Dynamic Ultrasonography of the Shoulder
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Body Mechanics As the Rotator Cuff Gether in a Cuff-Shape Across the Greater and Lesser Tubercles the on Head of the Humerus
EXPerT CONTENT Body Mechanics by Joseph E. Muscolino | Artwork Giovanni Rimasti | Photography Yanik Chauvin Rotator Cuff Injury www.amtamassage.org/mtj WORKING WITH CLieNTS AFFecTED BY THIS COmmON CONDITION ROTATOR CUFF GROUP as the rotator cuff group because their distal tendons blend and attach to- The four rotator cuff muscles are gether in a cuff-shape across the greater and lesser tubercles on the head of the supraspinatus, infraspinatus, the humerus. Although all four rotator cuff muscles have specific concen- teres minor, and subscapularis (Fig- tric mover actions at the glenohumeral (GH) joint, their primary functional ure 1). These muscles are described importance is to contract isometrically for GH joint stabilization. Because 17 Before practicing any new modality or technique, check with your state’s or province’s massage therapy regulatory authority to ensure that it is within the defined scope of practice for massage therapy. the rotator cuff group has both mover and stabilization roles, it is extremely functionally active and therefore often physically stressed and injured. In fact, after neck and low back conditions, the shoulder is the most com- Supraspinatus monly injured joint of the human body. ROTATOR CUFF PATHOLOGY The three most common types of rotator cuff pathology are tendinitis, tendinosus, and tearing. Excessive physi- cal stress placed on the rotator cuff tendon can cause ir- ritation and inflammation of the tendon, in other words, tendinitis. If the physical stress is chronic, the inflam- matory process often subsides and degeneration of the fascial tendinous tissue occurs; this is referred to as tendinosus. The degeneration of tendinosus results in weakness of the tendon’s structure, and with continued Teres minor physical stress, whether it is overuse microtrauma or a macrotrauma, a rotator cuff tendon tear might occur. -

Should Joint Presentation File
6/5/2017 The Shoulder Joint Bones of the shoulder joint • Scapula – Glenoid Fossa Infraspinatus fossa – Supraspinatus fossa Subscapular fossa – Spine Coracoid process – Acromion process • Clavicle • Humerus – Greater tubercle Lesser tubercle – Intertubercular goove Deltoid tuberosity – Head of Humerus Shoulder Joint • Bones: – humerus – scapula Shoulder Girdle – clavicle • Articulation – glenohumeral joint • Glenoid fossa of the scapula (less curved) • head of the humerus • enarthrodial (ball and socket) 1 6/5/2017 Shoulder Joint • Connective tissue – glenoid labrum: cartilaginous ring, surrounds glenoid fossa • increases contact area between head of humerus and glenoid fossa. • increases joint stability – Glenohumeral ligaments: reinforce the glenohumeral joint capsule • superior, middle, inferior (anterior side of joint) – coracohumeral ligament (superior) • Muscles play a crucial role in maintaining glenohumeral joint stability. Movements of the Shoulder Joint • Arm abduction, adduction about the shoulder • Arm flexion, extension • Arm hyperflexion, hyperextension • Arm horizontal adduction (flexion) • Arm horizontal abduction (extension) • Arm external and internal rotation – medial and lateral rotation • Arm circumduction – flexion, abduction, extension, hyperextension, adduction Scapulohumeral rhythm • Shoulder Joint • Shoulder Girdle – abduction – upward rotation – adduction – downward rotation – flexion – elevation/upward rot. – extension – Depression/downward rot. – internal rotation – Abduction (protraction) – external rotation -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Shoulder Impingement
3 Shoulder Impingement Catherine E. Tagg, FRCR1 Alastair S. Campbell, FRCR2 Eugene G. McNally, FRCR3 1 Nevill Hall Hospital, Aneurin Bevan Health Board, Abergavenny, Address for correspondence Eugene G. McNally, FRCR, Nuffield United Kingdom Orthopaedic Centre, Oxford University Hospitals NHS Trust, Old Road, 2 Craigavon Area Hospital, Southern Health and Social Care Trust, Oxford, OX3 7LD, UK (e-mail: [email protected]). Portadown, United Kingdom 3 Nuffield Orthopaedic Centre, Oxford University Hospitals NHS Trust, Oxford, United Kingdom Semin Musculoskelet Radiol 2013;17:3–11. Abstract This update examines recent articles and evidence for the role of ultrasound in the diagnosis and management of shoulder impingement syndromes and emphasizes its principal application in evaluation for external impingement. Shoulder ultrasound is Keywords commonly used as the initial investigation for patients with shoulder pain and suspected ► shoulder impingement. This is due to the high resolution of current ultrasound machines, wide ► ultrasound availability, good patient tolerance, cost effectiveness, and, most importantly, its ► impingement dynamic and interventional role. Impingement is a clinical scenario of painful functional limita- (AC) joint. The morphology of the acromion has been catego- tion of the shoulder,1 thought to be secondary to compression rized into three types (type I flat, type II concave, and type III or altered dynamics that irritate and ultimately damage the hooked). It has been suggested that the hooked type III tissues around the shoulder joint. Shoulder impingement is configuration may predispose to external impingement.9 currently subdivided into external (subacromial) and internal However, it is more likely that (unless the anatomical changes impingement. External impingement is further subdivided into are gross) acromial changes are secondary rather than pri- primary and secondary, and internal impingement into poster- mary. -

