Appendix 2015-45 Pharmaceutical Care Services Plan
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
1 Apologies for Absence
GAVINTON, FOGO & POLWARTH COMMUNITY COUNCIL Minutes of Meeting held in Gavinton Village Hall . : on Monday, 29 October, 2001 at 7.00pm PRESENT: Mrs B Darling (Chairman), Mrs CAllm-an, MrSBrodie, Mr A Macmillan, Mr D Paterson, Mrs F Renton, Mr F Seed. Councillor W L Forrest Mrs J Wheadon (Committee Secretary). 4 members of the public. 1 APOLOGIES FOR ABSENCE Apologies were received from Mr I Gill, Mrs U Robinson and Mr B Weir. 2 MINUTES OF MEETING HELD ON 17 SEPTEMBER 2001 The Minutes, which had previously been circulated, were signed by the Chairman as a correct copy. 3 MATTERS ARISING 3,14(c) Basketball net on Gavinton village green - Mary Weir and the original sub-committee said that the net could be removed but what would happen to it had not been decided. 8(a) Bonfire night - there was to be a bonfire in the playing field. Thanks to all volunteers and Mr D Seed for providing a straw bale. 4 LOTHIAN AND BORDERS POLICE WPC Rachael Mackey and WPC Karen Parker attended to hear our concerns regarding speeding through Gavinton. In July there had been a speeding check in the village and one person had been caught Due to pressure on resources manpower was concentrated on accident or crash hotspots to ascertain why these occurred and as no accidents had been reported, Gavinton was not considered a problem. It was suggested that any concerns should be sent to the Police Traffic Department at Hawick, including the use of Main Street as a short cut to Duns industrial estate, especially early in the morning, and also the large number of children in the village. -

Military Tribunals Berwick Advertiser 1916
No. SURNAME CHRISTIAN NAME OCCUPATION PLACE DATE OF TRIBUNAL DATE OF NEWSPAPER TRIBUNAL AREA REASON FOR CLAIM RESULT OF TRIBUNAL PRESIDING OFFICER INFO 1 BOYD DAVID Sanitary inspector Berwick 25/02/1916 03/03/1916 BA BERWICK In the national interests, he said his services were indispensible in the interests of the health of the community. Claim refused Mr D. H. W. Askew Employed as the sanitary inspector for the borough of Berwick, he said he was happy to serve if the court decided. There was a long discussion and it was decided that his job could be done by someone unqualified. 2 UNIDENTIFIED UNIDENTIFIED Land agents assistant UNIDENTIFIED 25/02/1916 03/03/1916 BA BERWICK UNIDENTIFIED Temporary exemption granted until 31st May Mr D. H. W. Askew Case heard in private. 3 UNIDENTIFIED UNIDENTIFIED Dentist's assistant UNIDENTIFIED 25/02/1916 03/03/1916 BA BERWICK Indispensible to the business Temporary exemption granted Mr D. H. W. Askew Case heard in private. 4 UNIDENTIFIED UNIDENTIFIED Grocer's assistant UNIDENTIFIED 25/02/1916 03/03/1916 BA BERWICK Domestic hardship Temporary exemption granted until 31st August Mr D. H. W. Askew He had 3 brothers and one sister. His father had died 2 years before the war. One brother had emigrated to New Zealand and had been declared as unfit for service, another had emigrated to Canada and was currently serving in France, and the other brother had served in the territorial army, went to France to serve and had been killed. His only sister had died just before the war, he said he was willing to serve, but his mother did not want him to go, having lost one son 5 UNIDENTIFIED UNIDENTIFIED UNIDENTIFIED UNIDENTIFIED 25/02/1916 03/03/1916 BA BERWICK Domestic hardship Temporary exemption granted until 31st August Mr D. -

Grantshouse Community Council
Grantshouse Community Council Thursday 14th April 2016 at 7.30pm in Grantshouse Village Hall If anyone attending these meetings, whether addressing the Community Council or not, should let the Chairman, Vice Chairman or Secretary know if they wish to have their names omitted from any comments. If there are no declarations, it will be presumed that there are no objections. AGENDA Approximate Time 1. Apologies 1 min 2. Police Scotland 5 min 3. Neighbourhood Watch Report 5 min 4. NTR 15 min 5. Previous Minutes 5 min 6. Matters Arising 20 min 7. Treasurers Report 5 min 8. Correspondence 10 min 9. Drone Hill Apps 10 min 10. Broadband 5 min 11. Any Other Business 10 min 12. Date of Next Meeting Thursday 12th May 2016 Anyone is welcome to attend and contributions are encouraged from anyone in the community. 1 Grantshouse Community Council Thursday 10th March 2016 in Grantshouse Village Hall Present: John Prentice (Chairman), Kym Bannerman, Marion Donovan, Pat Durie, Ian Fleming, Margaret Fleming, Walter Wyse (NHW Coordinator), Joan Campbell (Councillor), Martin Sweeney (NTR Plc), Robert Thomson (NTR Plc) Apologies: Pat Durie, PC Richard Toward (Police Scotland) and Michael Cook (Councillor) NTR Plc: Martin Sweeney (NTR) wanted to introduce himself and Robert Thomson (NTR) as Manager and Site Manager of the Quixwood Wind Farm Development. Martin has asked if there are any issues relating to the installation of the Wind Farm to be contacted by the CC. NTR started off as National Toll Roads in Dublin but now they invest in Wind Farms and build and run them for their lifespan. -

