventricle per beat (during each ventricular systole), and it is about 70-80 ml/beat. Factors Affecting It: 1- End diastolic volume (EDV) (Preload): • It is: the volume of blood present in each ventricle at the end of ventricular diastole. • Preload: load on the muscle in the relaxed state. Indices of left ventricular • Normal amount: 120-130 ml, can be increased during diastole preload: (filling of ventricles) to a volume of (120-130mL). 1- Left ventricle end diastolic • Applying preload to a muscle causes: volume Or pressure (LVEDV) 1- The muscle to stretch. 2- Right atrial pressure 2- The muscle to develop passive tension. More relaxation time, more filling, more volume. EDV Depends on: A- Filling time: the duration of ventricular diastole. B- Venous return: the rate of blood flow during ventricular diastole. 3 Stroke Volume and Factors Affecting it 1- End diastolic volume (EDV) 2- End systolic volume (ESV) (Residual): (Preload): It is: volume of blood present (that remains) in Mechanism: each ventricle at the end of ventricular systole. -

Determination of Cardiac Output by Equating Venous Return Curves with Cardiac Response Curves
Determination of Cardiac Output By Equating Ve- nous Return Curves With Cardiac Response Curves1 ARTHUR C. GUYTQN From the Department of Physiology and Biophysics, School of Medicine, University of Mississippi, University, Mississippi HE CONCEPT that the heart responds with increasing cardiac output when there occurs increasing venous return was popularized by Starling and, in- deed, has come to be known as Starling’s law. There are many different forms in which Starling’s law can be expressed,including the relationship of cardiac output to right atria1 pressure, the relationship of cardiac output to the degree of distention of the right ventricle at the end of diastole, the relationship of cardiac work to right atria1 pressure or right ventricular distention, the relationship of left ventricular work to right atria1 pressure or right ventricular distention, etc. For the determina- tion of cardiac output, the form of Starling’s law which will be used in the present discussion is the relationship of cardiac output to mean right atria1 pressure, and this type of cruve will be called the “cardiac responsecurve” to right atria1 pressure. It is well known that many factors in the peripheral circulatory system combine together to determine the rate of venous return to the heart. These include the quantity of blood available, the degree of vascular resistance in various parts of the peripheral circulatory system, and the back pressure from the right atrium. It is with these factors that this paper is especially concerned, and it is hoped that this presentation will demonstrate how cardiac output is determined by equating the peripheral circulatory factors with the cardiac responsecurves. -
Venous Return & Factors Affecting Vr
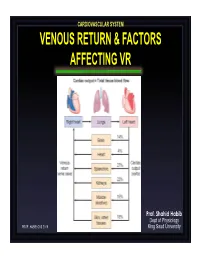
CARDIOVASCULAR SYSTEM VENOUS RETURN & FACTORS AFFECTING VR Prof. Shahid Habib Dept of Physiology PROF. HABIB CVS 2019 King Saud University OBJECTIVES At the end of the lecture you should be able to ….. Discuss functions of the veins as blood reservoirs. Describe measurement of central venous pressure (CVP) and state its physiological and clinical significance. State determinants of venous return and explain how they influence venous return. Define mean systemic filling pressure, give its normal value and describe the factors which affect it. Explain the effect of gravity on venous pressure and explain pathophysiology of varicose veins. Describe vascular and cardiac function curves under physiological and pathophysiological conditions. DISTRIBUTION OF BLOOD Capacitance Vessels Veins are blood reservoirs When the body is at rest and many of the capillaries are closed, the capacity of the venous reservoir is increased as extra blood bypasses the capillaries and enters the veins. When this extra volume of blood stretches the veins, the blood moves forward through the veins more slowly because the total cross sectional area of the veins has increased as a result of the stretching. Therefore, blood spends more time in the veins. When the stored blood is needed, such as during exercise, extrinsic factors reduce the capacity of the venous reservoir and drive the extra blood from the veins to the heart so that it can be pumped to the tissues. Rt. Lt. At At Right Left ven ven Large veins Large arteries CAPACITANCE VESSELS EXCHANGE VESSELS RESISTANCE VESSELS Venules Capillaries Arterioles Vascular circuit • all 3 layers are present, but thinner than in •In varicose veins, arteries of corresponding size (external blood pools because diameter). -

