Medial Epicondylitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Musculoskeletal Ultrasound Technical Guidelines II. Elbow
European Society of MusculoSkeletal Radiology Musculoskeletal Ultrasound Technical Guidelines II. Elbow Ian Beggs, UK Stefano Bianchi, Switzerland Angel Bueno, Spain Michel Cohen, France Michel Court-Payen, Denmark Andrew Grainger, UK Franz Kainberger, Austria Andrea Klauser, Austria Carlo Martinoli, Italy Eugene McNally, UK Philip J. O’Connor, UK Philippe Peetrons, Belgium Monique Reijnierse, The Netherlands Philipp Remplik, Germany Enzo Silvestri, Italy Elbow Note The systematic scanning technique described below is only theoretical, considering the fact that the examination of the elbow is, for the most, focused to one quadrant only of the joint based on clinical findings. 1 ANTERIOR ELBOW For examination of the anterior elbow, the patient is seated facing the examiner with the elbow in an extension position over the table. The patient is asked to extend the elbow and supinate the fore- arm. A slight bending of the patient’s body toward the examined side makes full supination and as- sessment of the anterior compartment easier. Full elbow extension can be obtained by placing a pillow under the joint. Transverse US images are first obtained by sweeping the probe from approximately 5cm above to 5cm below the trochlea-ulna joint, a Pr perpendicular to the humeral shaft. Cranial US images of the supracondylar region reveal the superficial biceps and the deep brachialis mu- Br scles. Alongside and medial to these muscles, follow the brachial artery and the median nerve: * the nerve lies medially to the artery. * Legend: a, brachial artery; arrow, median nerve; arrowheads, distal biceps tendon; asterisks, articular cartilage of the Humerus humeral trochlea; Br, brachialis muscle; Pr, pronator muscle 2 distal biceps tendon: technique The distal biceps tendon is examined while keeping the patient’s forearm in maximal supination to bring the tendon insertion on the radial tuberosity into view. -

Structure of the Flexor Digitorum Superficialis
Okajimas Folia Anat. Jpn., 56(5) : 277-288, December 1979 Structure of the Flexor Digitorum Superficialis By OSAMU OHTANI Department of Anatomy, Okayama University Medical School, Okayama 700, Japan (Director : Prof. Dr. H. Outi) —Received for Publication, March 9, 1979— Key Words: Flexor digitorum superficialis, Striated muscle, Forearm musculature. Summary. Fifty-two forearms of 26 Japanese adult cadavers were examined. The flexor digitorum superficialis can be separated into two layers: a superficial layer and a deep layer. The superficial layer is composed of the radial head and the superficial part of the humeroulnar head. It forms two muscle bellies which give rise to the tendons for the third and fourth digits, respectively. The deep layer is composed of the deep part of the humeroulnar head. After forming an inter- mediate tendon, the deep layer also divides into two fleshy bellies which give rise to the tendons for the second and fifth digits, respectively. Based on the mode of occurrence of the communicating muscle fasciculi between the superficial layer and the deep layer, the flexor digitorum superficialis can be classified into four types. Type I muscle has no communicating fasciculus (4/52, 7.7%). Type II muscle has a communicating muscle fasciculus between the intermediate tendon and the muscle belly for the fourth digit (muscle fasciculus A) (29/52, 55.8%). Type III muscle has the muscle fasciculus A as well as another communicating muscle fasciculus between the intermediate tendon and the belly for the third digit (muscle fasciculus B) (18/52, 34.6%). Type IV muscle has the muscle fasciculus B only (1/52, 1.9%). -

