The Best of the Oaracle: a Compilation of Articles from 2002-2007 Published by the Organization for Autism Research
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Journal of Precision Teaching and Celeration Volume 18, Issue 2
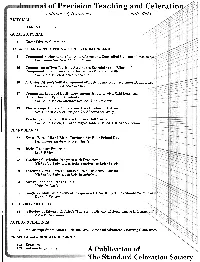
nal of Precision Teaching and Celeratio Volume 18, Number 2 Fall 2002 1 Editor's Comments i;i. GUEST EDITORIAL 2 Guest Editors' Comments rQ! : RESEARCH AND APPLICATION ARTICLES FROM IRELAND 6,' [, . 3 Compound Performance: The Role of Free and Controlled Operant Co 1,:I' .. ! % Philomena Smyth &Michael Keenan 16 Comparison of Two Teaching Structures Examining the Effects of Component Fluency on the Performance of Related Skills Claire McDowell &Michael Keenan 30 A Senior Citizen's Self-Management of Positive and Negative Inner Beha Emma E Cobane &Michael Keenan 37 Comparing Levels of Dysfluency Among Students with Mild Learning Difficulties and Qpical Students Claire McDowell, Michael Keenan &Ken l? Kerr 49 The Saplings Model of Education: Case Studies in Autism Ken l? Kerr, Audrey Campbell & Shauna McGrory 61 Teaching Component Skills to Improve Golf Swing Claire McDowell, Chris Mclntyre, Robert Bones & Michael Keenan CHART SHARES 67 Evan's Rate of Hand-Biting During a Six-Hour School Day Philomena Smyth & Nicola Hardy 69 Rick's Reading Progress Leah White 78 Tracking Curricular Progress with Precision Michael A. Fabrizio, Kristin Schrimer & Kelly Ferris 80 Teaching Visual Pattern Imitation to a Child with Autism Michael A. Fabrizio &Kristin Schrimer 83 Anna's Food and Stroke Chart Malcolm Neely 86 Single vs. Multiple Movement Frequencies: How Many Times Should We Dana J. Stevens DISCUSSION ARTICLES 88 A Review of Edward R. Tufte's 'The Visual Display of Quantitative In John W Eshleman AUTHOR GUIDELINES 95 Manuscript Submission Guidelines and Basic and Advanced Charting Guidelines ERRATUM and ACKNOWLEDGEMENTS 102 Erratum 103 Acknowledgements A Publication of .-*T.p I -TheStandard Celeration Society JournaI of Precision Teaching and Celeration Editor: RICHARD M. -

