Pediatric Ophthalmology in the Emergency Department Kimball A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Artificial Intelligence for Pediatric Ophthalmology
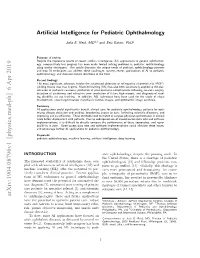
Artificial Intelligence for Pediatric Ophthalmology Julia E. Reid, MD m;y and Eric Eaton, PhDz Purpose of review Despite the impressive results of recent artificial intelligence (AI) applications to general ophthalmol- ogy, comparatively less progress has been made toward solving problems in pediatric ophthalmology using similar techniques. This article discusses the unique needs of pediatric ophthalmology patients and how AI techniques can address these challenges, surveys recent applications of AI to pediatric ophthalmology, and discusses future directions in the field. Recent findings The most significant advances involve the automated detection of retinopathy of prematurity (ROP), yielding results that rival experts. Machine learning (ML) has also been successfully applied to the clas- sification of pediatric cataracts, prediction of post-operative complications following cataract surgery, detection of strabismus and refractive error, prediction of future high myopia, and diagnosis of read- ing disability via eye tracking. In addition, ML techniques have been used for the study of visual development, vessel segmentation in pediatric fundus images, and ophthalmic image synthesis. Summary AI applications could significantly benefit clinical care for pediatric ophthalmology patients by opti- mizing disease detection and grading, broadening access to care, furthering scientific discovery, and improving clinical efficiency. These methods need to match or surpass physician performance in clinical trials before deployment with patients. Due to widespread use of closed-access data sets and software implementations, it is difficult to directly compare the performance of these approaches, and repro- ducibility is poor. Open-access data sets and software implementations could alleviate these issues, and encourage further AI applications to pediatric ophthalmology. Keywords pediatric ophthalmology, machine learning, artificial intelligence, deep learning INTRODUCTION atric ophthalmology, despite the pressing need. -
Aafp Fmx 2020
10/7/2020 Common Acute Eye Presentations Dr. Ahmed Mian HonBSc, BEd, MD CCFP (EM) Staff ER Consultant Department of Emergency Medicine, Humber River Hospital and University Health Network Medical Director and Chair, Medical Education HRH ED Investigative Coroner, Province of Ontario Faculty DFCM/EM University of Toronto and DFM Queens' University 1 ACTIVITY DISCLAIMER The material presented here is being made available by the American Academy of Family Physicians for educational purposes only. Please note that medical information is constantly changing; the information contained in this activity was accurate at the time of publication. This material is not intended to represent the only, nor necessarily best, methods or procedures appropriate for the medical situations discussed. Rather, it is intended to present an approach, view, statement, or opinion of the faculty, which may be helpful to others who face similar situations. The AAFP disclaims any and all liability for injury or other damages resulting to any individual using this material and for all claims that might arise out of the use of the techniques demonstrated therein by such individuals, whether these claims shall be asserted by a physician or any other person. Physicians may care to check specific details such as drug doses and contraindications, etc., in standard sources prior to clinical application. This material might contain recommendations/guidelines developed by other organizations. Please note that although these guidelines might be included, this does not necessarily imply the endorsement by the AAFP. 2 2 1 10/7/2020 Disclosure It is the policy of the AAFP that all individuals in a position to control content disclose any relationships with commercial interests upon nomination/invitation of participation. -