Disclosures Flexor Pronator Strain
11/19/2018 Flexor Pronator Strain, Epicondylitis, Avulsions Lee Kaplan, MD Director, UHealth Sports Medicine Institute Professor, Department of Orthopaedics, Kinesiology & Sports Science, Biomedical Engineering Medical Director and Head Team Physician, University of Miami Athletics Medical Director and Head Team Physician, Miami Marlins Josue Acevedo, MD Orthopaedics Sports Medicine fellow Disclosures • I have no conflicts of interest in relation to this presentation 2 Flexor Pronator Strain • Anatomy • Function • Forces • Clinical Presentation • Imaging Studies • Treatment 3 1 11/19/2018 Anatomy • Common Flexor Tendon origin - Medial Epicondyle Pronator Teres FCR Palmaris Longus FDS FCU 4 Function • Provides dynamic support to valgus stress during throwing motion • Contraction during early arm acceleration resists valgus and flexes wrist during ball release 5 Elbow Forces • Elbow valgus torque peaks at late cocking phase - during maximal shoulder external rotation (MER) • Can approach torque up to 120 N.m • Significantly higher torque in pitchers who enduring an injury Sawbick et al. JSES, 2004 Adam WA. AJSM, 2010. 6 2 11/19/2018 • Fastballs caused the greatest torque • Curveballs produced the greatest arm speed . • Predictors of increased elbow torque • Increased ball velocity • Higher BMI • Decreased arm slot • Protectors against elbow torque. • Increasing age • longer arm length • greater elbow circumference were independent 7 • VAS fatigue scores increased 0.72 points per inning • Medial elbow torque increased beyond inning 3, increase of 0.84 N·m each inning. • Pitch velocity decreased (0.28 mph per inning) • There were no differences in arm rotation or arm speed as the game progressed. • Arm slot decreased with each successive inning (0.73° on average per inning) ***These findings signify a possible relationship between fatigue and injury risk. -

Anatomical Considerations of Fascial Release in Ulnar Nerve Transposition: a Concept Revisited
LABORATORY INVESTIGATION J Neurosurg 123:1216–1222, 2015 Anatomical considerations of fascial release in ulnar nerve transposition: a concept revisited Mark A. Mahan, MD,1 Jaime Gasco, MD,2 David B. Mokhtee, MD,3 and Justin M. Brown, MD4 1Division of Neurological Surgery, Barrow Neurological Institute, St. Joseph’s Hospital and Medical Center, Phoenix, Arizona; 2Division of Neurological Surgery, University of Texas Medical Branch, Galveston, Texas; 3Tulsa Bone and Joint Associates, Tulsa, Oklahoma; and 4Division of Neurosurgery, University of California, San Diego, La Jolla, California OBJECT Surgical transposition of the ulnar nerve to alleviate entrapment may cause otherwise normal structures to become new sources of nerve compression. Recurrent or persistent neuropathy after anterior transposition is commonly attributable to a new distal compression. The authors sought to clarify the anatomical relationship of the ulnar nerve to the common aponeurosis of the humeral head of the flexor carpi ulnaris (FCU) and flexor digitorum superficialis (FDS) muscles following anterior transposition of the nerve. METHODS The intermuscular septa of the proximal forearm were explored in 26 fresh cadaveric specimens. The fibrous septa and common aponeurotic insertions of the flexor-pronator muscle mass were evaluated in relation to the ulnar nerve, with particular attention to the effect of transposition upon the nerve in this region. RESULTS An intermuscular aponeurosis associated with the FCU and FDS muscles was present in all specimens. Transposition consistently resulted in angulation of the nerve during elbow flexion when this fascial septum was not released. The proximal site at which the nerve began to traverse this fascial structure was found to be an average of 3.9 cm (SD 0.7 cm) from the medial epicondyle. -