Journal of Precision Teaching and Celeration Volume 13, Issue 1
Journal of Precision Teaching and Celeration Volume Xlll Fa11 1995 Number 1 Ten Products of Fluency Ogden R. Lindsley Lindsley 's Unteaching Citation Ogden R. Lindsley ' Visual Imagery and Structure Words: Julie Spaulding, Manfred Accelerating Number of Words and W.Haerte1, Randy L. Seevers, & Number of Descriptive Words Written John 0.Cooper During Free Writing Use of Error Drill, Feedback, Praise, Lisa DeAngelis, T. F. McLaughlin, and Fading to Increase the Legibility of & William J. Sweeney D'Nealian Handwriting with Two Special Education Students The Effect of Music on Head Posturing V. Timmons, T. F. McLaughlin, of a Student with Cerebral Palsy: & V. Kinakin A Case Study Using Precision Teaching to Enhance Michele Morrell, Robert Mouell, Direct Instruction Sight-Word Reading & Richard M. Kubina Jr. Use of Daily Measurement, Standard Susan Abba & T. F. McLaughlin Celeration Charting, and a Nicotrol Patch to Reduce Cigarette Smoking with a Female College Student: A Case Study The Effects of Precision Teaching Christine Bashore & and a Token Economy on Handwriting T. F. McLaughlin Skills: A Case Study Notes From Below the Floor: The National Debt Abigail B. Calkin PT Data Lands in Fiction Abigail B. Calkin A Publication of The Standard Celeration Society The Journal of Precision Teaching and Celeration (ISSN 0271-8200) is a multidisciplinary journal that is dedicated to a science of human behavior which includes direct, continuous and standard measurement. This measurement includes a standard unit of behavior, frequency; a standard scale on which successive frequencies are displayed, the Standard Celeration Chart; a standard measure of behavior change between two frequencies, frequency multiplier, and a standard, straight-line measure of behavior change across seven or more frequencies, celeration. -
A Study and Demonstration of the Training and Utilization of Psychological Assistants in Different Clinical Settings
DOCUMENT RESUME ED 086 581 r SO 006 753 AUTHOR EcCaulley, Mary H. TITLE A Study and Demonstration of the Training and Utilization of Psychological Assistants in Different Clinical Settings. Final Report. INSTITUTION Florida Univ., Gainesville. Dept. of Clinical Psychology. SPONS AGENCY Public Health Service (DREW), Arlington, Va. Bureau of Health Manpower. REPORT NO PH-108-66-209 PUB DATE Apr 69 NOTE 316p. EDRS PRICE MP-80.65 HC-$13.16 DESCRIPTORS Career Ladders; *Clinical Experience; College Graduates; Demonstration Projects; Educational Programs; *Health Occupations; Health Personnel; Job Placement; Job Training; Manpower Development; *Manpower Utilization; On the Job Training; *Psychology; *Subprofessionals; Summative Evaluation; Technical Occupations IDENTIFIERS *Clinical Psychology ABSTRACT The training program described in this final report is one of a number of attempts to solve the manpower shortage in psychology. The task proposes to demonstrate that the presence of psychological assistants, in this case seven female college graduates, increases the effectiveness and productivity of the clinical psychologists to whom they are assigned in varying positions in clinical service and research. Background information on manpower status in psychology and allied professions introduces the report. Requirement and selection of participants are described. The . assistants are trained by a combination of methods, described and evaluated in Part IV, the most important appearing to be the apprenticeship on the setting. Contributions of the assistant in each setting are presented with a composite description of an assistant's duties. Placement of the assistants at the end of the project is dealt with in relation to initial expectations and changing attitudes as the program progresses. -

Cognitive-Behavioral Therapy Boundless
Cognitive-Behavioral Therapy Boundless Cognitive Therapy Cognitive therapy seeks to help a client overcome difficulties by identifying and changing dysfunctional thought patterns. 1. fig. 1 shows a group cognitive therapy session Clinicians use therapy sessions to help clients address and change their negative cognitive biases. Cognitive therapy (CT) is one of the therapeutic approaches within the larger group of cognitive behavioral therapies (CBT) and was first expounded by Aaron T. Beck in the 1960s. Cognitive-based therapies have gained increasing use in the past several decades, beginning with the cognitive revolution in 1956. CT is a psychotherapy quite distinct from other mainstream forms such as psychoanalytic or behavioral psychotherapy: rather than focusing on motivations or instincts, it is based on an information-processing model of human behavior and psychopathology. Cognitive distortions, or exaggerated and irrational thoughts, were believed to perpetuate psychological disorders. The process of learning to refute these distortions is called cognitive restructuring. Cognitive therapy may consist of testing a client's assumptions and identifying how client's unquestioned thoughts are distorted, unrealistic and unhelpful. Once these thoughts have been challenged, the client's feelings about the subject matter of those thoughts can be more readily changed. Cognition: Any element of knowledge including attitude, emotion, belief, or behavior. Schema: A person's worldview; an outline or image universally applicable to a general conception, under which it is likely to be presented to the mind Source URL: https://www.boundless.com/psychology/psychological-therapies/cognitive-behavioral-therapy/ Saylor URL: http://www.saylor.org/courses/psych404/ Attributed to: [Boundless] www.saylor.org Page 1 of 20 Cognitive Distortion: Exaggerated and irrational thoughts, believed to perpetuate psychological disorders. -