Cardio Vascular Assessment in Vasoplegia Following Cardiac Surgery Kanishka Indraratna*
Review Article ISSN 2639-846X Anesthesia & Pain Research Cardio Vascular Assessment in Vasoplegia Following Cardiac Surgery Kanishka Indraratna* *Correspondence: Kanishka Indraratna, Sri Jayewardenepura General Hospital, Sri Sri Jayewardenepura General Hospital, Sri Lanka, Postal Address- Lanka, Postal Address-7A, Claessen Place, Colombo-5, Sri Lanka, 7A, Claessen Place, Colombo, Sri Lanka. Tel: +94777578144, E-mail: [email protected]. Received: 25 July 2018; Accepted: 29 August 2018 Citation: Indraratna K. Cardiovascular Assessment in Vasoplegia Following Cardiac Surgery. Anesth Pain Res. 2018; 2(2): 1-4. ABSTRACT Severe vasodilatation during cardiac surgery has been known for many years. It is characterized by a low systemic vascular resistance, a high cardiac index, and a low blood pressure, which can be resistant to even high doses of vasoconstrictors. This condition is associated with a high mortality. After cardiac surgery, there can be cardiac dysfunction as well. However with a low systemic vascular resistance, the cardiac function curve would be shifted upwards and to the left, giving the impression of good contractility. The ejection fraction, which is the commonly used measurement of cardiac contractility, cannot therefore be relied upon for a correct assessment under these circumstances. This can affect fluid and inotrope management. Therefore a measurement which does not depend on the afterload, but measures pure myocardial contractility is required. Ventricular elastance is such a measure. A measurement of arterial elastance which reflects the flow characteristics and pulsatility of flow may be more appropriate than systemic vascular resistance to measure arterial tone. Ventricular-arterial coupling has to be maintained for optimum myocardial performance. The severe vasodilatation, the possible myocardial impairment and also its treatment with high doses of vasoconstrictors can affect the relationship between the ventricular and arterial systems. -

Time-Varying Elastance and Left Ventricular Aortic Coupling Keith R
Walley Critical Care (2016) 20:270 DOI 10.1186/s13054-016-1439-6 REVIEW Open Access Left ventricular function: time-varying elastance and left ventricular aortic coupling Keith R. Walley Abstract heart must have special characteristics that allow it to respond appropriately and deliver necessary blood flow Many aspects of left ventricular function are explained and oxygen, even though flow is regulated from outside by considering ventricular pressure–volume characteristics. the heart. Contractility is best measured by the slope, Emax, of the To understand these special cardiac characteristics we end-systolic pressure–volume relationship. Ventricular start with ventricular function curves and show how systole is usefully characterized by a time-varying these curves are generated by underlying ventricular elastance (ΔP/ΔV). An extended area, the pressure– pressure–volume characteristics. Understanding ventricu- volume area, subtended by the ventricular pressure– lar function from a pressure–volume perspective leads to volume loop (useful mechanical work) and the ESPVR consideration of concepts such as time-varying ventricular (energy expended without mechanical work), is linearly elastance and the connection between the work of the related to myocardial oxygen consumption per beat. heart during a cardiac cycle and myocardial oxygen con- For energetically efficient systolic ejection ventricular sumption. Connection of the heart to the arterial circula- elastance should be, and is, matched to aortic elastance. tion is then considered. Diastole and the connection of Without matching, the fraction of energy expended the heart to the venous circulation is considered in an ab- without mechanical work increases and energy is lost breviated form as these relationships, which define how during ejection across the aortic valve. -

