Bromine As a Drinking-Water Disinfectant
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Disinfection Byproducts in Chlorinated Drinking Water
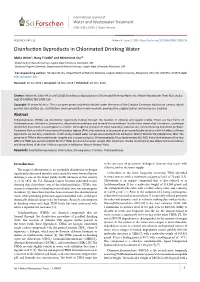
International Journal of Water and Wastewater Treatment SciO p Forschene n HUB for Sc i e n t i f i c R e s e a r c h ISSN 2381-5299 | Open Access RESEARCH ARTICLE Volume 4 - Issue 2 | DOI: http://dx.doi.org/10.16966/2381-5299.156 Disinfection Byproducts in Chlorinated Drinking Water Malia Vester1, Hany F Sobhi2 and Mintesinot Jiru1* 1Department of Natural Sciences, Coppin State University, Maryland, USA 2Center for Organic Synthesis, Department of Natural Sciences, Coppin State University, Maryland, USA *Corresponding author: Mintesinot Jiru, Department of Natural Sciences, Coppin State University, Maryland, USA, Tel: 410-951-4139; E-mail: [email protected] Received: 07 Jul, 2018 | Accepted: 14 Nov, 2018 | Published: 20 Nov, 2018 Citation: Vester M, Sobhi HF, Jiru M (2018) Disinfection Byproducts in Chlorinated Drinking Water. Int J Water Wastewater Treat 4(2): dx.doi. org/10.16966/2381-5299.156 Copyright: © Vester M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Trihalomethanes (THMs) are disinfection byproducts formed through the reaction of chlorine and organic matter. There are four forms of Trihalomethanes: chloroform, bromoform, dibromochloromethane and bromodichloromethane. Studies have shown that chloroform, a principal disinfection byproduct, is carcinogenic in rodents. Although the presence of these hazardous materials are constantly being monitored by Water Treatment Plant and the Environmental Protection Agency (EPA), they continue to be present at an unpredictable levels and the full effects of these byproducts are not fully understood. -

The Development of the Periodic Table and Its Consequences Citation: J
Firenze University Press www.fupress.com/substantia The Development of the Periodic Table and its Consequences Citation: J. Emsley (2019) The Devel- opment of the Periodic Table and its Consequences. Substantia 3(2) Suppl. 5: 15-27. doi: 10.13128/Substantia-297 John Emsley Copyright: © 2019 J. Emsley. This is Alameda Lodge, 23a Alameda Road, Ampthill, MK45 2LA, UK an open access, peer-reviewed article E-mail: [email protected] published by Firenze University Press (http://www.fupress.com/substantia) and distributed under the terms of the Abstract. Chemistry is fortunate among the sciences in having an icon that is instant- Creative Commons Attribution License, ly recognisable around the world: the periodic table. The United Nations has deemed which permits unrestricted use, distri- 2019 to be the International Year of the Periodic Table, in commemoration of the 150th bution, and reproduction in any medi- anniversary of the first paper in which it appeared. That had been written by a Russian um, provided the original author and chemist, Dmitri Mendeleev, and was published in May 1869. Since then, there have source are credited. been many versions of the table, but one format has come to be the most widely used Data Availability Statement: All rel- and is to be seen everywhere. The route to this preferred form of the table makes an evant data are within the paper and its interesting story. Supporting Information files. Keywords. Periodic table, Mendeleev, Newlands, Deming, Seaborg. Competing Interests: The Author(s) declare(s) no conflict of interest. INTRODUCTION There are hundreds of periodic tables but the one that is widely repro- duced has the approval of the International Union of Pure and Applied Chemistry (IUPAC) and is shown in Fig.1. -
درمان و تشخیص نامه شیوه کلرین گاز با مسمومیت Medical Guideline For
شیوه نامه تشخیص و درمان مسمومیت با گاز کلرین Medical Guideline for Chlorine Gas Poisoning اداره کل پدافند غیرعامل وزارت بهداشت، درمان و آموزش پزشکی مرداد 6931 فهرست مطالب عنوان صفحه 1- مشخصات کلی ....................................................................................................................................... 1 1 ....................................................................................................................... Threshold Limit Values; 2- ویژگیها ............................................................................................................................................... 2 2-1: مکانیسم اثر ...................................................................................................................................... 2 3- نحوه مواجهه و تماس ............................................................................................................................... 3 3-1- مواجهه حاد تنفسی ............................................................................................................................ 4 3-2- مواجهه حاد پوستی ـ مخاطی ................................................................................................................ 4 3-3- مواجهه حاد گوارشی .......................................................................................................................... 5 4- عﻻیم و نشانه های مسمومیت ...................................................................................................................... 5 4-1- عﻻیم مواجهه حاد تنفسی -