Chapter 5 the Shoulder Joint
The Shoulder Joint • Shoulder joint is attached to axial skeleton via the clavicle at SC joint • Scapula movement usually occurs with movement of humerus Chapter 5 – Humeral flexion & abduction require scapula The Shoulder Joint elevation, rotation upward, & abduction – Humeral adduction & extension results in scapula depression, rotation downward, & adduction Manual of Structural Kinesiology – Scapula abduction occurs with humeral internal R.T. Floyd, EdD, ATC, CSCS rotation & horizontal adduction – Scapula adduction occurs with humeral external rotation & horizontal abduction © McGraw-Hill Higher Education. All rights reserved. 5-1 © McGraw-Hill Higher Education. All rights reserved. 5-2 The Shoulder Joint Bones • Wide range of motion of the shoulder joint in • Scapula, clavicle, & humerus serve as many different planes requires a significant attachments for shoulder joint muscles amount of laxity – Scapular landmarks • Common to have instability problems • supraspinatus fossa – Rotator cuff impingement • infraspinatus fossa – Subluxations & dislocations • subscapular fossa • spine of the scapula • The price of mobility is reduced stability • glenoid cavity • The more mobile a joint is, the less stable it • coracoid process is & the more stable it is, the less mobile • acromion process • inferior angle © McGraw-Hill Higher Education. All rights reserved. 5-3 © McGraw-Hill Higher Education. All rights reserved. From Seeley RR, Stephens TD, Tate P: Anatomy and physiology , ed 7, 5-4 New York, 2006, McGraw-Hill Bones Bones • Scapula, clavicle, & humerus serve as • Key bony landmarks attachments for shoulder joint muscles – Acromion process – Humeral landmarks – Glenoid fossa • Head – Lateral border • Greater tubercle – Inferior angle • Lesser tubercle – Medial border • Intertubercular groove • Deltoid tuberosity – Superior angle – Spine of the scapula © McGraw-Hill Higher Education. -

Axial Skeleton List for API
Axial Skeleton List for API Sutures Coronal Lambdoidal Squamous Sagittal Bones of the Skull Frontal Bone Parietal Bone Temporal Bone Occipital Bone Zygomatic Bone Zygomatic Arch Zygomatic Process Mandible (mental foramen) Maxilla Nasal Bone Vomer Bone Ethmoid Bone (Crista galli) Foramen magnum Sella turcica External auditory (acoustic) meatus Mastoid Process Styloid Process Superior nuchal line Inferior nuchal line External occipital protuberance (EOP) Sternum (xyphoid process) Ribs Sacrum Coccyx Dr. Tarsha Smith Page 1 Axial Skeleton List for API (continued) Vertebrae Atlas (superior articular facet; posterior tubercle) Axis (dens or odontoid process) Cervical, Thoracic, Lumbar Know following terms on all vertebrae, if present: Facet, Pedicle, Spinous, Body, Transverse process, Lamina Appendicular Skeleton List for API Clavicle Conoid tubercle Scapula Acromion Medial border Coracoid process Lateral border Glenoid cavity Subscapular fossa Spine Infraspinous fossa Humerus Head Capitulum Surgical neck Trochlea Greater tubercle Olecranon fossa Lesser tubercle Coronoid fossa Epicondyles (lateral & medial) Radius Tuberosity of radius Articular facets Styloid process Head & neck Ulna Trochlear notch Radial notch of ulna Coronoid process Hand Phalanges Metacarpals Carpals: Scaphoid, Lunate, Triquetrium, Pisiform, Trapezium, Trapezoid, Capitate, Hamate Dr. Tarsha Smith Page 2 Appendicular Skeleton List for API (continued) Pelvis Ilium Crest Anterior superior Anterior inferior Ischium Body Ramus Spine Pubis Pubic symphysis Obturator foramen Acetabulum Femur Fovea capitis Greater trochanter Head Neck Lesser trochanter Linea aspera Epicondyles (medial & lateral) Condyles (medial & lateral) Intercondylar fossa Patella (kneecap) Tibia Condyle (medial & lateral) Tibial tuberosity Medial malleolus Fibula Lateral malleolus Apex Foot Metatarsals Phalanx Tarsals: Cuneiforms, Navicular, talus, cuboid, calcaneus Dr. Tarsha Smith Page 3 . -

