Technical & Financial File
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Rwanda Irrigation Master Plan
Rwanda Irrigation Master Plan The Government of Rwanda, Ministry of Agriculture & Animal Resources Ebony Enterprises Ltd The World Agroforestry Centre (ICRAF) Rwanda Irrigation Master Plan The Government of Rwanda, Ministry of Agriculture & Animal Resources Ebony Enterprises Limited The World Agroforestry Centre (ICRAF) i Rwanda Irrigation Master Plan The Government of Rwanda, Ministry of Agriculture & Animal Resources Ebony Enterprises Limited The World Agroforestry Centre (ICRAF) Coordinators of IMP Study: NGABONZIZA Prime MAIMBO Mabanga Malesu Supervisor of IMP study: DVOSKIN Dan Authors: MAIMBO Mabanga Malesu ODUOR Alex Raymonds KIPRUTO Cherogony NYOLEI Douglas GACHENE Charles BIAMAH Elijah Kipngetich O’NEIL Mick MIYUKI Ilyama JEPHINE Mogoi Steering Committee Members: SENDEGE Norbert NGABONZIZA Prime NZEYIMANA Innocent MUSABYIMANA Innocent MUSABYIMANA J. Claude AZENE BEKELE Tesemma KAGABO Desire HARINDINTWALI Reverien BAYOULI Amor MOULAYE Abdou Enterprises Ltd. Republic of Rwanda Ministry of Agriculture and Animal Resources, MINAGRI ii Acknowledgement The World Agroforestry Centre greatly appreciates the opportunity accorded by the Managing Director of Ebony Enterprises Limited, Brigadier General (Rtd) Danny Kassif, to participate in the Rwanda Irrigation Master Plan through a sub-contractual agreement signed in March 2009. Upon inception of Phase I study, a number of Ebony personnel provided administrative and logistical support which cannot go unrecognized. These include Pini Moria, Ram Lustgarten, Arik Almog, Adina Avisar and Avi Evron. Cognizance is also extended to the Ministry of Agriculture and Animal Resources for providing technical backstopping and logistical support while carrying out the study in Rwanda. The following Officers are highly appreciated for their contributions to ensuring that Phase I of the study was a success: The Permanent Secretary – MINAGRI, Mr. -

THESIS UWIRAGIYE Emmanuel.Pdf
HOUSEHOLD DEVELOPMENT BENEFITS ASSOCIATED WITH LAND EXPROPRIATION IN KIBEHO AND MUNINI SECTORS UWIRAGIYE Emmanuel A Dissertation submitted to the Department of Development Studies, College of Arts and Social Science (CASS), in partial fulfillment of the requirements for the award of the degree of Master of Arts in Development Studies of the University of Rwanda (UR). Supervisor: Dr UWIZEYE Dieudonné Huye, June 2021 DECLARATION I declare that this thesis is the result of my own work and has not been submitted for any other degree at the University of Rwanda or any other institution. UWIRAGIYE Emmanuel REG No.219014043 Signature: ………… Date: ………………………………………………… Supervisor I certify that this work was done under my supervision, and I confirm that it is ready for examination. DR. UWIZEYE Dieudonné Signature : ………………………………… Date : …………………………………………… I DEDICATION I dedicate this work to all those who toil day and night without advanced education and manage to parry what poverty and limited capabilities hurl on them! II ACKNOWLEDGEMENTS I am grateful to God and to the Jesuits who allowed and sponsored my studies. The completion of this study would not have been possible without the support and encouragement of several special people. I express my gratitude to my supervisor, Dr. UWIZEYE Dieudonné. He provided helpful feedbacks at a surprising pace. His guidance, both during the research and over the entire course of my time at UR was invaluable. I am deeply indebted to him. I humbly acknowledge that within the university I have also had the support of many lecturers, Dr. Buchanan I., Dr. Mulindahabi C., Dr. Ndahiriwe I., Dr Nkurayija J., Dr. -