Toxicological Profile for Chlorine
CHLORINE 25 3. HEALTH EFFECTS 3.1 INTRODUCTION The primary purpose of this chapter is to provide public health officials, physicians, toxicologists, and other interested individuals and groups with an overall perspective on the toxicology of chlorine. It contains descriptions and evaluations of toxicological studies and epidemiological investigations and provides conclusions, where possible, on the relevance of toxicity and toxicokinetic data to public health. A glossary and list of acronyms, abbreviations, and symbols can be found at the end of this profile. 3.2 DISCUSSION OF HEALTH EFFECTS BY ROUTE OF EXPOSURE To help public health professionals and others address the needs of persons living or working near hazardous waste sites, the information in this section is organized first by route of exposure (inhalation, oral, and dermal) and then by health effect (death, systemic, immunological, neurological, reproductive, developmental, genotoxic, and carcinogenic effects). These data are discussed in terms of three exposure periods: acute (14 days or less), intermediate (15–364 days), and chronic (365 days or more). Levels of significant exposure for each route and duration are presented in tables and illustrated in figures. The points in the figures showing no-observed-adverse-effect levels (NOAELs) or lowest observed-adverse-effect levels (LOAELs) reflect the actual doses (levels of exposure) used in the studies. LOAELs have been classified into "less serious" or "serious" effects. "Serious" effects are those that evoke failure in a biological system and can lead to morbidity or mortality (e.g., acute respiratory distress or death). "Less serious" effects are those that are not expected to cause significant dysfunction or death, or those whose significance to the organism is not entirely clear. -

Toxicological Profile for Bromodichloromethane
BROMODICHLOROMETHANE 89 CHAPTER 5. POTENTIAL FOR HUMAN EXPOSURE 5.1 OVERVIEW Bromodichloromethane has been identified in at least 238 of the 1,854 hazardous waste sites that have been proposed for inclusion on the EPA National Priorities List (NPL) (ATSDR 2017). However, the number of sites in which bromodichloromethane has been evaluated is not known. The number of sites in each state is shown in Figure 5-1. Of these sites, 233 are located within the United States, 2 are located in the Virgin Islands, and 3 are located in Puerto Rico (not shown). Figure 5-1. Number of NPL Sites with Bromodichloromethane Contamination • The most likely route of exposure for the general public to bromodichloromethane is through ingestion, inhalation, and dermal contact of chlorinated drinking water. • A median bromodichloromethane intake of 2.8–4.2 µg/day from drinking water has been estimated; inhalation and dermal exposure would add to this daily intake. BROMODICHLOROMETHANE 90 5. POTENTIAL FOR HUMAN EXPOSURE • Bromodichloromethane is formed as a byproduct of water disinfection methods using chlorination. This is the primary source of bromodichloromethane in the environment. • Its principal use is as a chemical intermediate for organic synthesis and as a chemical reagent. • Volatilization is an important fate process. Bromodichloromethane evaporates from sources and enters the environment as a gas, which is slowly broken down in air. Residual bromodichloromethane may be broken down slowly by bacteria. • In the atmosphere, bromodichloromethane is thought to undergo slow degradation through oxidative pathways, with a half-life of about 2–3 months. 5.2 PRODUCTION, IMPORT/EXPORT, USE, AND DISPOSAL 5.2.1 Production The principal anthropogenic source of bromodichloromethane is its unintentional formation as a byproduct during the chlorination of water containing organic materials and bromide. -