Conduct Research
1 www.onlineeducation.bharatsevaksamaj.net www.bssskillmission.in “Consultation”. In Section 1 of this course you will cover these topics: Introduction And Overview Of The Book Counseling And Consultation The Context Of Consultation Topic : Introduction And Overview Of The Book Topic Objective: At the end of this topic student would be able to: Gain a complete overview on the contents of this book Definition/Overview: Group Process Consultation: consists of activities designed to increase group awareness and understanding, so that the group or organization can take steps to improve the way that its members work together. Health psychology: is concerned with understanding how biology, behavior, and social context influence health and illness. Health psychologists work alongside other medical professionals in clinical settings, work on behavior change in public health promotion, teach at universities, andWWW.BSSVE.IN conduct research. Scientific Method: refers to techniques for investigating phenomena, acquiring new knowledge, or correcting and integrating previous knowledge. To be termed scientific, a method of inquiry must be based on gathering observable, empirical and measurable evidence subject to specific principles of reasoning. Key Points: 1. Introduction This Topic is an introduction to consultation and an overview of the book topic by topic. As is the case in consultation, it is important for students to have an understanding of what they will experience during the reading process. The author also found it important to provide www.bsscommunitycollege.in www.bssnewgeneration.in www.bsslifeskillscollege.in 2 www.onlineeducation.bharatsevaksamaj.net www.bssskillmission.in some explanation of the flow of the book. The first part of this topic describes consultation and serves to orient the reader to what lies ahead. -

University Microfilms 300 North Zeeb Road Ann Arbor, Michigan 48106 a Xarox Education Company 73-11,490 I
INFORMATION TO USERS This dissertation was produced from a microfilm copy of the original document. While the most advanced technological means to photograph and reproduce this document have been used, the quality is heavily dependent upon the quality of the original submitted. The following explanation of techniques is provided to help you understand markings or patterns which may appear on this reproduction. 1. The sign or "target" for pages apparently lacking from the document photographed is "Missing Page(s)". If it was possible to obtain the missing page(s) or section, they are spliced into the film along with adjacent pages. This may have necessitated cutting thru an image and duplicating adjacent pages to insure you complete continuity. 2. When an image on the film is obliterated with a large round black mark, it is an indication that the photographer suspected that the copy may have moved during exposure and thus cause a blurred image. You will find a good image of the page in the adjacent frame. 3. When a map, drawing or chart, etc., was part of the material being photographed the photographer followed a definite method in "sectioning" the material. It is customary to begin photoing at the upper left hand corner of a large sheet and to continue photoing from left to right in equal sections with a small overlap. If necessary, sectioning is continued again — beginning below the first row and continuing on until complete. 4. The majority of users indicate that the textual content is of greatest value, however, a somewhat higher quality reproduction could be made from "photographs" if essential to the understanding of the dissertation. -

7E5ed7cd6d30570ca8a7bd54ef
1 www.onlineeducation.bharatsevaksamaj.net www.bssskillmission.in “Introduction to Educational Psychology”. In Section 1 of this course you will cover these topics: Educational Psychology: Developing A Professional Knowledge Base The Development Of Cognition And Language Personal, Social, And Emotional Development Group And Individual Differences Topic : Educational Psychology: Developing A Professional Knowledge Base Topic Objective: At the end of this topic student would be able to: Explain Educational psychology Explain Social, moral and cognitive development Explain Individual differences and disabilities Explain Learning and cognition Explain Behavioral perspective Explain Cognitive perspective Explain Social cognitive perspective Explain Constructivist perspective Explain Motivation Explain Research methodology Explain QuantitativeWWW.BSSVE.IN methods Explain Qualitative methods Explain Applications in instructional design and technology Explain Applications in teaching Explain Careers in educational psychology Explain Employment outlook Definition/Overview: Educational psychology: Educational psychology is the study of how humans learn in educational settings, the effectiveness of educational interventions, the psychology of teaching, and the social psychology of schools as organizations. Although the terms "educational psychology" and "school psychology" are often used interchangeably, www.bsscommunitycollege.in www.bssnewgeneration.in www.bsslifeskillscollege.in 2 www.onlineeducation.bharatsevaksamaj.net www.bssskillmission.in -