Emergency Plan of Action (Epoa) Rwanda: Floods and Windstorm
P a g e | 1 Emergency Plan of Action (EPoA) Rwanda: Floods and Windstorm DREF Operation n° MDRRW020 Glide n°: FL-2021-000049-RWA Date of issue: 14 May 2021 Expected timeframe: 3 months Expected end date: 31 August 2021 Category allocated to the of the disaster or crisis: Yellow DREF allocated: CHF 174,720 Total number of 6,500 people (1,300 Number of people to be 3,500 people (700 people affected: households) assisted: households) Provinces affected: Northern and Eastern Provinces/Regions Northern Province of Province of Rwanda (Gicumbi targeted: Rwanda (Gicumbi and and Burera in the North and Burera Districts and Eastern Kayonza District in the Province: Kayonza District Eastern Province Host National Society presence (n° of volunteers, staff, branches): 45 volunteers (6 NRTs, 9 BDRTs, 6 RRC staff (Head of Disaster Response, IT manager, PMER and 3 branch coordinators) Red Cross Red Crescent Movement partners actively involved in the operation: Belgian Red Cross Flanders, French, Spanish, Austrian and Japanese Red Cross Societies and the International Federation of Red Cross and Red Crescent Societies Other partner organizations actively involved in the operation: Ministry of Emergency (MINEMA), Local authorities and Faith based organisation A. Situation Analysis Description of the disaster More recently, from 28 April to 2nd May 2021, extensive flooding and mudslides were reported in Burera District due to waterflows and rocks from the volcanoes. The effects of rains and windstorm has also been observed in other districts including Gicumbi and Kayonza Districts as of 30 April 2021. This has led to extensive destruction of houses, crops, latrines death of livestock, destruction of the roads, and loss of households’ materials and even human death. -
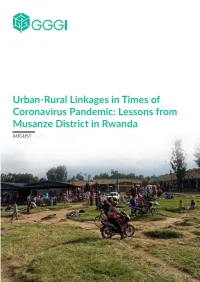
Lessons from Musanze District in Rwanda AUGUST 2020
Urban-Rural Linkages in Times of Coronavirus Pandemic: Lessons from Musanze District in Rwanda AUGUST 2020 1 Copyright © 2020 Global Green Growth Institute Jeongdong Building 19F 21-15 Jeongdong-gil Jung-gu, Seoul 04518 Republic of Korea The Global Green Growth Institute does not make any warranty, either express or implied, or assumes any legal liability or responsibility for the accuracy, completeness, or any third party’s use or the results of such use of any information, apparatus, product, or process disclosed of the information contained herein or represents that its use would not infringe privately owned rights. The views and opinions of the authors expressed herein do not necessarily state or reflect those of the Global Green Growth Institute. Cover Image © Ilija Gubic Acknowledgements This report is written by Ilija Gubic and Andrew Kabera of Global Green Growth Institute. This report was reviewed by Daniel Ogbonnaya and Michelle DeFreese and edited by Michelle DeFreese and Pamela Birungi of Global Green Growth Institute. Illustrations for the report are drawn by Dario Babudri for Global Green Growth Institute while report is designed by Irene Isingizwe of Amasimbi Creative Ltd. 1. Introduction 5 Contents 2. Material and methods 6 3. Importance of urban-rural linkages 7 4. Results and Discussion 8 5. Case Study: Urban-Rural Linkages in 9 Musanze District . 6. Conclusions and Recommendations 21 7. References 21 4 1. Introduction Since December 2019, human life around the an infected person coughs or sneezes. COVID19’s world has been put into turmoil due to the global main difference with other coronaviruses is spread of Coronavirus disease-2019 (COVID-19). -

