A BI-RADS Based Expert Systems for the Diagnoses of Breast Diseases
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Bukit Arang Tertiary Basin in Chuping, Perlis
GeoL. Soc. MaLaYJia, BuLLetin 42, December 1998; pp. 179-186 The Bukit Arang Tertiary Basin in Chuping, Perlis C.Y. LEE School of Physics Universiti Sains Malaysia 11800 USM Penang Abstract: The Bukit Arang Tertiary Basin extends from the Perlis-Thailand border at Bukit Arang Bukit Tinggi southwards to the Chuping area of eastern Perlis. It is part of the larger Sadao Basin located across the border in Thailand. Another southern extension of this main basin is found in the vicinity ofBukit Kayu Hitam, north of Changlun, just a few kilometres to the east across the interstate boundary in Kedah. Based on sparse geological evidence, the original postulated areal extent of the basin within Perlis was approximately 26 square kilometres with a minimum thickness of about 200 m. Recent gravity data indicate that it is at least twice as large in area and up to 800 m thick. The sediments consist ofloose and partially consolidated gravels, sands, silts and clays oflacustrine and fluvio-deltaic origin of Late Tertiary age. They are underlain by shales, mudstones and siltstones of the Kubang Pasu Formation of Carboniferous age. Geophysical evidence suggests that this basement is uneven, with a ridge-like feature in a north-south orientation. The basement appears to be faulted as well with WNW-ESE and approximately N-S strikes. Stratigraphically these Tertiary Beds can be correlated with the very similar strata of the Batu Arang Tertiary Basin of Late Oligocene to Late Miocene age in Selangor and with other Tertiary basins of similar lithology elsewhere in the peninsula. The Bukit Arang Tertiary Beds contain several seams of low quality coal of not much economic significance. -

Factors for Success of Sunnah Movement in Perlis State
International Journal of Academic Research in Business and Social Sciences Vol. 10, No. 4, April, 2020, E-ISSN: 2222-6990 © 2020 HRMARS Factors for Success of Sunnah Movement in Perlis State Abdul Ghafur Abdul Hadi and Basri Ibrahim To Link this Article: http://dx.doi.org/10.6007/IJARBSS/v10-i4/7137 DOI:10.6007/IJARBSS/v10-i4/7137 Received: 18 February 2020, Revised: 04 March 2020, Accepted: 26 March 2020 Published Online: 10 April 2020 In-Text Citation: (Hadi & Ibrahim, 2020) To Cite this Article: Hadi, A. G. A., & Ibrahim, B. (2020). Factors for Success of Sunnah Movement in Perlis State. International Journal of Academic Research in Business and Social Sciences, 10(4), 336–347. Copyright: © 2020 The Author(s) Published by Human Resource Management Academic Research Society (www.hrmars.com) This article is published under the Creative Commons Attribution (CC BY 4.0) license. Anyone may reproduce, distribute, translate and create derivative works of this article (for both commercial and non-commercial purposes), subject to full attribution to the original publication and authors. The full terms of this license may be seen at: http://creativecommons.org/licences/by/4.0/legalcode Vol. 10, No. 4, 2020, Pg. 336 - 347 http://hrmars.com/index.php/pages/detail/IJARBSS JOURNAL HOMEPAGE Full Terms & Conditions of access and use can be found at http://hrmars.com/index.php/pages/detail/publication-ethics 336 International Journal of Academic Research in Business and Social Sciences Vol. 10, No. 4, April, 2020, E-ISSN: 2222-6990 © 2020 HRMARS Factors for Success of Sunnah Movement in Perlis State Abdul Ghafur Abdul Hadi1 and Basri Ibrahim2 1Universiti Islam Malaysia, Cyberjaya, Malaysia, 2Universiti Islam Malaysia, Cyberjaya, Malaysia/ Faculty of Islamic Contemporary Studies, Universiti Sultan Zainal Abidin, Terengganu, Malaysia. -