2.Heart As Pump
By Adam Hollingworth 2.Heart as a Pump Table of Contents Cardiac Cycle ......................................................................................................................................................... 2 CVS Pressures .................................................................................................................................................................... 3 Heart Failure ..................................................................................................................................................................... 3 Pericardium ....................................................................................................................................................................... 3 Timing .................................................................................................................................................................................. 4 Length of Systole & Diastole ......................................................................................................................................... 4 Arterial Pulse ........................................................................................................................................................ 4 JVP ............................................................................................................................................................................. 4 Cardiac Graph ...................................................................................................................................................... -

Basic Cardiac Rhythms – Identification and Response Module 1 ANATOMY, PHYSIOLOGY, & ELECTRICAL CONDUCTION Objectives
Basic Cardiac Rhythms – Identification and Response Module 1 ANATOMY, PHYSIOLOGY, & ELECTRICAL CONDUCTION Objectives ▪ Describe the normal cardiac anatomy and physiology and normal electrical conduction through the heart. ▪ Identify and relate waveforms to the cardiac cycle. Cardiac Anatomy ▪ 2 upper chambers ▪ Right and left atria ▪ 2 lower chambers ▪ Right and left ventricle ▪ 2 Atrioventricular valves (Mitral & Tricuspid) ▪ Open with ventricular diastole ▪ Close with ventricular systole ▪ 2 Semilunar Valves (Aortic & Pulmonic) ▪ Open with ventricular systole ▪ Open with ventricular diastole The Cardiovascular System ▪ Pulmonary Circulation ▪ Unoxygenated – right side of the heart ▪ Systemic Circulation ▪ Oxygenated – left side of the heart Anatomy Coronary Arteries How The Heart Works Anatomy Coronary Arteries ▪ 2 major vessels of the coronary circulation ▪ Left main coronary artery ▪ Left anterior descending and circumflex branches ▪ Right main coronary artery ▪ The left and right coronary arteries originate at the base of the aorta from openings called the coronary ostia behind the aortic valve leaflets. Physiology Blood Flow Unoxygenated blood flows from inferior and superior vena cava Right Atrium Tricuspid Valve Right Ventricle Pulmonic Valve Lungs Through Pulmonary system Physiology Blood Flow Oxygenated blood flows from the pulmonary veins Left Atrium Mitral Valve Left Ventricle Aortic Valve Systemic Circulation ▪ Blood Flow Through The Heart ▪ Cardiology Rap Physiology ▪ Cardiac cycle ▪ Represents the actual time sequence between -

Pulse Wave Analysis to Estimate Cardiac Output
CLINICAL FOCUS REVIEW Jerrold H. Levy, M.D., F.A.H.A., F.C.C.M., Editor Pulse Wave Analysis to Estimate Cardiac Output Karim Kouz, M.D., Thomas W. L. Scheeren, M.D., Daniel de Backer, M.D., Bernd Saugel, M.D. ardiac output (CO)–guided therapy is a promising reference CO value measured using an indicator dilution Capproach to hemodynamic management in high-risk method (transpulmonary thermodilution or lithium dilu- patients having major surgery1 and in critically ill patients tion).5,9 CO measurement using indicator dilution methods with circulatory shock.2 Pulmonary artery thermodilu- requires a (central) venous catheter for indicator injection tion remains the clinical reference method for CO mea- upstream in the circulation and a dedicated arterial catheter Downloaded from http://pubs.asahq.org/anesthesiology/article-pdf/134/1/119/513741/20210100.0-00023.pdf by guest on 29 September 2021 surement,3 but the use of the pulmonary artery catheter and measurement system to detect downstream indicator decreased over the past two decades.4 Today, various CO temperature or concentration changes.5,9–11 monitoring methods with different degrees of invasiveness The VolumeView system (Edwards Lifesciences, are available, including pulse wave analysis.5 Pulse wave USA) and the PiCCO system (Pulsion Medical Systems, analysis is the mathematical analysis of the arterial blood Germany) calibrate pulse wave analysis–derived CO to pressure waveform and enables CO to be estimated con- transpulmonary thermodilution–derived CO. To measure tinuously and in real time.6 In this article, we review pulse CO using transpulmonary thermodilution, a bolus of cold wave analysis methods for CO estimation, including their crystalloid solution is injected in the central venous circu- underlying measurement principles and their clinical appli- lation.10 The cold indicator bolus injection causes changes cation in perioperative and intensive care medicine. -

