Recurrent Interlobar Pneumothorax in an Asthmatic Patient
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Spontaneous Pneumothorax in COVID-19 Patients Treated with High-Flow Nasal Cannula Outside the ICU: a Case Series
International Journal of Environmental Research and Public Health Case Report Spontaneous Pneumothorax in COVID-19 Patients Treated with High-Flow Nasal Cannula outside the ICU: A Case Series Magdalena Nalewajska 1, Wiktoria Feret 1 , Łukasz Wojczy ´nski 1, Wojciech Witkiewicz 2 , Magda Wi´sniewska 1 and Katarzyna Kotfis 3,* 1 Department of Nephrology, Transplantology and Internal Medicine, Pomeranian Medical University, 70–111 Szczecin, Poland; [email protected] (M.N.); [email protected] (W.F.); [email protected] (Ł.W.); [email protected] (M.W.) 2 Department of Cardiology, Pomeranian Medical University, 70–111 Szczecin, Poland; [email protected] 3 Department of Anesthesiology, Intensive Therapy and Acute Intoxications, Pomeranian Medical University in Szczecin, 70–111 Szczecin, Poland * Correspondence: katarzyna.kotfi[email protected] Abstract: The coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) has become a global pandemic and a burden to global health at the turn of 2019 and 2020. No targeted treatment for COVID-19 infection has been identified so far, thus supportive treatment, invasive and non-invasive oxygen support, and corticosteroids remain a common therapy. High-flow nasal cannula (HFNC), a non-invasive oxygen support method, has become a prominent treatment option for respiratory failure during the SARS-CoV-2 pandemic. Citation: Nalewajska, M.; Feret, W.; HFNC reduces the anatomic dead space and increases positive end-expiratory pressure (PEEP), Wojczy´nski,Ł.; Witkiewicz, W.; allowing higher concentrations and higher flow of oxygen. Some studies suggest positive effects of Wi´sniewska,M.; Kotfis, K. HFNC on mortality and avoidance of intubation. -

Allergic Bronchopulmonary Aspergillosis: a Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2
Review Allergy Asthma Immunol Res. 2016 July;8(4):282-297. http://dx.doi.org/10.4168/aair.2016.8.4.282 pISSN 2092-7355 • eISSN 2092-7363 Allergic Bronchopulmonary Aspergillosis: A Perplexing Clinical Entity Ashok Shah,1* Chandramani Panjabi2 1Department of Pulmonary Medicine, Vallabhbhai Patel Chest Institute, University of Delhi, Delhi, India 2Department of Respiratory Medicine, Mata Chanan Devi Hospital, New Delhi, India This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. In susceptible individuals, inhalation of Aspergillus spores can affect the respiratory tract in many ways. These spores get trapped in the viscid spu- tum of asthmatic subjects which triggers a cascade of inflammatory reactions that can result in Aspergillus-induced asthma, allergic bronchopulmo- nary aspergillosis (ABPA), and allergic Aspergillus sinusitis (AAS). An immunologically mediated disease, ABPA, occurs predominantly in patients with asthma and cystic fibrosis (CF). A set of criteria, which is still evolving, is required for diagnosis. Imaging plays a compelling role in the diagno- sis and monitoring of the disease. Demonstration of central bronchiectasis with normal tapering bronchi is still considered pathognomonic in pa- tients without CF. Elevated serum IgE levels and Aspergillus-specific IgE and/or IgG are also vital for the diagnosis. Mucoid impaction occurring in the paranasal sinuses results in AAS, which also requires a set of diagnostic criteria. Demonstration of fungal elements in sinus material is the hall- mark of AAS. -