Rwanda Women's Network Location
1 RWANDA WOMEN’S NETWORK1 ASSERTING WOMEN’S LAND RIGHTS Name: Rwanda Women’s Network Location: Eastern Rwanda Year of foundation: 1997 Contact: Annette Mukiga E-Mail: [email protected] 1 Prepared by Justine Mirembe, in collaboration with Peninah Abatoni, Mary Balikungeri, Elisabetta Cangelosi, Annette Mukiga, Sabine Pallas, Viviana Sacco and the group of women and paralegals of the Polyclinic of Hope in Bugesera. 2 The Context Rwanda Women’s Network (RWN) is a national non-governmental organization working in Rwanda since 1997 when it took over from its parent organization-Church World Service. RWN was established with the mission of promoting and improving the socio-economic welfare of women in Rwanda. Its main administrative offices are located in Gasabo district “village of Hope” - Kigali City but RWN has also established 4 spaces/centers (Polyclinics of Hope) for women in the districts of Gatsibo, Nyarugenge and Bugesera. RWN began with a program of promoting women’s rights to land, housing and inheritance specifically targeting victims of rape and other violent crimes largely perpetuated during the 1994 genocide against Tutsi, as well as vulnerable homeless women returnees after the war. The current population of Rwanda stands at more than 11 million people, over 80% of whom depend on agriculture. With a surface area of 26.338 square kilometer for 11 million people, Rwanda’s population density stands at more than 416 inhabitants per square kilometer (Rwanda Demographic profile, 2013), making it a densely populated country. Gender wise, women constitute more than 53% of the adult population and 50% of these are widows. -

District Profile
THE REPUBLIC OF RWANDA District Profile Nyaruguru Fourth Population and Housing Census, Rwanda, 2012 Rwanda, Census, and Housing Fourth Population NATIONAL INSTITUTE OF STATISTICS OF RWANDA THE REPUBLIC OF RWANDA Ministry of Finance and Economic Planning National Institute of Statistics of Rwanda Fourth Population and Housing Census, Rwanda, 2012 District Profile Nyaruguru January 2015 The Fourth Rwanda Population and Housing Census (2012 RPHC) was implemented by the National Institute of Statistics of Rwanda (NISR). Field work was conducted from August 16th to 30th, 2012. The funding for the RPHC was provided by the Government of Rwanda, World Bank (WB), the UKAID (Former DFID), European Union (EU), One UN, United Nations Population Fund (UNFPA), United Nations Development Programme (UNDP), United Nations Children's Fund (UNICEF) and UN Women. Additional information about the 2012 RPHC may be obtained from the NISR: P.O. Box 6139, Kigali, Rwanda; Telephone: (250) 252 571 035 E-mail: [email protected]; Website: http://www.statistics.gov.rw. Recommended citation: National Institute of Statistics of Rwanda (NISR), Ministry of Finance and Economic Planning (MINECOFIN) [Rwanda]; 2012. Rwanda Fourth Population and Housing Census. District Profile: Nyaruguru xiii xv Fourth Population and Housing Census, Rwanda, 2012 District Profile:Nyaruguru iv Fourth Population and Housing Census, Rwanda, 2012 District Profile:Nyaruguru Table of Content Foreword ................................................................................................................................ -

World Bank Document
SFG1006 REV Rwanda Great Lakes Emergency Sexual and Gender Based Violence and Women’s Health Project Public Disclosure Authorized Environmental and Social Management Approach, including Environmental Management Plan and Medical Waste Management Plan Executive Summary and Conclusions The Environmental and Social Management Approach (ESMA) provides general policies, guidelines, codes of practice and procedures to mainstream environmental and social (E&S) due diligence during the implementation of the World Bank supported Great Lakes Emergency Sexual and Gender Based Violence and Women’s Health Project. The objective of the abbreviated ESMA is to help ensure that activities will be in compliance with the national legislations of Rwanda and the World Bank’s E&S safeguards policies. Public Disclosure Authorized The document is the main due diligence instrument required by the World Bank as financer, and additionally covers and goes beyond the Rwandan national regulatory requirements for project- level environmental assessment and management. The Environmental and Social Management Plan (ESMP) will be the main resource for environmental management and monitoring for the Client and set the standards and practices that will guide environmental and social project performance. It will become part of the tender package and environmental management and compliance will constitute a subsection of line items in the bill of quantities (BoQ). The selected bidders will be required to accept E&S conditions and tasks upon contract signature, and the implementation of the ESMP will be an integral part of the construction contracts. The monitoring of E&S performance will, much as other quality criteria, be tied to contractual penalties and damage restoration requirements via appropriate contractual clauses. -