Endogenous Brucella Endophthalmitis: a Case Report
Saudi Journal of Ophthalmology (2017) xxx, xxx–xxx Case Report Endogenous Brucella endophthalmitis: A case report ⇑ Merih Oray a, ; Zafer Cebeci a; Nur Kir a; Banu Turgut Ozturk b; Lutfiye Oksuz c; Ilknur Tugal-Tutkun a Abstract Brucellosis may be associated with a wide range of ophthalmic manifestations including endophthalmitis, which is a sight- threatening condition that needs to be rapidly recognized and treated to avoid permanent visual loss. A 26-year-old female with a 6-month history of vision loss in the left eye was treated with high dose systemic corticosteroids and azathioprine with an initial misdiagnosis elsewhere. A dense vitreous haze with opacities at the posterior hyaloid and a wide area of retinochoroiditis led to the diagnosis of endogenous endophthalmitis at presentation to us. The vitreous sample and blood cultures demonstrated growth of Brucella melitensis. She received 6 months of systemic antibiotherapy, which resulted in resolution of inflammation; however, visual acuity remained poor due to irreversible damage. Infectious etiology, including brucellosis in endemic countries, has to be considered in the differential diagnosis before administering immunomodulatory therapy in patients with panuveitis of unknown origin. Keywords: Endogenous endophthalmitis, Ocular brucellosis, Panuveitis Ó 2017 The Authors. Production and hosting by Elsevier B.V. on behalf of Saudi Ophthalmological Society, King Saud University. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). http://dx.doi.org/10.1016/j.sjopt.2017.03.002 Introduction We herein present an unusual case of endogenous endophthalmitis due to B. melitensis. Brucellosis (Malta fever) is a zoonotic systemic disease caused by Brucella melitensis or Brucella abortus. -

Differentiate Red Eye Disorders
Introduction DIFFERENTIATE RED EYE DISORDERS • Needs immediate treatment • Needs treatment within a few days • Does not require treatment Introduction SUBJECTIVE EYE COMPLAINTS • Decreased vision • Pain • Redness Characterize the complaint through history and exam. Introduction TYPES OF RED EYE DISORDERS • Mechanical trauma • Chemical trauma • Inflammation/infection Introduction ETIOLOGIES OF RED EYE 1. Chemical injury 2. Angle-closure glaucoma 3. Ocular foreign body 4. Corneal abrasion 5. Uveitis 6. Conjunctivitis 7. Ocular surface disease 8. Subconjunctival hemorrhage Evaluation RED EYE: POSSIBLE CAUSES • Trauma • Chemicals • Infection • Allergy • Systemic conditions Evaluation RED EYE: CAUSE AND EFFECT Symptom Cause Itching Allergy Burning Lid disorders, dry eye Foreign body sensation Foreign body, corneal abrasion Localized lid tenderness Hordeolum, chalazion Evaluation RED EYE: CAUSE AND EFFECT (Continued) Symptom Cause Deep, intense pain Corneal abrasions, scleritis, iritis, acute glaucoma, sinusitis, etc. Photophobia Corneal abrasions, iritis, acute glaucoma Halo vision Corneal edema (acute glaucoma, uveitis) Evaluation Equipment needed to evaluate red eye Evaluation Refer red eye with vision loss to ophthalmologist for evaluation Evaluation RED EYE DISORDERS: AN ANATOMIC APPROACH • Face • Adnexa – Orbital area – Lids – Ocular movements • Globe – Conjunctiva, sclera – Anterior chamber (using slit lamp if possible) – Intraocular pressure Disorders of the Ocular Adnexa Disorders of the Ocular Adnexa Hordeolum Disorders of the Ocular -

2018 Department of Ophthalmology Chair Report
SAVE THE▼ DATE Department of 200 Ophthalmology Years www.NYEE.edu Anniversary SPECIALTY REPORT | FALL 2018 www.NYEE.edu Celebration Join us for 200 Years and Counting: Bicentennial Cocktail Celebration October 15, 2020 Research Breakthrough: The Plaza 768 5th Avenue Gene Transfer New York, NY Therapy Restores 200 Years and Counting: Ophthalmology Vision in Mice Symposium October 16, 2020 Stay tuned for details on tickets and registration information. Cover image: Slice of a central retina section showing all layers (ONL, INL, GCL). Red indicates rod photoreceptors, located in outer nuclear layer (ONL). Green indicates Müller glial cells, whose cell bodies are located in inner nuclear layer (INL), and their branches across all three layers. Dark blue indicates the nucleus of all cells in three layers (GCL). Icahn School of Medicine at Medical Directors Neuro-Ophthalmology Uveitis and Ocular Immunology Mount Sinai Departmental Mark Kupersmith, MD Douglas Jabs, MD, MBA Avnish Deobhakta, MD Leadership System Chief, System Chief, Uveitis and Ocular Medical Director, NYEE - Neuro-Ophthalmology, Immunology, MSHS James C. Tsai, MD, MBA East 85th Street MSHS President, NYEE Stephanie Llop, MD System Chair, Department of Robin N. Ginsburg, MD 3 Message From the System Chair of the DepartmentValerie Elmalem, of Ophthalmology MD Sophia Saleem, MD Ophthalmology, MSHS Medical Director, NYEE- Joel Mindel, MD East 102nd Street Louis4 R. Pasquale,Breaking MD New Ground in Gene Transfer Therapy to Restore Vision Affiliated Leadership Ocular Oncology Site Chair, Department of Gennady Landa, MD Paul Finger, MD Ebby Elahi, MD, MBA Ophthalmology, MSH and MSQ Medical Director, NYEE- 6 This i-Doctor Is Transforming the Field of Ophthalmology President, NYEE/MSH System Vice Chair, Translational Williamsburg and Tribeca Ophthalmic Pathology Ophthalmology Alumni Ophthalmology Research, MSHS Jodi Sassoon, MD Society Kira Manusis, MD Inside Feature Site Chair, Pathology, NYEE Medical Director, NYEE- Paul A. -