Of the Periodic Table
of the Periodic Table teacher notes Give your students a visual introduction to the families of the periodic table! This product includes eight mini- posters, one for each of the element families on the main group of the periodic table: Alkali Metals, Alkaline Earth Metals, Boron/Aluminum Group (Icosagens), Carbon Group (Crystallogens), Nitrogen Group (Pnictogens), Oxygen Group (Chalcogens), Halogens, and Noble Gases. The mini-posters give overview information about the family as well as a visual of where on the periodic table the family is located and a diagram of an atom of that family highlighting the number of valence electrons. Also included is the student packet, which is broken into the eight families and asks for specific information that students will find on the mini-posters. The students are also directed to color each family with a specific color on the blank graphic organizer at the end of their packet and they go to the fantastic interactive table at www.periodictable.com to learn even more about the elements in each family. Furthermore, there is a section for students to conduct their own research on the element of hydrogen, which does not belong to a family. When I use this activity, I print two of each mini-poster in color (pages 8 through 15 of this file), laminate them, and lay them on a big table. I have students work in partners to read about each family, one at a time, and complete that section of the student packet (pages 16 through 21 of this file). When they finish, they bring the mini-poster back to the table for another group to use. -

Effects on Bromine, Chlorine and SO2 Under Air Firing and Oxy-Fuel
GAS-PHASE MERCURY OXIDATION: EFFECTS OF BROMINE, CHLORINE AND SO2 UNDER AIR FIRING AND OXY-FUEL CONDITIONS, EXPERIMENTAL AND MODELING STUDY by Paula Andrea Buitrago A dissertation submitted to the faculty of The University of Utah in partial fulfillment of the requirements for the degree of Doctor of Philosophy Department of Chemical Engineering The University of Utah August 2011 Copyright © Paula Andrea Buitrago 2011 All Rights Reserved STATEMENT OF DISSERTATION APPROVAL The dissertation of Paula Andrea Bnitrago has been approved by the following supervisory committee members: Geoffrey D. Silcox , Chair 4/1112011 Date Approved JoAnn S. Lighty , Member 4/1112011 Date Approved Jost Wendt , Member 4/18/2011 bate Approved Connie Senior , Member 4/15/2011 Date Approved Eric G. Eddings , Member 4/1112011 bate Approved and by JoAnn S. Lighty , Chair of ----------------~~~~==~~--------------- the Department of Chemical Engineering and by Charles A. Wight, Dean of The Graduate School. ABSTRACT The mercury in coal is emitted in its elemental state when the coal is burned. As the combustion flue gas cools, reactions under homogeneous and heterogeneous conditions between mercury and species such chlorine, bromine, SOx and NOx can take place. The temperature and concentration of these species determines the extent of mercury oxidation. The main objective of this study was to evaluate the effects of bromine, chlorine, SOx and NOx on gas-phase mercury oxidation reactions in flue gas. This study used a methane-fired, bench-scale reactor and CHEMKIN software for performing kinetic calculations. The model included reaction pathways to account for halogen, mercury, and combustion chemistry. The experimental results showed that chlorine is not effective as a gas-phase oxidant of mercury compared with other halogens such as bromine. -