(Cerbera Odollam) with Impregnation in Phosphoric Acid (H3PO4) A
Preparation and Characterization of Activated Carbon from the Sea Mango (Cerbera Odollam) with Impregnation in Phosphoric Acid (H3PO4) A. Nur Hidayah 1 M. A. Umi Fazara*,1 Z. Nor Fauziah 2 M. K. Aroua 3 1 School of Environmental Engineering, University Malaysia Perlis, Kompleks Pusat Pengajian Jejawi 3, 02600 Arau, Perlis, Malaysia. 2 Faculty of Engineering Technology, University Malaysia Perlis, Engineering Centre, 1st floor, Administration Building, Pauh Putra Main Campus, 02600 Arau, Perlis.. 3 Chemical Engineering Department, Faculty of Engineering, University of Malaya, 50603, Kuala Lumpur, Malaysia. *e-mail : [email protected] The properties of the activated carbon from Sea Mango (Cerbera Odollam) prepared from chemical and physical activation was studied. The sample was impregnated with phosphoric acid (H3PO4) at the impregnation ratio of precursor to activant as 1:2 and ° followed by thermal activation at 500 C with different flowing gas i.e. nitrogen (N2), carbon dioxide (CO2), steam and at the absent of any gases for duration of 2 hours. The sample experienced two different steps of preparation which were Method 1 and Method 2. In Method 1, the precursor will be thermally heated after the chemical activation process, and the samples were denoted as RIHM1-N, RIHM1-CO2, RIHM1-S and RIHM1-A which utilize either N2, CO2, steam and absent of any gases, respectively. Meanwhile in Method 2, the ° carbonization process with N2 flow at 200 C was done prior to chemical and thermal activation. This type of treatment method was denoted as RCIHM2-N, RCIHM2-CO2 RCIHM2-S and RCIHM2-A, which use the same flowing gases as described previously. -

Distribution and Analysis of Heavy Metals Contamination in Soil, Perlis, Malaysia
E3S Web of Conferences 34, 02040 (2018) https://doi.org/10.1051/e3sconf/20183402040 CENVIRON 2017 Distribution and Analysis of Heavy Metals Contamination in Soil, Perlis, Malaysia Ain Nihla Kamarudzaman1,*, Yee Shan Woo1, and Mohd Faizal Ab Jalil2 1School of Environmental Engineering, Universiti Malaysia Perlis, Kompleks Pusat Pengajian Jejawi 3, 02600 Arau, Perlis, Malaysia 2Perlis State Department of Environment, 2nd Floor, KWSP Building, Jalan Bukit Lagi, 01000 Kangar, Perlis, Malaysia Abstract. The concentration of six heavy metals such as Cu, Cr, Ni, Cd, Zn and Mn were studied in the soils around Perlis. The aim of the study is to assess the heavy metals contamination distribution due to industrialisation and agricultural activities. Soil samples were collected at depth of 0 – 15 cm in five stations around Perlis. The soil samples are subjected to soil extraction and the concentration of heavy metals was determined via ICP - OES. Overall concentrations of Cr, Cu, Zn, Ni, Cd and Mn in the soil samples ranged from 0.003 - 0.235 mg/L, 0.08 - 41.187 mg/L, 0.065 - 45.395 mg/L, 0.031 - 2.198 mg/L, 0.01 - 0.174 mg/L and 0.165 - 63.789 mg/L respectively. The concentration of heavy metals in the soil showed the following decreasing trend, Mn > Zn > Cu > Ni > Cr > Cd. From the result, the level of heavy metals in the soil near centralised Chuping industrial areas gives maximum value compared to other locations in Perlis. As a conclusion, increasing anthropogenic activities have influenced the environment, especially in increasing the pollution loading. -

Morphological Variability Identification of Harumanis Mango (Mangifera Indica L.) Harvested from Different Location and Tree Age