Nowhere to Go : Informal Settlement Eradication in Kigali, Rwanda
University of Louisville ThinkIR: The University of Louisville's Institutional Repository College of Arts & Sciences Senior Honors Theses College of Arts & Sciences 5-2017 Nowhere to go : informal settlement eradication in Kigali, Rwanda. Emily E Benken University of Louisville Follow this and additional works at: https://ir.library.louisville.edu/honors Part of the Social and Cultural Anthropology Commons Recommended Citation Benken, Emily E, "Nowhere to go : informal settlement eradication in Kigali, Rwanda." (2017). College of Arts & Sciences Senior Honors Theses. Paper 127. http://doi.org/10.18297/honors/127 This Senior Honors Thesis is brought to you for free and open access by the College of Arts & Sciences at ThinkIR: The University of Louisville's Institutional Repository. It has been accepted for inclusion in College of Arts & Sciences Senior Honors Theses by an authorized administrator of ThinkIR: The University of Louisville's Institutional Repository. This title appears here courtesy of the author, who has retained all other copyrights. For more information, please contact [email protected]. NOWHERE TO GO: INFORMAL SETTLEMENT ERADICATION IN KIGALI, RWANDA By Emily Elizabeth Benken Submitted in partial fulfillment of the requirements for Graduation summa cum laude and for Graduation with Honors from the Department of Anthropology University of Louisville May 2017 i ii NOWHERE TO GO: INFORMAL SETTLEMENT ERADICATION IN KIGALI, RWANDA By Emily Elizabeth Benken A Thesis Approved on March 27th, 2017 by the following Thesis Committee: Thesis Advisor Thesis Committee Member Thesis Committee Member iii DEDICATION This thesis is dedicated to my grandmother Mrs. Joyce Graeter Whose unending support made this thesis possible. -

RWANDA Poverty Assessment
RWANDA Poverty Assessment April 2015 Public Disclosure Authorized Poverty Global Practice Africa Region Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized April 2015 1 ׀ RWANDA Poverty Assessment April 2015 ׀ RWANDA Poverty Assessment 2 RWANDA Poverty Assessment Poverty Global Practice Africa Region April 2015 3 ׀ RWANDA Poverty Assessment Table of Contents ABBREVIATIONS AND ACRONYMS ................................................................................................10.... I ACKNOWLEDGEMENTS ........................................................................................................................... VIII11 EXECUTIVE SUMMARY ..............................................................................................................................12 IX 1. A Snapshot of Poverty in Rwanda ..........................................................................................................................12ix Rwanda‘s Poverty Profile: The Expected… ............................................................................................................13 x And the Rather Unexpected … .............................................................................................................................15 xii Inequality is high, driven by location, education, and occupation .......................................................................16 xiii Strong performance in health and basic education ................................................................................................17 -

World Bank Document
REPUBLIC OF RWANDA Public Disclosure Authorized Public Disclosure Authorized UPDATED BY: NYARUGURU DISTRICT AND RWANDA TRANSPORT DEVELOPMENT AGENCY Public Disclosure Authorized RWANDA FEEDER ROADS DEVELOPMENT PROJECT UPDATED RAP REPORT RESETTLEMENT ACTION PLAN FOR SELECTED FEEDER ROADS NYARUGURU DISTRICT Public Disclosure Authorized April 2020 Page 1 of 164 EXECUTIVE SUMMARY The Government of Rwanda (GoR) in partnership with its development partners- initiated Rwanda Feeder Roads Development Project (FRDP) implemented under the coordination of MINAGRI. The Ministry of Finance and Economic Planning (MINECOFIN), by a letter to the World Bank dated October 10, 2017, requested restructuring of the parent Feeder Road Development Project in line with changes to the institutional framework for road management. Accordingly, the Ministry of Agriculture and Animal Resources (MINAGRI), that was responsible for implementation and monitoring of the feeder roads program, was responsible to lead policy formulation. The responsibility of implementation, management and monitoring of all feeder roads programs shifted to RTDA. A Feeder Roads Unit (FRU) that was established in MINAGRI coordinating Development Partners’ (DP) programs, including the World Bank’s, in feeder roads development and has been managing the feeder roads program steering committee. The FRU activities shifted to RTDA. MININFRA and MINAGRI will co-chair the feeder roads program steering committee; RTDA will manage the feeder roads program implementation. The project received financing from IDA to rehabilitate, upgrade and maintain 500 km of selected feeder roads in Rwamagana, Gisagara, Karongi and Nyamasheke Districts. The GoR also applied for additional funding for the rehabilitation of 1200 km of feeder roads in other six districts, namely Gatsibo, Nyagatare, Nyaruguru, Gakenke, Rutsiro and Nyabihu Districts. -