Report of the HEW Work Group on Behavior Analysis in Education
MICROCOPY RESOLUTION TEST CHART NA1141k_BUREAUJOrzSTANDARDS41963:A DOCUMENT RESUME 'ED 079 233 SP 006 614- AUTHOR Stern, Joyce D. TITLE Report of the HEW Work,Group on Behavior Analysis in Education. Final Draft. INSTITUTION Department of Health, Education, and Welfare, Washington, D.C...Office of the AssiStant Secretary for Planning. and Evaluation. PUB DATE Jan 73 NOTE 178p. EDRS PRICE MF-$0.65 HC-$6.58 DESCRIPTORS -*Behavior; *Behavioral Science Research; *Behavior Change; Behavior Patterns; *Behavior Theories; Research Projects; Student Behavior; Teacher Behavior IDENTIFIERS Department of Health Education and Welfare 'ABSTRACT The Work Group on Behavior Modification in Education, which issued this report, was authorized by Secretary Elliot Richardson'on November 21, 1970._The body of this report includes an analysis of the benefits- of behavior modification techniques in education, examples of their successful appliCation with a variety of large student populations, an examination of the problems raised by the approach,- an assessment of its readiness to receive widespread promotion, and recommendations of possible next steps that could be taken. by U:S. Meliartment of Health,-Education and Welfare and the Office of Education relative to further-research.and dissemination. There are'four-appendixes; Appendix A'contains a list of'general references of basic literature in the discipline; Appendix B provides an overview of behavior_modification_activitieS in the range of. educational settings; Appendix C lists selected materials available for instructing parents and teachers in behavior analysis techniques; and Appendix D consists of detailed reports of 15 major centers of activity in behavior modification, (Author/JA3 FILMED FROM-BEST AVAILABLECOPY FINAL DRAFT U S DEPARTMENT OF HEALTH. -
Emotional Agility: Get Unstuck, Embrace Change and Thrive In
Susan David E M O T I O N A L A G I L I T Y Get Unstuck, Embrace Change, and Thrive in Work and Life Contents 1. Rigidity to Agility 2. Hooked 3. Trying to Unhook 4. Showing Up 5. Stepping Out 6. Walking Your Why 7. Moving On: The Tiny Tweaks Principle 8. Moving On: The See-Saw Principle 9. Emotional Agility at Work 10. Raising Emotionally Agile Children 11. Conclusion: Becoming Real Endnotes Acknowledgements Follow Penguin ABOUT THE AUTHOR Susan David PhD is a psychologist on the faculty of Harvard Medical School, co-founder and co-director of the Institute of Coaching at McLean Hospital, and CEO of Evidence Based Psychology, a boutique business consultancy. An in-demand speaker and advisor, Susan has consulted to the senior leadership of hundreds of major international organizations, including Ernst & Young, the United Nations and World Economic forum. Her work has featured in numerous publications, including the Harvard Business Review, Time, Fast Company and the Wall Street Journal. Susan has a PhD in clinical psychology and a post doctorate in emotions from Yale University. To the love of my life, Anthony Samir, & to my darlings, Noah and Sophie, who know how to dance each and every day. 1. Rigidity to Agility Years ago, in the Downton Abbey era, a well-regarded captain stood on the bridge of a British battleship watching the sun set across the sea. As the story goes, the captain was about to head below for dinner when suddenly a lookout announced, ‘Light, sir. Dead ahead two miles.’ The captain turned back toward the helm. -

Elements of Change 6. Behavioral Therapy 6.1
ELEMENTS OF CHANGE 6. BEHAVIORAL THERAPY 6.1. Background Behavioral therapy is a form of therapy rooted in the principles of behaviorism. The school of thought known as behaviorism is focused on the idea that we learn from our environment. In behavioral therapy, the goal is to reinforce desirable behaviors and eliminate unwanted or maladaptive ones. The techniques used in this type of treatment are based on the theories of classical conditioning and operant conditioning. One important thing to note about the various behavioral therapies is that unlike some other types of therapy that are rooted in insight (such as psychoanalytic and humanistic therapies), behavioral therapy is action based. Behavioral therapists are focused on using the same learning strategies that led to the formation of unwanted behaviors as well as other new behaviors. Because of this, behavioral therapy tends to be highly focused. The behavior itself is the problem, and the goal is to teach clients new behaviors to minimize or eliminate the issue. Old learning led to the development of a problem, and so the idea is that new learning can fix it. The first use of the term behavior modification appears to have been by Edward Thorndike in 1911. His article Provisional Laws of Acquired Behavior or Learning makes frequent use of the term "modifying behavior". Through early research in the 1940s and the 1950s the term was used by Joseph Wolpe's research group. The experimental tradition in clinical psychology used it to refer to psycho-therapeutic techniques derived from empirical research. It has since come to refer mainly to techniques for increasing adaptive behavior through reinforcement and decreasing maladaptive behavior through extinction or punishment (with emphasis on the former). -