Morphological Variability Identification of Harumanis Mango (Mangifera indica L.) Harvested from Different Location and Tree Age Authors: Siti Nur Arina Yusuf, Ahmad Mukhlis Abdul Rahman, Zarina Zakaria, Vijay Kumar Subbiah, Maz Jamilah Masnan and Zakaria Wahab *Correspondence: [email protected] DOI: https://doi.org/10.21315/tlsr2020.31.2.6 Highlights • Fifty accessions of Harumanis harvested from different location and tree age were evaluated based on their morphological variation. • The result of Principal Component Analysis (PCA) provided a good approximation of the data which majorly contributed by parameters of weight, fruit dimensional characteristics, peel percentage and hue angle, h. • Preliminary screening of important morphological characteristics which contribute to the phenotypic diversity of Harumanis is successfully achieved. TLSR, 31(2), 2020 © Penerbit Universiti Sains Malaysia, 2020 Tropical Life Sciences Research, 31(2), 107–143, 2020 Morphological Variability Identification of Harumanis Mango (Mangifera indica L.) Harvested from Different Location and Tree Age 1Siti Nur Arina Yusuf, 1Ahmad Mukhlis Abdul Rahman*, 1Zarina Zakaria, 2Vijay Kumar Subbiah, 3Maz Jamilah Masnan and 4Zakaria Wahab 1Department of Chemical Engineering Technology, Faculty of Engineering Technology, Universiti Malaysia Perlis, Sungai Chuchuh, 02100 Padang Besar, Perlis, Malaysia 2Biotechnology Research Institute, Universiti Malaysia Sabah, Jalan UMS, 88400 Kota Kinabalu, Sabah, Malaysia 3Institute of Engineering Mathematics, Universiti Malaysia Perlis, Kampus Pauh Putra, 02600 Arau, Perlis, Malaysia 4Department of Mechanical Engineering Technology, Faculty of Engineering Technology, Universiti Malaysia Perlis, Sungai Chuchuh, 02100 Padang Besar, Perlis, Malaysia Publication date: 6 August 2020 To cite this article: Siti Nur Arina Yusuf, Ahmad Mukhlis Abdul Rahman, Zarina Zakaria, Vijay Kumar Subbiah, Maz Jamilah Masnan and Zakaria Wahab. -

Senarai Premis Yang Berjaya Mendapat Pensijilan (Mesti)
SENARAI PREMIS YANG BERJAYA MENDAPAT PENSIJILAN (MESTI) BIL NAMA SYARIKAT ALAMAT SYARIKAT NAMA WAKIL SYARIKAT NO TELEFON PRODUK LOT 19, JALAN INDUSTRI, KAWASAN PERINDUSTRIAN, 02000 Tel: 04-9853089 1 IGLOO ICE SDN BHD CHUA SHUI CHWN AIS KUALA PERLIS Faks: 04-9853122 2 RAROSYA ENTERPRISE 42 KAMPUNG BANGGOL SENA KANGAR RAFEDAH BINTI ISMAIL@MUSA 017-5121048 SOS CILI KOMPLEKS GERAK TANI WAWASAN E-1 (MADA) 02700 SIMPANG 3 PPK E-1 SIMPANG EMPAT EMPAT AL-HIDAYAH BT ALIAS 04-9807248 / 012-5883542 MINI POPIA PERLIS LOT 7 & 8, KAWASAN PERINDUSTRIAN MIEL JEJAWI FASA 2, 013-5846717 / 4 HPA INDUSTRIES SDN. BHD. A. ZAKARIA ABU BAKAR / NORASYIKIN KOPI RADIX, RADIX DIET JALAN JEJAWI SEMATANG, 02600 ARAU, PERLIS 019-6330727/049760741 5 SBA FOOD ENTERPRISE AB, JALAN KG SYED OMAR 01000 KANGAR SARIMAH BT ANI 017-5319490 REMPEYEK NO. 5&6, KAW PERINDUSTRIAN RINGAN, JALAN BESAR 02100 6 MEGA DUTAMAS SDN. BHD. TEOH YICK XIANG 017-4128967 COKLAT PADANG BESAR, PERLIS LOT A-5, KAWASAN MIEL, JEJAWI PHASE 1, 02600 JEJAWI, 019-4752188 7 ATLAS EDIBLE ICE SDN BHD LOW BEE BEE Ais tiub & Ais hancur PERLIS. 04-9777388 019-4907826 NO 2, 4 & 6, JALAN MURAI BATU, TAMAN KIM, 02100 PADANG 8 MEGA DUTAMAS SDN. BHD. YAP YUEN SER 04-9492788 COKLAT BESAR, PERLIS 04-9491788(F) 9 TERIAU ENTERPRISE NO 12 A KAMPUNG GUAR UJUNG BATU UTAN AJI 01000 KANGAR JAMINAH BT TERIAH 04-9766071 KACANG BERSALUT 109, LORONG SRI INAI, KAMPUNG JEJAWI DALAM 02600 ARAU 10 FAUZIAH BT ISMAIL FAUZIAH BINTI ISMAIL 017-4614385 REMPEYEK PERLIS LOT 555, JALAN BATAS LINTANG, 02700 SIMPANG EMPAT, 11 PERUSAHAAN PASTA ITIFAQ MOHD TARMIZIE ROMLI 017-5568953 MEE KUNING PERLIS 019-4549889 PERTUBUHAN PELADANG KAWASAN PAYA, KM 4 JALAN KAKI 12 PPK PAYA RAHMAH BT SALAMAT 04-9760280 CIP BUAH-BUAHAN BUKIT, 01000 KANGAR PERLIS 04-9761140 13 SYAFI BAKERY 500, JALAN MASJID KG. -