Act 1994 Scottish Borders Council Community Council
ADOPTED 2007 LOCAL GOVERNMENT ETC. (SCOTLAND) ACT 1994 SCOTTISH BORDERS COUNCIL COMMUNITY COUNCIL SCHEME 1.0 Introduction 1.1 The Scottish Borders Council, in accordance with the terms of Section 22 of the Local Government etc. (Scotland) Act 1994 has adopted the following Community Council Scheme for the operation of Community Councils within the Scottish Borders Council area, and has revoked the previous Scheme adopted by Scottish Borders Council in 1997, with effect from midnight on 13 December 2007. 2.0 Purpose of Community Councils 2.1 In addition to any other purpose which a Community Council may pursue, the general purpose of a Community Council shall be to ascertain, co-ordinate and express to the Local Authority for its area, and to public authorities, the views of the community which it represents in relation to matters for which those authorities are responsible, and to take such action in the interests of that community as appears to it to be expedient and practicable. 3.0 Procedure for Establishment of Community Councils 3.1 In the event of not less than 20 electors in any one of the areas listed in Schedule 1 to this Scheme, and shown delineated on the maps (numbered 1 - 67) annexed to the principal copy of this Scheme, with the exception of Bowden, for the reasons stated in Clause 3.2 below, making written application for the establishment of a Community Council for that area in accordance with this Scheme, the Scottish Borders Council shall, within six weeks from the date of the petition, invite nominations and thereafter, if necessary, organise an election for the establishment of a Community Council for that area. -

Engagement Report
2 | P a g e Engagement report “The Integration Authority must also publish a statement at the same time it publishes its strategic commissioning plan, which describes the consultation it undertook.” (From Public Bodies (Joint Working) (Scotland) Act 2014). Table of Contents ................................................................................................................................................................ 1 Introduction ........................................................................................................................................ 4 Our Vision ............................................................................................................................................ 4 Users Engagement Policy .................................................................................................................... 4 Principles of Engagement ................................................................................................................... 4 Methods of Communication and Engagement ............................................................................... 5 Communications Principles and Standards..................................................................................... 6 Target Audience .............................................................................................................................. 6 Role of the Strategic Planning Group ................................................................................................. -