Behavior Therapy Was Given by Skinner and Lindsley
BEHAVIOUR THERAPY Degree Course (Three Years) Psychology Honours B. A. Part– I Honours Paper II : PSYCHOPATHOLOGY Unit 9 by Dr. Ranjan Kumar Ph. D ; M Phil ; PGDGC Assistant Professor of Psychology Ram Ratan Singh College, Mokama Patliputra University, Patna BEHAVIOUR THERAPY Dr. Ranjan Kumar Ph. D in Clinical Psychology (RINPAS, Ranchi) M. Phil. in Medical & Social Psychology (RINPAS, Ranchi) PG Diploma in Guidance & Counselling (RIE,NCERT,BBSR [email protected] The term Behavior Therapy was given by Skinner and Lindsley Popularized by Eyesenk Behavior therapy (BT) was developed in the 1950s more or less independently in three countries: (1) South Africa, where Joseph Wolpe developed a treatment, systematic desensitization, for phobias and other anxiety disorders and published the book Psychotherapy by reciprocal inhibition in 1958; (2) USA, where Ogden Lindsley used operant techniques in working with schizophrenic patients; and (3) England, where HansEysenck was instrumental in developing an alternative to psychoanalysis Why Behavior therapy? ◼ Late 1950 and early 1960 ◼ People became aware of the limitations of Freudian Psychotherapy ◼ Psychologist became aware of Social Learning approach in the treatment of abnormal behavior. ◼ Based on experimentally established principle of learning. ◼ Unadaptive behaviors are eliminated, adaptive behaviors are strengthened. (Wolpe,1969) Approaches of BT ◼ Pavlovian Approach * best illustrated by the work of Wolpe use for phobias, sexual problem, social inhibition ◼ Skinnerain Approach * Great use in hospital psychotics,MR child and autistic child. Assumption of BT ◼ It has connection with behaviors rather than underlying causes. ◼ Maladaptive beh are acquired as adaptive beh,so they are unlearned during BT. ◼ BT demands a specific treatment goal, which was not present in traditional therapy. -

1 Special Event
#308 International Poster Session 5/24/2009 5:30 p.m.- 7:00 p.m. North Hall A AUT 1. Some Effects of Pace of Instruction on Problem Behavior During Discrete Trial Instruction. (Applied Behavior Analysis) CRYSTAL N. BOWEN (Marcus Autism Center), Amber L. Valentino (The Marcus Autism Center), M. Alice Shillingsburg (Marcus Institute), Nathan A. Call (Marcus Autism Center and Emory University School of Medicine) Abstract: Discrete trial instruction (DTI) is a method commonly used in intervention for children with language deficits. The current research supports the effectiveness of DTI for this population; however, the research on the specific parameters utilized during DTI is limited. Current literature suggests that manipulation of the Inter-trial Interval (ITI), or pace of instruction, can influence the number of trials to criterion, final performance, and stability during teaching situations (Holt and Schafer, 1973). Although research does not suggest a specific ITI to create an ideal pace of instruction, research has suggested that pace of instruction is a variable that can be manipulated and can influence responding. As suggested by Koegel et al., utilizing this information can be important in selecting the optimal interval for teaching children with autism. In the current study, we used a multi-element design to assess the effects of pace of instruction on the rate of problem behavior during language intervention (DTI) in a classroom setting. Additionally, we assessed whether the pace of instruction or the rate of reinforcement during fast paced instruction that affects problem behavior during DTI. 2. Teaching Relaxation Strategies and Appropriate Break Requests to an Adolescent Girl with Autism.