Tracy L. Kivell Pierre Lemelin Brian G. Richmond Daniel Schmitt
Developments in Primatology: Progress and Prospects Series Editor: Louise Barrett Tracy L. Kivell Pierre Lemelin Brian G. Richmond Daniel Schmitt Editors The Evolution of the Primate Hand Anatomical, Developmental, Functional, and Paleontological Evidence Developments in Primatology: Progress and Prospects Series Editor Louise Barrett Lethbridge , Alberta , Canada More information about this series at http://www.springer.com/series/5852 Tracy L. Kivell • Pierre Lemelin Brian G. Richmond • Daniel Schmitt Editors The Evolution of the Primate Hand Anatomical, Developmental, Functional, and Paleontological Evidence Editors Tracy L. Kivell Pierre Lemelin Animal Postcranial Evolution (APE) Lab Division of Anatomy Skeletal Biology Research Centre Department of Surgery School of Anthropology and Conservation Faculty of Medicine and Dentistry, University of Kent University of Alberta Canterbury, UK Edmonton , AB , Canada Department of Human Evolution Daniel Schmitt Max Planck Institute for Evolutionary Department of Evolutionary Anthropology Anthropology Duke University Leipzig , Germany Durham , NC , USA Brian G. Richmond Division of Anthropology American Museum of Natural History New York , NY , USA Department of Human Evolution Max Planck Institute for Evolutionary Anthropology Leipzig, Germany ISSN 1574-3489 ISSN 1574-3497 (electronic) Developments in Primatology: Progress and Prospects ISBN 978-1-4939-3644-1 ISBN 978-1-4939-3646-5 (eBook) DOI 10.1007/978-1-4939-3646-5 Library of Congress Control Number: 2016935857 © Springer Science+Business Media New York 2016 This work is subject to copyright. All rights are reserved by the Publisher, whether the whole or part of the material is concerned, specifi cally the rights of translation, reprinting, reuse of illustrations, recitation, broadcasting, reproduction on microfi lms or in any other physical way, and transmission or information storage and retrieval, electronic adaptation, computer software, or by similar or dissimilar methodology now known or hereafter developed. -
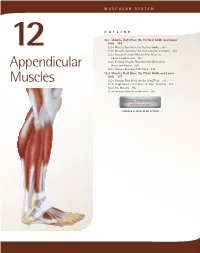
Appendicular Muscles 355
MUSCULAR SYSTEM OUTLINE 12.1 Muscles That Move the Pectoral Girdle and Upper Limb 355 12.1a Muscles That Move the Pectoral Girdle 355 12 12.1b Muscles That Move the Glenohumeral Joint/Arm 360 12.1c Arm and Forearm Muscles That Move the Elbow Joint/Forearm 363 12.1d Forearm Muscles That Move the Wrist Joint, Appendicular Hand, and Fingers 366 12.1e Intrinsic Muscles of the Hand 374 12.2 Muscles That Move the Pelvic Girdle and Lower Limb 377 Muscles 12.2a Muscles That Move the Hip Joint/Thigh 377 12.2b Thigh Muscles That Move the Knee Joint/Leg 381 12.2c Leg Muscles 385 12.2d Intrinsic Muscles of the Foot 391 MODULE 6: MUSCULAR SYSTEM mck78097_ch12_354-396.indd 354 2/14/11 3:25 PM Chapter Twelve Appendicular Muscles 355 he appendicular muscles control the movements of the upper 2. Identify the muscles that move the scapula and their actions. T and lower limbs, and stabilize and control the movements 3. Name the muscles of the glenohumeral joint, and explain of the pectoral and pelvic girdles. These muscles are organized how each moves the humerus. into groups based on their location in the body or the part of 4. Locate and name the muscles that move the elbow joint. the skeleton they move. Beyond their individual activities, these 5. Identify the muscles of the forearm, wrist joint, fingers, muscles also work in groups that are either synergistic or antago- and thumb. nistic. Refer to figure 10.14 to review how muscles are named, and Muscles that move the pectoral girdle and upper limbs are recall the first Study Tip! from chapter 11 that gives suggestions organized into specific groups: (1) muscles that move the pectoral for learning the muscles. -
Aandp1ch10lecture.Pdf
Chapter 10 Lecture Outline See separate PowerPoint slides for all figures and tables pre- inserted into PowerPoint without notes. Copyright © McGraw-Hill Education. Permission required for reproduction or display. 1 Introduction Copyright © The McGraw-Hill Education. Permission required for reproduction or display. • Muscles constitute nearly half of the body’s weight and are of central interest in several fields of health care and fitness Figure 10.5a 10-2 The Structural and Functional Organization of Muscles • Expected Learning Outcomes – Describe the varied functions of muscles. – Describe the connective tissue components of a muscle and their relationship to the bundling of muscle fibers. – Describe the various shapes of skeletal muscles and relate this to their functions. – Explain what is meant by the origin, insertion, belly, action, and innervation of a muscle. 10-3 The Structural and Functional Organization of Muscles (Continued) – Describe the ways that muscles work in groups to aid, oppose, or moderate each other’s actions. – Distinguish between intrinsic and extrinsic muscles. – Describe, in general terms, the nerve supply to the muscles and where these nerves originate. – Explain how the Latin names of muscles can aid in visualizing and remembering them. 10-4 The Structural and Functional Organization of Muscles • About 600 human skeletal muscles • Constitute about half of our body weight • Three kinds of muscle tissue – Skeletal, cardiac, smooth • Specialized for one major purpose – Converting the chemical energy in ATP -