Heritage Festival 2017
Heritage Festival 2017 Where People, Place & Myth Meet PROGRAMME OF EVENTS PICTURING THE PAST: LIGHTING THE BORDERS PHOTOGRAPHY COMPETITION Lantern making workshops Entries by midnight, Friday 11 August 2017 11 August, 11.00–13.00 & 14.00–17.00 Live Borders Libraries & Archives, Newcastleton Village Hall, Newcastleton St Mary’s Mill, Selkirk TD7 5EW TD9 0QD. Parade: Sat 2 September meeting Entry Free at 20.00, Hermitage Castle, Newcastleton Celebrate Scotland’s Year of History, 12 August, 11.00–13.00 & 14.00–17.00 Heritage & Archaeology by capturing Duns Parish Hall, Church Square, Duns TD11 your Borders heritage through photography. 3DD. Parade: Friday 1 September meeting Do you have a favourite building, monument at 19.00 Market Square, Duns or archaeological feature in the Scottish Come along and make your own willow Borders? Why not get out and about with and tissue paper lantern for our spectacular your camera this summer? Entering is easy! public parades in Duns and Newcastleton! 1. You must be within one of these three These workshops are free with a small categories when the competition closes: donation (£2) towards materials appreciated. 11 years and under, 12–17 years, 18–25 years. Wear old clothes and bring your family 2. Download an entry form, which includes along. Drop in sessions – please allow at full conditions of entry: www.liveborders. least 1 hour to make your lantern. For more org.uk/librariesandarchives information on lantern making workshops please contact Sara. 3. A digital copy of the image along with the completed entry form must be submitted via &[email protected] email to [email protected]. -
Prevention of Homelessness Application Form
PREVENTION OF HOMELESSNESS APPLICATION FORM Priority for “Prevention of Homelessness” is awarded at Silver level. A Silver priority pass will be issued to persons assessed by either Scottish Borders Council (SBC) or BHA as being threatened with homelessness. Examples of this include, but are not limited to: Relationship breakdown (non-BHA tenants) Living in an insecure tenancy such as tied accommodation or having a Short Assured Tenancy which is coming to an end within 2-6 months Having a relationship breakdown with parents or another occupant of the home Having financial difficulties in making rent or mortgage payments within the current home Is living in a mobile home (not static) In order to assess your Prevention of Homelessness Priority application, please complete form in full. APPLICATION: Homehunt Registration Number ___________________ Your Name ____________________________________________________________________________ Your Address ___________________________________________________________________________ Telephone: Home _________________ Work _________________ Mobile ________________________ Prevention of Homelessness Have you/are you had a relationship breakdown and are a non-BHA tenant? Yes No if Yes, please give details of your relationship __________________________________________ ________________________________________________________________________________ living in an insecure tenancy such as tied accommodation Yes No or having a Short Assured Tenancy which is coming to an end within 2-6 months? if “Yes”, -
Relationship Breakdown (Bha Tenant) Information/Application Form
STATUTORILY HOMELESSNESS/ RELATIONSHIP BREAKDOWN (BHA TENANT) INFORMATION/APPLICATION FORM If you wish to make a homeless application you should apply immediately to your Local Authority (in the Scottish Borders area this is Scottish Borders Council). You can access the homeless service through any Scottish Borders Council Contact Centre or by contacting the homeless service direct at the address below. Your Local Authority will discuss housing options with you. If Scottish Borders Council accepts a duty to house you as a homeless person and refers you to Berwickshire Housing Association, then you will receive Gold Priority for housing. If Scottish Borders Council does not accept a duty to house you but nevertheless deems you are in significant housing need and/or at risk of becoming homeless, you may qualify for bronze priority if a referral is made and confirmation of your housing options agreement is received. Finally, if you wish to make a homeless application to the Scottish Borders Council from another Local Authority area your Local Authority can, in certain circumstances, make a ’homeless referral’ to Scottish Borders Council. For more information contact your own Local Authority. Scottish Borders Council, Homelessness Services, Paton Street, Galashiels TD1 1AS Tel: 01896 661 385 Out of Hours Service Bordercare: 01896 752111 Freephone Number 0800 376 1138 Additionally, BHA will award a Gold pass to existing BHA tenants demonstrating relationship breakdown. In order to assess your Relationship Breakdown (BHA Tenant) Priority application, -
Copy of List of Public Roads
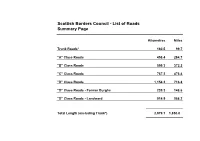
Scottish Borders Council - List of Roads Summary Page Kilometres Miles Trunk Roads* 160.5 99.7 "A" Class Roads 458.4 284.7 "B" Class Roads 599.3 372.2 "C" Class Roads 767.2 476.4 "D" Class Roads 1,154.2 716.8 "D" Class Roads - Former Burghs 239.3 148.6 "D" Class Roads - Landward 914.9 568.2 Total Length (excluding Trunk*) 2,979.1 1,850.0 Trunk Roads (Total Length = 160.539 km or 99.695 Miles) Classification / Route Description Section Length Route No. A1 London-Edinburgh- From boundary with Northumberland at Lamberton Toll to boundary with 29.149 km 18.102 miles Thurso East Lothian at Dunglass Bridge A7 Galashiels-Carlisle From the Kingsknowe roundabout (A6091) by Selkirk and Commercial 46.247 km 28.719 miles Road, Albert Road and Sandbed, Hawick to the boundary with Dumfries & Galloway at Mosspaul. A68 Edinburgh-Jedburgh- From boundary with Midlothian at Soutra Hill by Lauder, St. Boswells and 65.942 km 40.95 miles Newcastle Jedburgh to Boundary with Northumberland near Carter Bar at B6368 road end A702 Edinburgh-Biggar- From Boundary with Midlothian at Carlops Bridge by West Linton to 10.783 km 6.696 miles Dumfries Boundary with South Lanarkshire at Garvald Burn Bridge north of Dolphinton. A6091 Melrose Bypass From the Kingsknowe R'bout (A7) to the junction with the A68 at 8.418 km 5.228 miles Ravenswood R'bout "A" Class Roads (Total Length = 458.405 km or 284.669 Miles) Classification / Description Section Length Route Route No. A7 Edinburgh-Galashiels- From the boundary with Midlothian at Middleton by Heriot, Stow and 31.931 km 19.829 miles Carlisle Galashiels to the Kingsknowe R'bout (A6091) A1107 Hillburn-Eyemouth- From A1 at Hillburn by Redhall, Eyemouth and Coldingham to rejoin A1 at 21.509 km 13.357 miles Coldingham-Tower Tower Farm Bridge A697 Morpeth-Wooler- From junction with A698 at Fireburnmill by Greenlaw to junction with A68 38.383 km 23.836 miles Coldstream-Greenlaw- at Carfraemill. -