Asal Nama Negeri Perlis
Maklumat Lanjut DOSM/DOSM.PERLIS/1.2020/SIRI 84 Asal nama Negeri Perlis Nama Negeri Perlis dikatakan berasal daripada perkataan Siam prow-lowy yang bererti ‘kelapa hanyut’, daripada perkataan dialek Melayu Utara ‘perelus’ iaitu ‘kaki termasuk ke dalam atau ke celah sesuatu’, atau daripada nama Peran Leh yang dikatakan seorang peran atau pelawak mahsyur bernama Saleh. Selain itu, nama Perlis turut dikatakan bermula daripada perkataan ‘peroleh’ yang bermakna ‘mendapat, sempena nama pembesar bergelar Tok Perlis dan dikaitkan dengan ‘perlit’ yang bererti batu. Tambahan juga, Perlis juga biasa disebut sebagai Kayang. Nama Kayang ini dipendekkan bersempena nama Kota Indera Kayangan yang diasaskan oleh Sultan Dhiauddin Al-Mukarram Shah I berhampiran Kuala Sungai Perlis. Baginda adalah Sultan Kedah yang kelima belas dan memerintah dari tahun 1661 sehingga 1687. Sumber : Portal Rasmi Diraja Perlis Terletak di utara Semenanjung Malaysia dan 821km2 1 Pihak Berkuasa bersempadan dengan wilayah selatan Thailand Keluasan Tempatan (PBT) (Satun dan Songkhla), dengan keluasan hanya 821km2 (negeri terkecil di Malaysia) pentadbiran 3Parlimen Negeri Perlis diterajui oleh intitusi Diraja dan dibahagikan kepada 3 Parlimen iaitu, Kangar, 22Mukim Padang Besar dan Arau dengan pecahan 15 1Daerah Dewan Undangan Negeri dan mempunyai 22 15Dewan Pentadbiran Mukim. Selain daripada Wilayah Persekutuan Undangan Negeri Putrajaya dan Labuan, Perlis merupakan antara (DUN) negeri yang mempunyai hanya 1 Daerah Pentadbiran iaitu Perlis. 1 Evolusi Penduduk Perlis Evolusi Penduduk Perlis 2010 - 2020e (‘000) Pertumbuhan penduduk Negeri Perlis mulai260.0 1.6 254.0 254.9 255.0 253.5 1.4 tahun 2010 sehingga tahun 2020 secara 251.0 252.0 1.2 purata pada kadar 0.8 peratus setahun250.0. -

PERLIS 01000 Padang 1 TABIKA KEMAS BANGUNAN KHAS KG
Bil Nama Alamat Daerah Dun Parlimen Bil. Kelas JALAN SANTAN 01000 KANGAR PERLIS 01000 Padang 1 TABIKA KEMAS BANGUNAN KHAS KG. BONGKOK Perlis Santan 1 KANGAR Besar KG. TEBUK 02700 SIMPANG EMPAT PERLIS 02700 2 TABIKA KEMAS KG TEBUK Perlis Guar Sanji Arau 1 SIMPANG EMPAT 3 TABIKA KEMAS BANGUNAN JKR 01000 KANGAR PERLIS 01000 KANGAR Perlis Kayang Kangar 1 PERUMAHAN TAMAN EMAS JALAN BUKIT KETERI Padang 4 TABIKA KEMAS BANGUNAN KHAS TAMAN EMAS Perlis Beseri 1 02400 BESERI PERLIS 02400 BESERI Besar TABIKA KEMAS BANGUNAN KHAS BATU KG. BATU BERTANGKUP 02500 CHUPING PERLIS Padang 5 Perlis Chuping 1 BERTANGKUP 02500 CHUPING Besar TABIKA KEMAS BANGUNAN KHAS BATU KG. BATU BERTANGKUP 02500 CHUPING PERLIS Padang 6 Perlis Chuping 1 BERTANGKUP 2 02500 CHUPING Besar TABIKA KEMAS BANGUNAN KHAS BEREK POLIS TAMAN SERI AMAN JALAN SIMPANG EMPAT 7 Perlis Kayang Kangar 1 SERIAB 1 01000 KANGAR PERLIS 01000 KANGAR TABIKA KEMAS BANGUNAN KHAS BEREK POLIS TAMAN SERI AMAN JALAN SIMPANG EMPAT 8 Perlis Kayang Kangar 1 SERIAB 2 01000 KANGAR PERLIS 01000 KANGAR TABIKA KEMAS BANGUNAN KHAS FELDA MATA FELDA MATA AYER 02100 PADANG BESAR PERLIS Padang 9 Perlis Titi Tinggi 1 AYER 02100 PADANG BESAR Besar TABIKA KEMAS BANGUNAN KHAS FELDA RIMBA FELDA RIMBA MAS 02100 PADANG BESAR PERLIS Padang 10 Perlis Titi Tinggi 1 MAS 02100 PADANG BESAR Besar KEM UPP02100 PADANG BESAR (U) PERLIS 02100 Padang 11 TABIKA KEMAS BANGUNAN KHAS KEM UPP Perlis Titi Tinggi 1 PADANG BESAR Besar TABIKA KEMAS BANGUNAN KHAS KG BEHOR KG. BEHOR MASJID 01000 KANGAR PERLIS 01000 12 Perlis Kayang Kangar 1 MASJID KANGAR KG. -