Eyelid and Orbital Infections
27 Eyelid and Orbital Infections Ayub Hakim Department of Ophthalmology, Western Galilee - Nahariya Medical Center, Nahariya, Israel 1. Introduction The major infections of the ocular adnexal and orbital tissues are preseptal cellulitis and orbital cellulitis. They occur more frequently in children than in adults. In Schramm's series of 303 cases of orbital cellulitis, 68% of the patients were younger than 9 years old and only 17% were older than 15 years old. Orbital cellulitis is less common, but more serious than preseptal. Both conditions happen more commonly in the winter months when the incidence of paranasal sinus infections is increased. There are specific causes for each of these types of cellulitis, and each may be associated with serious complications, including vision loss, intracranial infection and death. Studies of orbital cellulitis and its complication report mortality in 1- 2% and vision loss in 3-11%. In contrast, mortality and vision loss are extremely rare in preseptal cellulitis. 1.1 Definitions Preseptal and orbital cellulites are the most common causes of acute orbital inflammation. Preseptal cellulitis is an infection of the soft tissue of the eyelids and periocular region that is localized anterior to the orbital septum outside the bony orbit. Orbital cellulitis ( 3.5 per 100,00 ) is an infection of the soft tissues of the orbit that is localized posterior to the orbital septum and involves the fat and muscles contained within the bony orbit. Both types are normally distinguished clinically by anatomic location. 1.2 Pathophysiology The soft tissues of the eyelids, adnexa and orbit are sterile. Infection usually originates from adjacent non-sterile sites but may also expand hematogenously from distant infected sites when septicemia occurs. -

A Patient & Parent Guide to Strabismus Surgery
A Patient & Parent Guide to Strabismus Surgery By George R. Beauchamp, M.D. Paul R. Mitchell, M.D. Table of Contents: Part I: Background Information 1. Basic Anatomy and Functions of the Extra-ocular Muscles 2. What is Strabismus? 3. What Causes Strabismus? 4. What are the Signs and Symptoms of Strabismus? 5. Why is Strabismus Surgery Performed? Part II: Making a Decision 6. What are the Options in Strabismus Treatment? 7. The Preoperative Consultation 8. Choosing Your Surgeon 9. Risks, Benefits, Limitations and Alternatives to Surgery 10. How is Strabismus Surgery Performed? 11. Timing of Surgery Part III: What to Expect Around the Time of Surgery 12. Before Surgery 13. During Surgery 14. After Surgery 15. What are the Potential Complications? 16. Myths About Strabismus Surgery Part IV: Additional Matters to Consider 17. About Children and Strabismus Surgery 18. About Adults and Strabismus Surgery 19. Why if May be Important to a Person to Have Strabismus Surgery (and How Much) Part V: A Parent’s Perspective on Strabismus Surgery 20. My Son’s Diagnosis and Treatment 21. Growing Up with Strabismus 22. Increasing Signs that Surgery Was Needed 23. Making the Decision to Proceed with Surgery 24. Explaining Eye Surgery to My Son 25. After Surgery Appendix Part I: Background Information Chapter 1: Basic Anatomy and Actions of the Extra-ocular Muscles The muscles that move the eye are called the extra-ocular muscles. There are six of them on each eye. They work together in pairs—complementary (or yoke) muscles pulling the eyes in the same direction(s), and opposites (or antagonists) pulling the eyes in opposite directions. -