Muscles of the Upper Limb.Pdf
11/8/2012 Muscles Stabilizing Pectoral Girdle Muscles of the Upper Limb Pectoralis minor ORIGIN: INNERVATION: anterior surface of pectoral nerves ribs 3 – 5 ACTION: INSERTION: protracts / depresses scapula coracoid process (scapula) (Anterior view) Muscles Stabilizing Pectoral Girdle Muscles Stabilizing Pectoral Girdle Serratus anterior Subclavius ORIGIN: INNERVATION: ORIGIN: INNERVATION: ribs 1 - 8 long thoracic nerve rib 1 ---------------- INSERTION: ACTION: INSERTION: ACTION: medial border of scapula rotates scapula laterally inferior surface of scapula stabilizes / depresses pectoral girdle (Lateral view) (anterior view) Muscles Stabilizing Pectoral Girdle Muscles Stabilizing Pectoral Girdle Trapezius Levator scapulae ORIGIN: INNERVATION: ORIGIN: INNERVATION: occipital bone / spinous accessory nerve transverse processes of C1 – C4 dorsal scapular nerve processes of C7 – T12 ACTION: INSERTION: ACTION: INSERTION: stabilizes / elevates / retracts / upper medial border of scapula elevates / adducts scapula acromion / spine of scapula; rotates scapula lateral third of clavicle (Posterior view) (Posterior view) 1 11/8/2012 Muscles Stabilizing Pectoral Girdle Muscles Moving Arm Rhomboids Pectoralis major (major / minor) ORIGIN: INNERVATION: ORIGIN: INNERVATION: spinous processes of C7 – T5 dorsal scapular nerve sternum / clavicle / ribs 1 – 6 dorsal scapular nerve INSERTION: ACTION: INSERTION: ACTION: medial border of scapula adducts / rotates scapula intertubucular sulcus / greater tubercle flexes / medially rotates / (humerus) adducts -

Bone Handout”)
The Skeletal System (“Bone Handout”) Bone Markings - as in Table 6.1, know categories, names, descriptions and categories of bone markings Common Fractures - as in Table 6.2, identify type from pictures The Axial Skeleton Skull Cranial bones frontal (supraorbital foramen) parietal temporal (mastoid process, external auditory(acoustic) meatus, styloid process, zygomatic process, stylomastoid foramen) occipital (foramen magnum, hypoglossal canal, occipital condyles) sphenoid (optic canal, superior orbital fissure, sella turcica, foramen rotundum, foramen ovale, foramen spinosum , greater wings, lesser wings) ethmoid (olfactory foramina) Relevant Figures: 7.4, 7.6, 7.7a, 7.9 Facial bones nasal maxilla (infraorbital foramen, inferior orbital fissure) zygomatic mandible (mental foramen, body, ramus, mandibular condyle) lacrimal (lacrimal fossa) palatine inferior nasal conchae vomer Relevant Figures: 7.4, 7.6, 7.7a Sutures coronal sagittal lambdoid squamous Relevant Figures: 7.4, 7.5 Paranasal Sinuses frontal sphenoidal maxillary ethmoidal Relevant Figures: 7.15 Fontanels anterior posterior sphenoidal mastoid Relevant Figures: 7.28 Hyoid bone Relevant Figures: 7.17 1 Vertebrae Parts of a “typical vertebra” using thoracic as example body vertebral arch (pedicle, lamina, vertebral foramen) intervertebral foramen transverse process spinous process superior articular process inferior articular process Divisions of vertebral column cervical (transverse foramina) thoracic (transverse costal facet - for tubercle of rib, superior and inferior costal -
Radiographic Interpretation of the Canine Shoulder
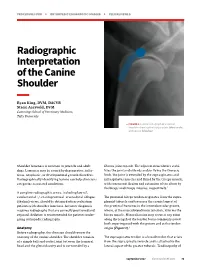
PROCEDURES PRO h ORTHOPEDICS/DIAGNOSTIC IMAGING h PEER REVIEWED Radiographic Interpretation of the Canine Shoulder Ryan King, DVM, DACVR Stacie Aarsvold, DVM Cummings School of Veterinary Medicine, Tufts University d FIGURE 1 Lateral radiograph of a normal shoulder showing the biceps origin (blue circle) and course (blue bar) Shoulder lameness is common in juvenile and adult fibrous joint capsule. The adjacent musculature stabi- dogs. Lameness may be caused by degenerative, infec- lizes the joint and extends and/or flexes the thoracic tious, neoplastic, or developmental growth disorders. limb. The joint is extended by the supraspinatus and Radiographically identifying lesions can help clinicians infraspinatus muscles and flexed by the triceps muscle, categorize associated conditions. with concurrent flexion and extension of the elbow by the biceps and triceps muscles, respectively.1 A complete radiographic series, including lateral, caudocranial +/- cranioproximal–craniodistal oblique The proximal biceps tendon originates from the supra- (skyline) views, should be obtained when evaluating glenoid tubercle and traverses the cranial aspect of patients with shoulder lameness. Accurate diagnosis the proximal humerus in the intertubercular groove, requires radiographs that are correctly positioned and where, at the musculotendinous junction, it forms the exposed. Sedation is recommended for patients under- biceps muscle. Mineralization may occur at any point going orthopedic radiography. along the length of the tendon but is commonly noted both superimposed with the groove and at the tendon Anatomy origin (Figure 1).1 Before radiography, the clinician should review the anatomy of the canine shoulder. The shoulder consists The supraspinatus tendon is a broad tendon that arises of a simple ball-and-socket joint between the humeral from the supraspinatus muscle and is attached to the head and the glenoid cavity and is surrounded by a lateral aspect of the greater tubercle. -