Senarai Perlis
NO NAMA KEDAI NO PHONE ALAMAT MASJID BERHAMPIRAN DAERAH NEGERI ANUWARHAZLY BIN KASSIM NO 94. KAMPUNG TITI BESI, 02600 SURAU BILAL KAMPUNG UTAN PADANG 1 60125669210 PERLIS (MADA) ARAU PERLIS KANDIS 02600 ARAU PERLIS BESAR AYAM BISMI SDN BHD BOHOR BATU 1, 1/2 BATU HAMPAR, 2 60194196160 MASJID AL-ALA BOHOR TEMAK KANGAR PERLIS TEMAK BOHOR TEMAK 01000 KANGAR NO.9 TINGKAT BAWAH TAMAN AYAM BISMI SDN BHD TAMAN MASJID TUANKU SYED PUTRA 3 60197709060 INDERA, JALAN SEKOLAH DERMA KANGAR PERLIS INDERA JAMALULLAI L KANGAR 01000 KANGAR NO.3 TAMAN MELATI PERMAI, MASJID KAMPUNG PADANG LATI 4 AYUNI JAYA ENTERPRISE 60175835518 KANGAR PERLIS 02400 BESERI PERLIS 02400 KANGAR PERLIS NO24 TKT BAWAH, JALAN 5 AZHAR & FAMILY FRESH MART 6013450315 BERSERI INDAH, 02400, KANGAR MASJID AL HAKIM PADANG MALAU KANGAR PERLIS PERLIS 131 KAMPUNG BAHAGIA MASJID AL RAHMANIAH PEKAN 6 BHI BAHAGIA ENTERPRISE 60125731959 SEBERANG TOK PI, 02000 KUALA KANGAR PERLIS KUALA PERLIS 02000 KUALA PERLIS PERLIS, PERLIS NO 3 JALAN 1 TAMAN SRI MASJID SAIDINA OMAR AL- 7 DANTY MINI MARKET 60124730100 BAHAGIA, JALAN RAJA SYED ALWI KANGAR PERLIS KHATTAB 01000 KANGAR PERLIS NO 137B LORONG LUBUK BESAR BUKIT 8 DNUR MART ENTERPRSIE 60125583859 ULU KM 3 JALAN DATO KAYAMAN MASJID KAMPUNG SURAU PERLIS KETERI 02450 BUKIT KETERI PERLIS NO. 157 LOT 1382 JALAN MATA 9 DS MATA AYER ENTERPRISE 60124745043 MASJID MATA AIR AL -SYAKIRIN ARAU PERLIS AYER, 02500 ARAU PERLIS BERHADAPAN MASJID TELOK 10 ERIEYANA ENTERPRISE 60174049576 MASJID TELUK JAMBU KANGAR PERLIS JAMBU 01000 KANGAR PERLIS NO 9448 LOT KEDAI 3B -

The Preliminary Investigation on the Dredged Marine Sediment of Kuala Perlis As a Potential Brick Material
2012 2nd International Conference on Biotechnology and Environment Management IPCBEE vol. 42 (2012) © (2012) IACSIT Press, Singapore DOI: 10.7763/IPCBEE. 2012. V42. 6 The Preliminary Investigation on The Dredged Marine Sediment of Kuala Perlis as A Potential Brick Material W. S. Wan Salim 1 , N. A. Mohd Noor 2, S. F. Sadikon 1, M. F. Arshad 3, N. Wahid 4 and S. Mohd Salleh 1 1 Faculty of Civil Engineering, UiTM (Perlis), 02600 Arau Perlis 2 Faculty of Civil Engineering, UiTM (Pahang), Lintasan Semarak, 25600 Jengka Pahang, Malaysia 3 Faculty of Civil Engineering, UiTM Malaysia, 40450 Shah Alam Selangor, Malaysia 4 Faculty of Civil Engineering, UiTM (Pulau Pinang), 13500 Permatang Pauh Pulau Pinang, Malaysia Abstract. The marine sediment of estuary of Perlis River has to be dredged out of the basin to maintain the depth of ferry, boat and shipping channel. These dredged sediments were dumped back to the sea as marine disposal. However, these dump materials can come back to the river mouth depends on the wave flow where it possibly will contribute to the rapid sedimentation to the existing sediment brought by the river current. Consequently, the Marine Department which has authorities to maintain the water depth of harbour is burdened with high maintenance cost due to the frequent dredging activity. Therefore, it is important to introduce an alternative solution to manage the marine disposal other than dumping it back to the sea. Several experiments on physical and chemical properties were conducted to examine the suitability of marine sediments to be used as raw material in brick production. -

A Resistivity Survey for Groundwater in Perlis Using Offset Wenner Technique