Pneumothorax in Patients with Idiopathic Pulmonary Fibrosis
Yamazaki et al. BMC Pulm Med (2021) 21:5 https://doi.org/10.1186/s12890-020-01370-w RESEARCH ARTICLE Open Access Pneumothorax in patients with idiopathic pulmonary fbrosis: a real-world experience Ryo Yamazaki, Osamu Nishiyama* , Kyuya Gose, Sho Saeki, Hiroyuki Sano, Takashi Iwanaga and Yuji Tohda Abstract Background: Some patients with idiopathic pulmonary fbrosis (IPF) develop pneumothorax. However, the charac- teristics of pneumothorax in patients with IPF have not been elucidated. The purpose of this study was to clarify the clinical course, actual management, and treatment outcomes of pneumothorax in patients with IPF. Methods: Consecutive patients with IPF who were admitted for pneumothorax between January 2008 and Decem- ber 2018 were included. The success rates of treatment for pneumothorax, hospital mortality, and recurrence rate after discharge were examined. Results: During the study period, 36 patients with IPF were admitted with pneumothorax a total of 58 times. During the frst admission, 15 patients (41.7%) did not receive chest tube drainage, but 21 (58.3%) did. Of the 21 patients, 8 (38.1%) received additional therapy after chest drainage. The respective treatment success rates were 86.6% and 66.7% in patients who underwent observation only vs chest tube drainage. The respective hospital mortality rates were 13.3% and 38.0%. The total pneumothorax recurrence rate after hospital discharge was 34.6% (n 9). = Conclusions: Pneumothorax in patients with IPF was difcult to treat successfully, had a relatively poor prognosis, and showed a high recurrence rate. Keywords: Idiopathic pulmonary fbrosis, Hospitalization, Pneumothorax, Recurrence, Treatment Background pneumothorax was signifcantly associated with poor Idiopathic pulmonary fbrosis (IPF) is a specifc form survival in patients with IPF [11]. -

Secondary Spontaneous Pneumothorax in a Patient of Allergic Bronchopulmonary Aspergillosis: an Unusual Presentation
International Journal of Research in Medical Sciences Sandal S et al. Int J Res Med Sci. 2021 Apr;9(4):1205-1208 www.msjonline.org pISSN 2320-6071 | eISSN 2320-6012 DOI: https://dx.doi.org/10.18203/2320-6012.ijrms20211377 Case Report Secondary spontaneous pneumothorax in a patient of allergic bronchopulmonary aspergillosis: an unusual presentation Shivali Sandal1, Surender Kumar2* 1Department of Critical Care Medicine, Inderaprastha Apollo, New Delhi, India 2Department of Cardiology, UN Mehta Institute of Cardiology and Research Centre, Ahmedabad, Gujarat, India Received: 23 January 2021 Accepted: 01 March 2021 *Correspondence: Dr. Surender Kumar, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Allergic bronchopulmonary aspergillosis (ABPA) is a complex immunologic pulmonary disorder caused by hypersensitivity to fungus, Aspergillus fumigates. It clinically manifests with non-specific respiratory and systemic symptoms. ABPA is typically seen in patients with long-standing asthma or cystic fibrosis. Pleural involvement in ABPA is uncommon and secondary spontaneous pneumothorax is very rare. Herein, we report a case of 33 years old male patient presented with dyspnoea, low grade fever and productive cough. High Resolution Computed tomography (HRCT) scan of thorax was suggestive of ABPA with secondary pneumothorax. Keywords: Allergic bronchopulmonary aspergillosis, Aspergillus fumigates, High resolution computed tomography, Secondary spontaneous pneumothorax INTRODUCTION episodes of increasing dyspnea, cough with sputum production, pleuritic pain and fever. -

Cryptogenic Organizing Pneumonia
462 Cryptogenic Organizing Pneumonia Vincent Cottin, M.D., Ph.D. 1 Jean-François Cordier, M.D. 1 1 Hospices Civils de Lyon, Louis Pradel Hospital, National Reference Address for correspondence and reprint requests Vincent Cottin, Centre for Rare Pulmonary Diseases, Competence Centre for M.D., Ph.D., Hôpital Louis Pradel, 28 avenue Doyen Lépine, F-69677 Pulmonary Hypertension, Department of Respiratory Medicine, Lyon Cedex, France (e-mail: [email protected]). University Claude Bernard Lyon I, University of Lyon, Lyon, France Semin Respir Crit Care Med 2012;33:462–475. Abstract Organizing pneumonia (OP) is a pathological pattern defined by the characteristic presence of buds of granulation tissue within the lumen of distal pulmonary airspaces consisting of fibroblasts and myofibroblasts intermixed with loose connective matrix. This pattern is the hallmark of a clinical pathological entity, namely cryptogenic organizing pneumonia (COP) when no cause or etiologic context is found. The process of intraalveolar organization results from a sequence of alveolar injury, alveolar deposition of fibrin, and colonization of fibrin with proliferating fibroblasts. A tremen- dous challenge for research is represented by the analysis of features that differentiate the reversible process of OP from that of fibroblastic foci driving irreversible fibrosis in usual interstitial pneumonia because they may determine the different outcomes of COP and idiopathic pulmonary fibrosis (IPF), respectively. Three main imaging patterns of COP have been described: (1) multiple patchy alveolar opacities (typical pattern), (2) solitary focal nodule or mass (focal pattern), and (3) diffuse infiltrative opacities, although several other uncommon patterns have been reported, especially the reversed halo sign (atoll sign). -

RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax
RCH Trauma Guideline Management of Traumatic Pneumothorax & Haemothorax Trauma Service, Division of Surgery Aim To describe safe and competent management of traumatic pneumothorax and haemothorax at RCH. Definition of Terms Haemothorax: collection of blood in the pleural space Pneumothorax: collection of air in the pleural space Tension Pneumothorax: one way valve effect which allows air to enter the pleural space, but not leave. Air and so intrapleural pressure (tension) builds up and forces a mediastinal shift. This leads to decreased venous return to the heart and lung collapse/compression causing acute life-threatening respiratory and cardiovascular compromise. Ventilated patients are particularly at risk due to the positive pressure forcing more air into the pleural space. Tension pneumothorax results in rapid clinical deterioration and is an emergency. Finger thoracostomy: preferred method of emergency pleural decompression of a tension pneumothorax. It involves incising 3-4cm of skin over the 4th intercostal space just anterior to the mid-axillary line followed by blunt dissection to the pleura to allow introduction of a finger into the pleural space. Main Points 1. Management of a clinically significant traumatic pneumothorax or haemothorax typically requires pleural decompression by chest drain insertion. 2. Anatomical landmarks should be used to determine the site of incision for pleural decompression within the ‘triangle of safety’ to reduce risk of harm. 3. All patients in traumatic cardiac arrest who do not respond immediately to airway opening should have their pleural cavities decompressed by finger thoracostomy, concurrent with efforts to restore the circulating blood volume. 4. With few exceptions, chest drain insertion follows immediately after finger thoracostomy, with the caveat that the time and place of insertion must be consistent with the child’s overall clinical priorities. -

Difficulty in Management of Pneumothorax in an Octogenarian with Pulmonary Fibrosis
doi • 10.5578/tt.66527 Tuberk Toraks 2018;66(1):76-77 Geliş Tarihi/Received:03.02.2018 • Kabul Ediliş Tarihi/Accepted: 19.02.2018 Difficulty in management of pneumothorax in an octogenarian with pulmonary fibrosis 1 Shinichiro OKAUCHI 1 1 Division of Respiratory Medicine, Mito Medical Center, Tsukuba University, Hajime OSAWA Mito, Japan 1 Hiroaki SATOH 1 Tsukuba Üniversitesi Mito Tıp Merkezi, Solunum Bölümü, Mito, Japonya EDİTÖRE MEKTUP EDİTÖRE LETTER TO THE LETTER TO EDITOR Dear Editor, 23rd day (Figure 1-C). Two months after the removal of the chest tube, the respiratory condition of the patient Treatment of pneumothorax in patients with idiopathic does not deteriorate. pulmonary fibrosis (IPF) is often problematic. Especially in elderly patients with IPF, treatment of pneumothorax Pneumothorax is a common complication in IPF may often be unsuccessful due to unexpected compli- patients, who can present increased morbidity caused cations. We would like to share our experience in by exacerbation of the respiratory manifestations of the pneumothorax treatment in a very elderly patient with disease, which can lead to respiratory failure and death IPF. (1). Pneumothorax in patients with IPF, air leaks from complicatedly modified lungs are sustained, and pul- An 84-year-old man was referred to our hospital with monary re-expansion is difficult to achieve due to an exacerbation of dyspnea. Ten years prior to this contraction tendency. If the lungs are re-expanded, presentation, the patient was diagnosed with idiopath- fortunately, pleurodesis is a conceivable effective treat- ic pulmonary fibrosis (IPF) (Figure 1-A). In addition to ment, but this is also problematic. -