Localized Pigmented Villonodular Synovitis of the Shoulder, Acta Med Port 2013 Jul-Aug;26(4):459-462
Madruga Dias J, et al. Localized pigmented villonodular synovitis of the shoulder, Acta Med Port 2013 Jul-Aug;26(4):459-462 Joint Bone Spine. 2013;80:146–54. Emerg Med. 2012 (in press). 12. Citak M, Backhaus M, Tilkorn DJ, Meindl R, Muhr G, Fehmer T. Necrotiz- 14. Young MH, Aronoff DM, Engleberg NC. Necrotizing fasciitis: pathogen- ing fasciitis in patients with spinal cord injury: An analysis of 25 patients. esis and treatment. Expert Rev Anti Infect Ther. 2005;3:279–94. Spine. 2011;36:E1225-9. 15. Lancerotto L, Tocco I, Salmaso R, Vindigni V, Bassetto F. Necrotizing 13. Wilson MP, Schneir AB. A Case of Necrotizing Fasciitis with a LRINEC fasciitis: classification, diagnosis, and management. J Trauma Acute Score of Zero: Clinical Suspicion Should Trump Scoring Systems. J Care Surg. 2012;72:560–6. CASO CLÍNICO Localized Pigmented Villonodular Synovitis of the Shoulder: a Rare Presentation of an Uncommon Pathology Sinovite Vilonodular Pigmentada Circunscrita do Ombro: uma Apresentação Rara de uma Patologia Incomum João MADRUGA DIAS1, Maria Manuela COSTA1, Artur DUARTE2, José A. PEREIRA da SILVA1 Acta Med Port 2013 Jul-Aug;26(4):459-462 ABSTRACT Pigmented Vilonodular Synovitis is a rare clinical entity characterized as a synovial membrane benign tumour, despite possible aggres- sive presentation with articular destruction. The localized variant is four times less frequent and the shoulder involvement is uncommon. We present the case of a Caucasian 59 year-old patient, who presented with left shoulder pain, of uncharacteristic quality, with local swelling and marked functional limitation of 1 month duration. Shoulder ultrasonography showed subacromial bursitis. -

Soft Tissue Mass Around the Shoulder
6 Ann Rheum Dis 1998;57:6–8 CASE STUDIES IN DIAGNOSTIC IMAGING Series editor: V N Cassar-Pullicino Ann Rheum Dis: first published as 10.1136/ard.57.1.6 on 1 January 1998. Downloaded from Soft tissue mass around the shoulder H S Reid, E McNally, A Carr Clinical history tumours but characteristically arise adjacent A previously fit 47 year old female school to joints and grow slowly. With the exception teacher presented with a six month history of a of PVNS, all these conditions typically show painful swelling over her right shoulder. There some degree of calcification on plain film.1 was rapid development of the swelling initially, Most cases of synovial osteochondromatosis which then stabilised. On examination she was show a pattern of coarse calcification and one apyrexial with a large, firm, non-tender mass third of cases of synovial sarcomas show spotty around the right shoulder, which clinically had calcification.1 Cystic lesions such as a ganglion some cystic features. There was no significant or synovial cyst can occasionally reach this limitation of movement. Other findings on size. clinical examination included some minor soft A lipoma would fit the clinical context but fat tissue capsular swelling of the second and third is of lower density on plain film than muscle metacarpophalangeal joints of the right hand. and consequently would appear blacker on Otherwise the remainder of the locomotor sys- plain film. Other benign neoplasms such as a tem was normal. haemangioma or an angiolipoma could give Her erythrocyte sedimentation rate was this appearance and sarcoma has to be consid- increased at 51 mm 1st h, but C reactive ered.