WNL, Elbow Regional Examination Observation
Elbow Regional Examination Patient:____________________________________ date: ______ Check normal, circle & describe abnormal (dd/mm/yr) CC & signifi cant history: ____________________________________________________ Insurance: ______________________________________ __________________________________________________________________________ Date of birth: ____________________________________ M/F Fracture screen (tuning fork, percussion, torsion test, grip strength): □ WWNLNL, □ RReferefer fforor XX-ra-ray: _________________________________________ Observation: □ WWNLNL Palpation: □ WWNL,NL, texture, tenderness, pain referral Development: □ ggood,ood, □ ffair,air, □ ppooroor RRightight LLefteft □ AAntalgia:ntalgia: __________________________________________________ Palpation L R Palpation L R □ SSkinkin ((bruising,bruising, sscars):cars): ______________________________ Medial epicondyle Common exten. tendon □ AAsymmetry:symmetry: ______________________________________________ Ulnar groove Anconeus Observation □ WNL L R Med. collateral ligament Brachioradialis Common fl exor tendon Extensor carpi ulnaris Head tilt Flexor carpi ulnaris Extensor carpi rad longus Head rotation Palmaris longus Extensor carpi rad brevis Shoulder high Flexor carpi radialis Extensor digitorum Shoulder rounded Pronator teres Supinator Humerus rotated Biceps tendon Triceps tendon Elbow fl exed Head of radius Triceps muscle Elbow hyperextended Radial tunnel Olecranon Valgus forearm Lateral epicondyle Olecranon bursa Varus forearm Lat. collateral ligament Cubital fossa -

A Case Report of Unilateral Absence of Palmaris Longus
International Journal of Health Sciences and Research www.ijhsr.org ISSN: 2249-9571 Case Report A Case Report of Unilateral Absence of Palmaris Longus Dr Anju Thomas1, Dr Vinod Kumar Alapatti2 1Associate Professor, Department of Rachana Sharira, Sri Dharmasthala Manjunatheshwara College of Ayurveda & Hospital, Hassan-573 201, Karnataka, India 2Professor, Rajiv Gandhi Ayurveda Medical College & Hospital, Mahe Corresponding Author: Dr Anju Thomas ABSTRACT Palmaris longus is one among the superficial flexor muscles of forearm possessing a short fusiform belly and a long tendon lying between the flexor carpi radialis and the flexor carpi ulnaris. It is phylogenetically a degenerating muscle which shows a lot of variations, the most common one being absence. Based on ethnicity, gender, race, and hand dominance, it may be absent in individuals either unilaterally or bilaterally. [1] This paper describes the unilateral absence of palmaris longus muscle in the right forearm which was observed during routine cadaver dissection of a male cadaver aged about 65 yrs in the department of Shareera Rachana at Sri Dharmasthala Manjunatheshwara College of Ayurveda & Hospital, Hassan, Karnataka, India. The variation was compared with the presence of palmaris longus muscle of left limb and other possible variations of palmaris longus muscle reported in the literature. The prevalence of absence, related variations, clinical importance & evolutionary aspect of palmaris longus muscle has been discussed in the paper. Keywords: Palmaris longus, Flexor muscle, Variation INTRODUCTION skin in grasping objects by tensing it. The Palmaris longus is a slender fusiform muscle is supplied by branches of ulnar muscle medial to flexor carpi radialis. It artery & median nerve. -

Day 1: Dry Lab Stations Pod 2. Nerve Identification for NCS Confirmed By
Day 1: Dry Lab Stations There will be 3 pods teaching on the areas described below with 3 stations at each pod. Participants will be placed in groups of 4-5 and rotate to each pod throughout the afternoon. There will be 1 faculty lead at each pod and 3 faculty assistants. Pod 1. PEX: Physical Exam Skills Confirmed by Ultrasound - Acromioclavicular joint - Biceps tendon - Supraspinatus tendon - Lateral epicondyle - Medial epicondyle - Ulnar nerve/cubital tunnel - Medial joint line of the knee - Lateral joint line of the knee - Quadriceps tendon - Patellar tendon - Fibular head - Iliotibial band - MCL/LCL - Pes anserine - Achilles tendon - Plantar fascia - Base of 5th metatarsal - Navicular bone - Tibiotalar joint - ATFL - Greater trochanter Pod 2. Nerve identification for NCS Confirmed by Ultrasound - Median - Ulnar - Lateral femoral cutaneous - Brachial Plexus - Tibial - Common Peroneal - Sural Pod 3. Spasticity Injection Muscle Identification Confirmed by Ultrasound - Hip flexors adductors - Posterior calf - Biceps - Brachialis/brachioradialis - Flexor carpi ulnaris - Flexor digitorum profundus - Pronator qudratus - Flexor digitorum superficialis - Flexor carpi radialis - Pronator teres - Flexor pollicis longus Day 1 and 2: Cadaver Stations There will be 10 stations teaching on areas as described below. Participants will be placed in groups of 4 and rotate to each station throughout the rest of the course. There will be one faculty member at each station. Station 1. Shoulder Injections - AC joint - GH joint - Biceps tendon sheath - Subacromia/subdeltoid bursa Station 2. Knee Injections - Suprapatellar bursa - Pes anserine bursa - Patellar tendon tenotomy Station 3. Wrist and Hand Injections - Carpal tunnel - APL/EPB tendon sheath at the wrist - Finger flexor tendon sheath - CMC joint Station 4. -