DBDMH As a Processing Aid to the List of Allowed Substances in the National Organic Program
CBI Deleted ALBEMARLE CORPORATION Petition to add DBDMH as a processing aid to the List of Allowed Substances in the National Organic Program This petition contains Confidential Business Information. This includes “trade secrets” related to the production process and quality control tests and data. This information is commercially valuable, used in Albemarle business and maintained in secrecy. Introduction Hypobromous acid (HOBr) derived from 1,3-dibromo-5,5-dimethylhydantoin (DBDMH, CAS No. 77-48-5) exhibits antimicrobial effects in water. It is used as a post-harvest intervention in the beef industry, and results from laboratory studies and commercial trials have shown a reduction in E. coli and Salmonella levels1 with HOBr from DBDMH. It can be used to control bacterial numbers on beef hides, carcasses, heads and organs. This chemistry is also used in the poultry processing industry. DBDMH is a stable white to off-white granular solid. In water, DBDMH undergoes a hydrolysis reaction to form two molecules of hypobromous acid (HOBr) and one molecule of dimethylhydantoin (DMH). During use, DBDMH is placed into a flow-through chemical feeder. The aqueous output of this feeder is mixed with a separate stream of water to dilute the HOBr to the desired level, and supply a constant stream of HOBr to the DBDMH application system. The water flow to the feeder and the water flow for dilution can be controlled to achieve the proper dilution to obtain the desired HOBr concentration. Hypobromous acid is the active antimicrobial agent in the water applied to the beef. The oxidizing action of hypobromous acid kills the bacteria. -
Evaluating Analytical Methods for Detecting Unknown Chemicals in Recycled Water
PROJECT NO. 4992 Evaluating Analytical Methods for Detecting Unknown Chemicals in Recycled Water Evaluating Analytical Methods for Detecting Unknown Chemicals in Recycled Water Prepared by: Keith A. Maruya Charles S. Wong Southern California Coastal Water Research Project Authority 2020 The Water Research Foundation (WRF) is a nonprofit (501c3) organization which provides a unified source for One Water research and a strong presence in relationships with partner organizations, government and regulatory agencies, and Congress. The foundation conducts research in all areas of drinking water, wastewater, stormwater, and water reuse. The Water Research Foundation’s research portfolio is valued at over $700 million. The Foundation plays an important role in the translation and dissemination of applied research, technology demonstration, and education, through creation of research‐based educational tools and technology exchange opportunities. WRF serves as a leader and model for collaboration across the water industry and its materials are used to inform policymakers and the public on the science, economic value, and environmental benefits of using and recovering resources found in water, as well as the feasibility of implementing new technologies. For more information, contact: The Water Research Foundation Alexandria, VA Office Denver, CO Office 1199 North Fairfax Street, Suite 900 6666 West Quincy Avenue Alexandria, VA 22314‐1445 Denver, Colorado 80235‐3098 Tel: 571.384.2100 Tel: 303.347.6100 www.waterrf.org [email protected] ©Copyright 2020 by The Water Research Foundation. All rights reserved. Permission to copy must be obtained from The Water Research Foundation. WRF ISBN: 978‐1‐60573‐503‐0 WRF Project Number: 4992 This report was prepared by the organization(s) named below as an account of work sponsored by The Water Research Foundation. -

NACE Bromine Chemistry Review Paper
25 YEARS OF BROMINE CHEMISTRY IN INDUSTRIAL WATER SYSTEMS: A REVIEW Christopher J. Nalepa Albemarle Corporation P.O. Box 14799 Baton Rouge, LA 70898 ABSTRACT Bromine chemistry is used to great advantage in nature for fouling control by a number of sessile marine organisms such as sponges, seaweeds, and bryozoans. Such organisms produce small quantities of brominated organic compounds that effectively help keep their surfaces clean of problem bacteria, fungi, and algae. For over two decades, bromine chemistry has been used to similar advantage in the treatment of industrial water systems. The past several years in particular has seen the development of several diverse bromine product forms – one-drum stabilized bromine liquids, all-bromine hydantoin solids, and pumpable gels. The purpose of this paper is to review the development of bromine chemistry in industrial water treatment, discuss characteristics of the new product forms, and speculate on future developments. Keywords: Oxidizing biocide, bleach, bromine, bromine chemistry, sodium hypobromite, activated sodium bromide, Bromochlorodimethylhydantoin, Bromochloromethyethylhydantoin, Dibromodi- methylhydantoin,, BCDMH, BCMEH, DBDMH, stabilized bromine chloride, stabilized hypobromite INTRODUCTION Sessile marine organisms generate metabolites to ward off predators and deter attachment of potential micro- and macrofoulants. Sponges, algae, and bryozoans for example, produce a rich variety of bromine-containing compounds that exhibit antifoulant properties (Fig. 1).1,2,3 Scientists are actively studying these organisms to understand how they maintain surfaces that are relatively clean and slime- free.4 Brominated furanones isolated from the red algae Delisea pulchra, for example, have been found to interfere with the chemical signals (acylated homoserine lactones) that bacteria use to communicate with one another to produce biofilms.5,6 This work may eventually lead to more effective control of microorganisms in a number of industries such as industrial water treatment, oil and gas production, health care, etc. -