JUGULAR VENOUS PRESSURE Maddury Jyotsna
INDIAN JOURNAL OF CARDIOVASCULAR DISEASES JOURNAL in women (IJCD) 2017 VOL 2 ISSUE 2 CLINICAL ROUNDS 1 WINCARS JVP- JUGULAR VENOUS PRESSURE Maddury Jyotsna DEFINITION OF JUGULAR VENOUS PULSE AND The external jugular vein descends from the angle of the PRESSURE mandible to the middle of the clavicle at the posterior Jugular venous pulse is defined as the oscillating top of border of the sternocleidomastoid muscle. The external vertical column of blood in the right Internal Jugular jugular vein possesses valves that are occasionally Vein (IJV) that reflects the pressure changes in the right visible. Blood flow within the external jugular vein is atrium in cardiac cycle. In other words, Jugular venous nonpulsatile and thus cannot be used to assess the pressure (JVP) is the vertical height of oscillating column contour of the jugular venous pulse. of blood (Fig 1). Reasons for Internal Jugular Vein (IJV) preferred over Fig 1: Schematic diagram of JVP other neck veins are IJV is anatomically closer to and has a direct course to right atrium while EJV does not directly drain into Superior vena cava. It is valve less and pulsations can be seen. Due to presence of valves in External Jugular vein, pulsations cannot be seen. Vasoconstriction secondary to hypotension (as in congestive heart failure) can make EJV small and barely visible. EJV is superficial and prone to kinking. Partial compression of the left in nominate vein is usually relieved during modest inspiration as the diaphragm and the aorta descend and the pressure in the two internal -

Chapter 9 Monitoring of the Heart and Vascular System
Chapter 9 Monitoring of the Heart and Vascular System David L. Reich, MD • Alexander J. Mittnacht, MD • Martin J. London, MD • Joel A. Kaplan, MD Hemodynamic Monitoring Cardiac Output Monitoring Arterial Pressure Monitoring Indicator Dilution Arterial Cannulation Sites Analysis and Interpretation Indications of Hemodynamic Data Insertion Techniques Systemic and Pulmonary Vascular Resistances Central Venous Pressure Monitoring Frank-Starling Relationships Indications Monitoring Coronary Perfusion Complications Electrocardiography Pulmonary Arterial Pressure Monitoring Lead Systems Placement of the Pulmonary Artery Catheter Detection of Myocardial Ischemia Indications Intraoperative Lead Systems Complications Arrhythmia and Pacemaker Detection Pacing Catheters Mixed Venous Oxygen Saturation Catheters Summary References HEMODYNAMIC MONITORING For patients with severe cardiovascular disease and those undergoing surgery associ- ated with rapid hemodynamic changes, adequate hemodynamic monitoring should be available at all times. With the ability to measure and record almost all vital physi- ologic parameters, the development of acute hemodynamic changes may be observed and corrective action may be taken in an attempt to correct adverse hemodynamics and improve outcome. Although outcome changes are difficult to prove, it is a rea- sonable assumption that appropriate hemodynamic monitoring should reduce the incidence of major cardiovascular complications. This is based on the presumption that the data obtained from these monitors are interpreted correctly and that thera- peutic decisions are implemented in a timely fashion. Many devices are available to monitor the cardiovascular system. These devices range from those that are completely noninvasive, such as the blood pressure (BP) cuff and ECG, to those that are extremely invasive, such as the pulmonary artery (PA) catheter. To make the best use of invasive monitors, the potential benefits to be gained from the information must outweigh the potential complications.