Update to Win Berwickshire an Ipad Housing Association
Summer 2019 YOUR CHANCE UPDATE TO WIN BERWICKSHIRE AN IPAD HOUSING ASSOCIATION CHIRNSIDE DEVELOPMENT REFLECTS Glebe Place in Chirnside is the latest of our affordable and LOCAL DEMAND energy efficient housing developments to be completed. Our vision of creating Scottish Government, with BHA and Angela Taylor, BHA’s Property Director, said: thriving rural communities the Scottish Government providing the “BHA is delighted with the high quality of is there for all to see funding to develop these much needed, these homes and standard of this new following the completion new affordable homes. development. These 25 homes provide a range of house types which people can of our new affordable and As with all of BHA’s new-build homes afford to rent, are energy efficient and energy efficient housing they are of a very high standard when it warm, and are much needed in the area.” development in Chirnside. comes to energy efficiency. During the construction, Hart Builders were Reflecting local demand, this 25 unit This new development was built by Hart particularly pleased to offer a local school development at Glebe Place is a good mix Builders and Smith Scott Mullen. pupil (and neighbour to the development) a of housing types and flats suitable for During the construction phase Hart placement on site to gain work experience individuals and families. Builders recruited all of their joiners and and an overview of the career opportunities BHA has worked in partnership with labourers locally and several Borders firms available to her in construction. Scottish Borders Council (SBC) and the were sub-contracted. -

Domestic Abuse Pass Form
DOMESTIC ABUSE APPLICATION FORM Priority for “Domestic Abuse” is awarded at Platinum level. Domestic Abuse priority is awarded in the following circumstances: You need to move to prevent domestic abuse within your current property Or You are currently staying in temporary refuge accommodation (eg. with Women’s Aid) and need your own home And You have not been assessed by your local authority as homeless BHA work closely with Scottish Borders Council (SBC) to tackle Domestic Abuse. Where an applicant has been identified as at high risk via a Multi-Agency Risk Assessment Committee (MARAC), then they will be awarded a Platinum priority pass. If your local authority has accepted that you are Homeless due to domestic abuse, please complete the Homeless priority pass form. If you are currently at risk of abuse and/or require support due to domestic abuse, please contact one of the following agencies: Call 999 if there is a risk to your safety or that of a family member Call Police Scotland on 101 if you wish to report an incident Call Scotland’s Domestic Abuse and Forced Marriage Helpline on 0800 027 1234 Go to https://sdafmh.org.uk/ or https://womensaid.scot/ If you have nowhere to stay due to fleeing abuse, contact your local council (see contact details on Homeless Priority Pass) In order to assess your Domestic Abuse Priority application, please complete form in full. APPLICATION: Homehunt Registration Number ___________________ Your Name ____________________________________________________________________________ Your Address ___________________________________________________________________________ Telephone: Home _________________ Work _________________ Mobile ________________________ Domestic Abuse situation Are you: Needing to move to prevent domestic abuse in your current property? Yes No if Yes, please give contact details of any supporting agency which can confirm your need for re- housing (eg. -

Health and Social Care News Update
SCOTTISH BORDERS COUNCIL and NHS BORDERS Health and Social Care News Update Issue 7 – Winter 2017/18 In this issue .... • IT Integration Project Welcome to the health and • Major investment in Waverley Care Home and Community social care news update Equipment Service unveiled Colleagues, • Integration Joint Board update I am delighted to introduce the Winter • Joint Older People’s edition of the Health and Social Care Inspection News Update. • Carers (Scotland) Act You will see from this edition we are in a Implementation time of great change and I look forward • General Manager Patient to working with you all to meet the Pathways – Dr Jane Prior challenges that lie ahead • Locality Plan consultation • Commissioning and During the ten weeks or so that I have Implementation Plan been in post, I have tried to get out and • Scottish Borders Mental about as much as I can and have been Health Strategy really encouraged by what I have seen • Alcohol related brain damage so far. I have been throughout the BGH conference held and Kelso Community Hospital, visited I’ve also met with unions and staff • Scottish Borders Seniors teams in Mental Health and Learning representatives in what I felt was a very Networking Forum (SBSNF) Disability and seen first-hand some of forward looking and exciting exchange • Men’s Sheds make progress the work they undertake. I’ve talked with of views and ideas. They are already • Community equipment homecare providers, district nurses, our well on their way with arrangements to amnesty GP fraternity, occupational therapists, support the partnership of Council and • Other news in brief speech therapists, physios, social NHS staff and we have agreed to meet workers and health care assistants.