Rwanda USADF Country Portfolio
Rwanda USADF Country Portfolio Overview: Country program was established in 1986 and resumed U.S. African Development Foundation Partner Organization: in 2005 after a pause. USADF currently manages a portfolio of 24 Country Program Coordinator: Geoffrey Kayigi Africa Development Consultants projects and one Cooperative Agreement in Rwanda. PO Box 7210, CCOAIB Building, 3rd Floor Program Director: Rebecca Ruzibuka Total active commitment is $4.33 million. Agricultural investments Remera 1, Plot 2280, Umuganda Bld, Kigali Tel: +250.78.841.5194 total $3.66 million, off-grid energy investments total $348,778, and Tel: +250.78.830.3934 Email: [email protected] youth-led enterprise investments total $25,000. Email: [email protected] Country Strategy: The program focuses on smallholder farmer organizations across the country. Enterprise Duration Grant Size Description Coopérative des Agriculteurs de 2013-2017 $186,800 Sector: Agro-Processing (Maize) Maïs de Nyanza Town/City: Nyanza District, Southern Province (COAMANYA) Summary: The project funds will be used to construct a new factory and purchase approved equipment 2904-RWA and to expand marshland cultivation to another 130 hectares which will directly contribute to an increase of income for over 2,000 persons and promote food security in the area. Funds are also being used to roll out a pilot version of an innovative plot-mapping information system. Coopérative pour le 2015-2017 $78,700 Sector: Processing (Honey) Développement des Apiculteurs et Town/City: Nyamagabe District, Southern Province la Protection de l'Environnement Summary: The project funds will be used to supply beehives, harvesting equipment and to develop an (CODAPE) administrative and financial procedures manual and business plan, as well as to cover key staff 4113-RWA members’ salaries and basic administrative costs to enhance the cooperative’s capacity and boost its honey production and sales revenues. -
TWUBAKANE Decentralization and Health Program Rwanda
TWUBAKANE Decentralization and Health Program Rwanda QUARTERLY PERFORMANCE MONITORING REPORT #18 APRIL— JUNE 2009 USAID/Rwanda Cooperative Agreement # 623-A-00-05-00020-00 Distribution: USAID/Rwanda Twubakane Team Partners Government of Rwanda Ministry of Local Administration Ministry of Health National AIDS Control Commission Twubakane Steering Committee Members Twubakane Partner Districts NGOs, Bilateral and Multi-lateral Partner Agencies Twubakane Quarterly Report #18, April-June, 2009 TABLE OF CONTENTS ACRONYMS ..................................................................................................................................... 1 TWUBAKANE PROGRAM HIGHLIGHTS APRIL-JUNE, 2009 ............................................................ 2 1. INTRODUCTION .................................................................................................................... 3 2. KEY ACCOMPLISHMENTS AND PROGRESS .......................................................................... 3 2.1 TWUBAKANE PROGRAM FIELD OFFICES ............................................................................ 4 3. PERFORMANCE REVIEW BY PROGRAM COMPONENT ........................................................ 4 3.1 FAMILY PLANNING/REPRODUCTIVE HEALTH ACCESS AND QUALITY .............................. 4 3.2 CHILD SURVIVAL, MALARIA AND NUTRITION ACCESS AND QUALITY .............................. 7 3.3 DECENTRALIZATION PLANNING, POLICY AND MANAGEMENT ....................................... 10 3.4 DISTRICT-LEVEL CAPACITY BUILDING ..........................................................................