Delayed Tension Pneumothorax Complicating Staphylococcal Pneumonia S.P
Postgrad Med J: first published as 10.1136/pgmj.64.756.796 on 1 October 1988. Downloaded from Postgraduate Medical Journal (1988) 64, 796-798 Delayed tension pneumothorax complicating staphylococcal pneumonia S.P. Yates and S.K. Morcos Department of Radiodiagnosis and Imaging, Northern General Hospital, Herries Road, Sheffield S5 7AU, UK. Summary: A case is described in which a tension pneumothorax complicated staphylococcal pneumonia 11 months after its onset. The delayed and subacute/chronic nature of the tension pneumothorax is unusual. The case also highlights the difficult differential diagnosis between subpleural lung cysts and encysted pneumothorax. Introduction Staphylococcal pneumonia is fairly uncommon out- side hospitals, where it accounts for between 1 and 15% of acute pneumonias.1 2 It is rare for staphylococci to cause pneumonia in previously healthy individuals. Those who have viral lower ......i....:....l.- respiratory tract infections are predisposed, as are the immunocompromised.2 Pulmonary infection by copyright. may follow septicaemia due to distant focus of staphylococcal infection, but when this is the case the pattern tends to be one of discrete but multiple lung abscesses.3 The more usual pattern is that of a widespread bronchopneumonia, though occasio- nally the pneumonia can be confined to a single lobe or segment.4 Cavitation of the consolidated areas of the lung may occur and resolution of the pneumonia is generally complete, with little or no http://pmj.bmj.com/ scarring. Rupture of staphylococcal abscess cavities has been recognized as a cause of pneumothorax during the acute illness.3 The spread of sepsis to the pleural cavity can result in empyema and perma- nent damage to the pleura, with thickening and Figure 1 A chest radiograph demonstrates extensive adhesions. -

Subcutaneous Emphysema, Pneumothorax And
Published online: 2021-07-23 CASE REPORT Subcutaneous emphysema, pneumothorax and pneumomediastinum as a complication of an asthma attack Ana Isabel Franco, Sari Arponen, Fátima Hermoso1, María‑José García Internal Medicine Department and 1Thoracic Surgery Department, Hospital Universitario de Torrejón, Calle Mateo Inurria s/n, Torrejón de Ardoz, Spain Correspondence: Dr. Sari Arponen, Internal Medicine Department, Hospital Universitario de Torrejón, Calle Mateo Inurria s/n, Torrejón de Ardoz, Spain. E‑mail: [email protected] Abstract Introduction: Simultaneous subcutaneous emphysema, spontaneous pneumothorax, and pneumomediastinum are complications rarely observed synchronously during an acute exacerbation of bronchial asthma. Although spontaneous pneumothorax has already been reported in asthma patients in the literature, its concurrence with subcutaneous emphysema and pneumomediastinum is extremely rare except for iatrogenic conditions. Case Study: We describe a patient who presented to the emergency room with progressive dyspnea and chest pain. Three days before, she consulted her general physician with a history of violent dry cough and wheezing. An acute asthma exacerbation was diagnosed, and an inhaled short‑acting beta 2 agonist and oral prednisone were prescribed. The patient developed simultaneous subcutaneous emphysema, spontaneous pneumothorax, and pneumomediastinum, a rare complication of an asthma attack. Conclusions: Our aim is to emphasize that occult pneumothoraces should be considered in a patient presenting -
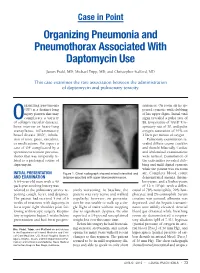
Organizing Pneumonia and Pneumothorax Associated with Daptomycin Use
Case in Point Organizing Pneumonia and Pneumothorax Associated With Daptomycin Use James Prahl, MD; Michael Tripp, MD; and Christopher Stafford, MD This case examines the rare association between the administration of daptomycin and pulmonary toxicity. rganizing pneumonia sentences. On room air he ap- (OP) is a distinct lung peared cyanotic with clubbing injury pattern that may of his upper digits. Initial vital Ocomplicate a variety signs revealed a pulse rate of of collagen vascular diseases, 88, temperature of 100.8º F, re- bone marrow or heart-lung spiratory rate of 30, and pulse transplants, inflammatory oxygen saturation of 91% on bowel disease (IBD), inhala- 2 liters per minute of oxygen. tion of toxic gases, vasculitis, Pulmonary examination re- or medications. We report a vealed diffuse coarse crackles case of OP complicated by a and rhonchi bilaterally. Cardiac spontaneous tension pneumo- and abdominal examinations thorax that was temporally re- were normal. Examination of lated to a prolonged course of the extremities revealed club- daptomycin. bing and mild digital cyanosis while the patient was on room INITIAL PRESENTATION Figure 1. Chest radiograph showed mixed interstitial and air. Complete blood count AND EXAMINATION airspace opacities with upper lobe predominance. demonstrated anemia, throm- A 64-year-old man with a 40 bocytosis, and a leukocytosis pack-year smoking history was of 12 x 103/µL with a differ- referred to the pulmonary service re- sively worsening. At baseline, the ential of 78% neutrophils, 20% lym- porting cough, fever, and dyspnea. patient was very active and walked phocytes, and 2% eosinophils. Serum The patient had received 5 out of 6 regularly; however, on presenta- creatine was normal, albumin was weeks of treatment with daptomycin tion he was unable to walk up a sin- depressed, and the hepatic transami- for a septic right shoulder joint fol- gle flight of stairs without stopping nases were mildly elevated. -