Stratospheric Ozone Is Destroyed by Reactions Involving
20 Questions: 2010 Update Section II: THE OZONE DEPLETION PROCESS What are the chlorine and bromine reactions that destroy Q9 stratospheric ozone? Reactive gases containing chlorine and bromine destroy stratospheric ozone in “catalytic” cycles made up of two or more separate reactions. As a result, a single chlorine or bromine atom can destroy many thousands of ozone molecules before it leaves the stratosphere. In this way, a small amount of reactive chlorine or bromine has a large impact on the ozone layer. A special situation develops in polar regions in the late winter/early spring season where large enhancements in the abun- dance of the most reactive gas, chlorine monoxide, leads to severe ozone depletion. tratospheric ozone is destroyed by reactions involving before it happens to react with another gas, breaking the cata- Sreactive halogen gases, which are produced in the chemi- lytic cycle, and up to tens of thousands of ozone molecules cal conversion of halogen source gases (see Figure Q8-1). The during the total time of its stay in the stratosphere. most reactive of these gases are chlorine monoxide (ClO), bro- Polar Cycles 2 and 3. The abundance of ClO is greatly mine monoxide (BrO), and chlorine and bromine atoms (Cl increased in polar regions during winter as a result of reac- and Br). These gases participate in three principal reaction tions on the surfaces of polar stratospheric clouds (PSCs) (see cycles that destroy ozone. Q8 and Q10). Cycles 2 and 3 (see Figure Q9-2) become the Cycle 1. Ozone destruction Cycle 1 is illustrated in Figure dominant reaction mechanisms for polar ozone loss because of Q9-1. -

Hypothiocyanous Acid Oxidation of Tubulin Cysteines Inhibits Microtubule Polymerization
W&M ScholarWorks Undergraduate Honors Theses Theses, Dissertations, & Master Projects 5-2011 Hypothiocyanous Acid Oxidation of Tubulin Cysteines Inhibits Microtubule Polymerization Hillary Meghan Clark College of William and Mary Follow this and additional works at: https://scholarworks.wm.edu/honorstheses Part of the Chemistry Commons Recommended Citation Clark, Hillary Meghan, "Hypothiocyanous Acid Oxidation of Tubulin Cysteines Inhibits Microtubule Polymerization" (2011). Undergraduate Honors Theses. Paper 398. https://scholarworks.wm.edu/honorstheses/398 This Honors Thesis -- Open Access is brought to you for free and open access by the Theses, Dissertations, & Master Projects at W&M ScholarWorks. It has been accepted for inclusion in Undergraduate Honors Theses by an authorized administrator of W&M ScholarWorks. For more information, please contact [email protected]. Hypothiocyanous acid oxidation of tubulin cysteines inhibits microtubule polymerization A thesis submitted in partial fulfillment of the requirement for the degree of Bachelor of Science in Chemistry from The College of William and Mary by Hillary Meghan Clark Accepted for _________________________ (Honors) ___________________________________ Dr. Lisa M. Landino, Director ___________________________________ Dr. Lizabeth A. Allison ___________________________________ Dr. Gary W. Rice Williamsburg, VA April 27, 2011 i Table of Contents List of Figures iii List of Tables iv List of Abbreviations v Chemical Index vi Introduction 1 Reactive Oxygen Species 1 Antioxidants