Karat Water Resources (Proceedings of the Ankara - Antalya Symposium, July 1985). IAHSPubl.no. 161 A RESISTIVITY SURVEY FOR GROUNDWATER IN PERLIS USING OFFSET WENNER TECHNIQUE Mohammed Sayyadul Arafin and C.Y. Lee School of Physics, University Sains Malaysia Minden, Pulau Pinang, Malaysia. Abstract Vertical electrical soundings using the Offset Wenner array were carried out throghout Perlis, Peninsula Malaysia to investigate the hydrogeology of the state. The survey has been succesful in locating proper sites for drilling and in determining depths to bedrock. In some cases VES curves show quite clearly the presence of karstic limestone which is the potential source of grundwater in Perlis. Hydraulic transmissivities obtained from pumping tests of 15 boreholes have been correlated with the electrical transverse resistance corrected for porewater resistivity. It shows that an inverse non-linear relation, contrary to the direct relation reported elsewhere for sand and gravel aquifers, exists for karstic limestone aquifers in Perlis. This nonlinear inverse relationship may be useful for predicting aquifer trans- missivity in the area surveyed provided the electrolytic resistivity is known accurately. Introduction Inadequate supply of potable water in Perlis, Malaysia, has been a chronic problem for many years. Besides rapidly increasing demand for water due to urbanization, water is also necessary for agriculture as sugarcane and paddy are the main sources of income of the state. The aim of the present study is to investigate the hydrogeology of Perlis state by geophysical methods. Such investigation is important to the development of water supply and to construction engineering as well. The Irrigation Department has planned to construct two small dams - one north of Beseri and the other near Arau.This study also hopes to supply the Irrigation Department and Public Works Department with additional information regarding the subsurface and hydrogeologic parameters. -
Ant Colony Optimization for Predicting Flood Based on River Water Level
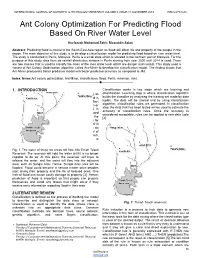
INTERNATIONAL JOURNAL OF SCIENTIFIC & TECHNOLOGY RESEARCH VOLUME 8, ISSUE 11, NOVEMBER 2019 ISSN 2277-8616 Ant Colony Optimization For Predicting Flood Based On River Water Level Nurfaezah Mohamad Zahir, Rizauddin Saian Abstract: Predicting flood is crucial in the South East Asia region as flood will affect life and property of the people in the region. The main objective of this study is to develop a classification model for predicting flood based on river water level. The study is conducted in Perlis, Malaysia. Perlis is a small state which is situated in the northern part of Malaysia. For the purpose of this study, data from six rainfall distribution stations in Perlis starting from year 2000 until 2014 is used. There are two classes that is used to classify the class of the river water level which are danger and normal. This study used a variant of Ant Colony Optimization algorithm called Ant-Miner to develop the classification model. The finding shows that Ant-Miner produced a better predictive model with better predictive accuracy as compared to J48. Index Terms:Ant colony optimization, Ant-Miner, classification, flood, Perlis, reservoir, river. ———————————————————— 1. INTRODUCTION Classification works in two steps which are learning and Many studies have been conducted to predict flood [1], [2], as classification. Learning step is where classification algorithm flood has terrible impacts on human being. Predicting flood is builds the classifier by analysing the training set made by data also crucial in the South East Asia region as flood will affect tuples. The data will be trained and by using classification life and property of the people in the region.