Morphometric Study and Occurrence of the Palmaris Longus Muscle in Human Fetuses
MOJ Anatomy & Physiology Research Article Open Access Morphometric study and occurrence of the palmaris longus muscle in human fetuses Abstract Volume 7 Issue 1 - 2020 Introduction: The palmaris longus muscle has a short belly and a long tendon, it is located in the superficial layer of the anterior compartment of the forearm and usually has insertions José Aderval Aragão,1,4 Julio Cezar de in the medial humeral epicondyle and palmar aponeurosis. As it is an accessory muscle in Oliveira Filho,2 Otávio Vinicius Nascimento wrist flexion, its absence does not cause functional impairment and its tendon is used as de Oliveira,2 Layla Raíssa Dantas Souza,2 a graft in many surgical procedures. This study aimed to determine the occurrence of the Bianca Holz Vieira,2 Iapunira Catarina palmaris longus muscle and its musculotendinous relations. Sant’Anna Aragão,3 Felipe Matheus Sant’Anna Methods: 20 forearms of 10 fetuses were dissected, with ages ranging from 19.6 to 37.8 Aragão,3 Francisco Prado Reis4 weeks of gestation, belonging to the anatomy laboratory of the Federal University of 1Department of Morphology, Federal University of Sergipe Sergipe. The belly and tendon length of the palmaris longus muscle were measured using a (UFS), Brazil 0.01mm precision digital caliper. 2Department of Medicine, Federal University of Sergipe (UFS), Brazil Results: The palmaris longus muscle was present in all cases. The length of the palmaris 3 longus muscle (PLM) was slightly longer on the right side, with its muscular belly being Medical School, University Center of Volta Redonda (UNIFOA), larger in the left dimidium and its tendon in the right. -

ANATOMY of the ELBOW and FOREARM Medial Cutaneous Nerve of Forearm Biceps Brachii Muscle Ulnar Nerve
ANATOMY OF THE ELBOW AND FOREARM Medial cutaneous nerve of forearm Biceps brachii muscle Ulnar nerve Brachial artery and median nerve Triceps brachii muscle Medial intermuscular septum Triceps brachii muscle Lateral cutaneous nerve of forearm (terminal musculocutaneous nerve) Ulnar artery Brachialis muscle Medial epicondyle of humerus Biceps brachii tendon Radial artery Common flexor tendon Brachioradialis muscle Bicipital aponeurosis Pronator teres muscle Extensor carpi radialis longus muscle Superior ulnar collateral artery Flexor carpi (anastomoses distally with Brachioradialis muscle Ulnar nerve radialis muscle posterior ulnar recurrent artery) Extensor carpi Medial epicondyle radialis longus muscle Palmaris longus of humerus Common extensor tendon muscle Superficial Flexor carpi Extensor carpi flexor Extensor carpi radialis brevis muscle ulnaris muscle radialis brevis muscle muscles Olecranon of ulna Extensor digitorum muscle Flexor digitorum Anconeus muscle superficialis muscle Flexor pollicis longus Palmaris longus tendon Flexor carpi ulnaris muscle Extensor digiti minimi muscle muscle and tendon Dorsal branch of ulnar nerve Radial artery Extensor carpi ulnaris muscle Ulnar artery and nerve Abductor pollicis longus muscle Median nerve Flexor digitorum superficialis tendon Palmar carpal ligament Pisiform Extensor pollicis brevis muscle (continuous with extensor retinaculum) Palmar branch of median nerve Thenar muscles Hypothenar muscles Extensor pollicis longus tendon Extensor carpi radialis brevis tendon Extensor carpi radialis