Pediatric Ophthalmology/Strabismus 2017-2019
Academy MOC Essentials® Practicing Ophthalmologists Curriculum 2017–2019 Pediatric Ophthalmology/Strabismus *** Pediatric Ophthalmology/Strabismus 2 © AAO 2017-2019 Practicing Ophthalmologists Curriculum Disclaimer and Limitation of Liability As a service to its members and American Board of Ophthalmology (ABO) diplomates, the American Academy of Ophthalmology has developed the Practicing Ophthalmologists Curriculum (POC) as a tool for members to prepare for the Maintenance of Certification (MOC) -related examinations. The Academy provides this material for educational purposes only. The POC should not be deemed inclusive of all proper methods of care or exclusive of other methods of care reasonably directed at obtaining the best results. The physician must make the ultimate judgment about the propriety of the care of a particular patient in light of all the circumstances presented by that patient. The Academy specifically disclaims any and all liability for injury or other damages of any kind, from negligence or otherwise, for any and all claims that may arise out of the use of any information contained herein. References to certain drugs, instruments, and other products in the POC are made for illustrative purposes only and are not intended to constitute an endorsement of such. Such material may include information on applications that are not considered community standard, that reflect indications not included in approved FDA labeling, or that are approved for use only in restricted research settings. The FDA has stated that it is the responsibility of the physician to determine the FDA status of each drug or device he or she wishes to use, and to use them with appropriate patient consent in compliance with applicable law. -

Frequency of Common Factors Leading to Leukocoria in Pediatric Age Group at Tertiary Care Eye Hospital: an Observational Study
Biostatistics and Biometrics Open Access Journal ISSN: 2573-2633 Research Article Biostat Biometrics Open Acc J Faisal’s Issue - January 2018 Copyright © All rights are reserved by Muhammad Faisal Fahim DOI: 10.19080/BBOAJ.2018.04.555636 Frequency of Common Factors Leading to Leukocoria in Pediatric Age Group at Tertiary Care Eye Hospital: An Observational Study Rizwana Dargahi1, Abdul Haleem1, Darikta Dargahi S1 and Muhammad Faisal Fahim2* 1Department of Ophthalmology, Shaheed Mohtarma Benazir Bhutto Medical University, Pakistan 2Department of Research & Development, Al-Ibrahim Eye Hospital, Pakistan Submission: November 27, 2017; Published: January 19, 2018 *Corresponding author: Muhammad Faisal Fahim, M.Sc. (Statistics), Statistician, Department of Research & Development, Al-Ibrahim Eye Hospital, Isra postgraduate Institute of Ophthalmology, Karachi, Pakistan, Tel: ; Email: Abstract Objective: To know the frequency of common factors leading to leukocoria in pediatric age group at a tertiary care eye hospital. Materials & methods: This was across sectional observational study carried out at Pediatric department, Al-Ibrahim eye hospital Karachi from February to July 2016. All patients younger than 10 years who presented with leukocoria were included. The excluding criteria were previous history of trauma and ocular surgery. Systemic as well as ocular examination and relevant investigations was done to know cause of was used to analyzed data. leukocoria. B. Scan was done in all the cases. If needed X-ray chest, CT scan & MRI orbit was done for confirming diagnosis. SPSS version 20.0 Results: In our country congenital cataract is the most common cause of leukocoria which comprises about 77.3% (133/172) which is treatable. 2nd common cause was persistent fetal vasculature comprises 8.1% (14/172). -