Pulmonary Hypertension in the Intensive Care Unit
Pulmonary vascular disease ORIGINAL ARTICLE Heart: first published as 10.1136/heartjnl-2015-307774 on 6 April 2016. Downloaded from Pulmonary hypertension in the intensive care unit. Expert consensus statement on the diagnosis and treatment of paediatric pulmonary hypertension. The European Paediatric Pulmonary Vascular Disease Network, endorsed by ISHLT and DGPK Michael Kaestner,1 Dietmar Schranz,2 Gregor Warnecke,3,4 Christian Apitz,1 Georg Hansmann,5 Oliver Miera6 For numbered affiliations see ABSTRACT heterogeneous underlying conditions.1 Distinction end of article. Acute pulmonary hypertension (PH) complicates the between precapillary and postcapillary aetiologies Correspondence to course of several cardiovascular, pulmonary and other (or establishment of a combination of the two) is Dr. Oliver Miera, Department systemic diseases in children. An acute rise of RV important to initiate specific individual therapy. of Congenital Heart Disease afterload, either as exacerbating chronic PH of different and Paediatric Cardiology, aetiologies (eg, idiopathic pulmonary arterial Pathophysiology of acute PH and RV failure Deutsches Herzzentrum Berlin, hypertension (PAH), chronic lung or congenital heart Augustenburger Platz 1, Chronic PH causes adaptation and remodelling of Berlin 13353, Germany; disease), or pulmonary hypertensive crisis after corrective the RV to increased loading conditions. Pulmonary [email protected] surgery for congenital heart disease, may lead to severe hypertensive crisis (PHC) occurs when compensatory circulatory compromise. Only few clinical studies provide mechanisms fail, RV systolic function decompensates This manuscript is a product of evidence on how to best treat children with acute severe and LV preload acutely decreases resulting in abol- the writing group of the 23 European Paediatric Pulmonary PH and decompensated RV function, that is, acute RV ished cardiac output and coronary perfusion. -

Imaging of Pulmonary Hypertension: an Update
296 Review Article Imaging of pulmonary hypertension: an update Harold Goerne1,2, Kiran Batra3, Prabhakar Rajiah3 1IMSS Centro Medico Nacional De Occidente, Guadalajara, Jalisco, Mexico; 2CID Imaging and Diagnostic Center, Guadalajara, Jalisco, Mexico; 3Radiology Department, UT Southwestern Medical Center, Dallas, Texas, USA Contributions: (I) Conception and design: H Goerne, P Rajiah; (II) Administrative support: H Goerne, P Rajiah; (III) Provision of study materials or patients: All authors; (IV) Collection and assembly of data: H Goerne, P Rajiah; (V) Data analysis and interpretation: H Goerne, P Rajiah; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Prabhakar Rajiah, MD. Associate Professor, Department of Radiology, Cardiothoracic Imaging, UT Southwestern Medical Center, E6.120 B, Mail code 9316, 5323 Harry Hines Boulevard, Dallas, TX 75390-8896, USA. Email: [email protected]. Abstract: Pulmonary hypertension (PH) is characterized by elevated pulmonary arterial pressure caused by a broad spectrum of congenital and acquired disease processes, which are currently divided into five groups based on the 2013 WHO classification. Imaging plays an important role in the evaluation and management of PH, including diagnosis, establishing etiology, quantification, prognostication and assessment of response to therapy. Multiple imaging modalities are available, including radiographs, computed tomography (CT), magnetic resonance imaging (MRI), nuclear medicine, echocardiography and