UCSF Ophthalmology Advice Guide Authors: Seanna Grob, MD, MAS
UCSF Ophthalmology Advice Guide Authors: Seanna Grob, MD, MAS and Neeti Parikh, MD Hello! We are excited that you are interested in ophthalmology! It is truly a special field in medicine. From saving someone’s vision after severe eye trauma, to restoring vision with cataract, retina, or cornea surgery, to preserving someone’s vision with glaucoma management and surgery, to reconstructing someone’s periocular area after trauma, burns, or tumor removal, amazing things can happen in ophthalmology. Ophthalmologists love their job and the majority say they would pick this specialty again if they had the choice. An incredible amount of job satisfaction comes from saving someone’s vision! We are here for you in the UCSF Department of Ophthalmology! We have put together this guide to help you through the process. This guide is meant to be very comprehensive. We want to make sure you are aware of all the opportunities and resources you have so that you can plan accordingly. You do not have to do everything we mention! Please feel free to reach out with questions about the specialty, how to get involved, and how to become a great ophthalmology applicant! 1 Medical School A well-rounded application is important for a successful match and any way you can prove to ophthalmology programs that you are dedicated to the field will be helpful to you. As more objective data (such as grades and board scores become less prevalent) other parts of your application will become more important. Various experiences you seek out are not only fun and educational, but will offer exposure to this wonderful field. -

Clinical Characteristics and Outcomes of Paediatric Orbital Cellulitis in Hospital Universiti Sains Malaysia: a Five-Year Review
Singapore Med J 2020; 61(6): 312-319 Original Article https://doi.org/10.11622/smedj.2019121 Clinical characteristics and outcomes of paediatric orbital cellulitis in Hospital Universiti Sains Malaysia: a five-year review Ismail Mohd-Ilham1,2, MBBS, MMed, Abd Bari Muhd-Syafi1,2, MBBS, Sonny Teo Khairy-Shamel1,2, MD, MMed, Ismail Shatriah1,2, MD, MMed INTRODUCTION Limited data is available on paediatric orbital cellulitis in Asia. We aimed to describe demographic data, clinical presentation, predisposing factors, identified microorganisms, choice of antibiotics and management in children with orbital cellulitis treated in a tertiary care centre in Malaysia. METHODS A retrospective review was performed on children with orbital cellulitis aged below 18 years who were admitted to Hospital Universiti Sains Malaysia, Kelantan, Malaysia, between January 2013 and December 2017. RESULTS A total of 14 paediatric patients fulfilling the diagnostic criteria for orbital cellulitis were included. Their mean age was 6.5 ± 1.2 years. Boys were more likely to have orbital cellulitis than girls (71.4% vs. 28.6%). Involvement of both eyes was observed in 14.3% of the patients. Sinusitis (28.6%) and upper respiratory tract infection (21.4%) were the most common predisposing causes. Staphylococcus aureus (28.6%) was the leading pathogen. Longer duration of hospitalisation was observed in those infected with methicillin-resistant Staphylococcus aureus and Burkholderia pseudomallei. 10 (71.4%) patients were treated with a combination of two or three antibiotics. In this series, 42.9% had surgical interventions. CONCLUSION Young boys were found to be more commonly affected by orbital cellulitis than young girls. -

Albinism Terminology
Albinism Terminology Oculocutaneous Albinism (OCA): Oculocutaneous (pronounced ock-you-low-kew- TAIN-ee-us) Albinism is an inherited genetic condition characterized by the lack of or diminished pigment in the hair, skin, and eyes. Implications of this condition include eye and skin sensitivities to light and visual impairment. Ocular Albinism (OA): Ocular Albinism is an inherited genetic condition, diagnosed predominantly in males, characterized by the lack of pigment in the eyes. Implications of this condition include eye sensitivities to light and visual impairment. Hermansky Pudlak Syndrome (HPS): Hermansky-Pudlak Syndrome is a type of albinism which includes a bleeding tendency and lung disease. HPS may also include inflammatory bowel disease or kidney disease. The severity of these problems varies much from person to person, and the condition can be difficult to diagnose with traditional blood tests Chediak Higashi Syndrome: Chediak Higashi Syndrome is a type of albinism in which the immune system is affected. Illnesses and infections are common from infancy and can be severe. Issues also arise with blood clotting and severe bleeding. Melanin: Melanin is pigment found in a group of cells called melanocytes in most organisms. In albinism, the production of melanin is impaired or completely lacking. Nystagmus: Nystagmus is an involuntary movement of the eyes in either a vertical, horizontal, pendular, or circular pattern caused by a problem with the visual pathway from the eye to the brain. As a result, both eyes are unable to hold steady on objects being viewed. Nystagmus may be accompanied by unusual head positions and head nodding in an attempt to compensate for the condition.