Oral Mucormycosis in an Immunocompetent Patient: a Case
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Estimated Burden of Serious Fungal Infections in Ghana
Journal of Fungi Article Estimated Burden of Serious Fungal Infections in Ghana Bright K. Ocansey 1, George A. Pesewu 2,*, Francis S. Codjoe 2, Samuel Osei-Djarbeng 3, Patrick K. Feglo 4 and David W. Denning 5 1 Laboratory Unit, New Hope Specialist Hospital, Aflao 00233, Ghana; [email protected] 2 Department of Medical Laboratory Sciences, School of Biomedical and Allied Health Sciences, College of Health Sciences, University of Ghana, P.O. Box KB-143, Korle-Bu, Accra 00233, Ghana; [email protected] 3 Department of Pharmaceutical Sciences, Faculty of Health Sciences, Kumasi Technical University, P.O. Box 854, Kumasi 00233, Ghana; [email protected] 4 Department of Clinical Microbiology, School of Medical Sciences, Kwame Nkrumah University of Science and Technology, Kumasi 00233, Ghana; [email protected] 5 National Aspergillosis Centre, Wythenshawe Hospital and the University of Manchester, Manchester M23 9LT, UK; [email protected] * Correspondence: [email protected] or [email protected] or [email protected]; Tel.: +233-277-301-300; Fax: +233-240-190-737 Received: 5 March 2019; Accepted: 14 April 2019; Published: 11 May 2019 Abstract: Fungal infections are increasingly becoming common and yet often neglected in developing countries. Information on the burden of these infections is important for improved patient outcomes. The burden of serious fungal infections in Ghana is unknown. We aimed to estimate this burden. Using local, regional, or global data and estimates of population and at-risk groups, deterministic modelling was employed to estimate national incidence or prevalence. Our study revealed that about 4% of Ghanaians suffer from serious fungal infections yearly, with over 35,000 affected by life-threatening invasive fungal infections. -

Fundamental Medical Mycology Errol Reiss
Fundamental Medical Mycology Fundamental Medical Mycology Errol Reiss Mycotic Diseases Branch, Centers for Disease Control and Prevention, Atlanta, Georgia H. Jean Shadomy Department of Microbiology and Immunology, Virginia Commonwealth University, School of Medicine, Richmond, Virginia G. Marshall Lyon, III Department of Medicine, Division of Infectious Diseases, Emory University, School of Medicine, Atlanta, Georgia A JOHN WILEY & SONS, INC., PUBLICATION This book was written by Errol Reiss in his private capacity. No official support or endorsement by the Centers for Disease Control and Prevention, Department of Health and Human Services is intended, nor should be inferred. Copyright 2012 by Wiley-Blackwell. All rights reserved Published by John Wiley & Sons, Inc., Hoboken, New Jersey Published simultaneously in Canada No part of this publication may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, scanning, or otherwise, except as permitted under Section 107 or 108 of the 1976 United States Copyright Act, without either the prior written permission of the Publisher, or authorization through payment of the appropriate per-copy fee to the Copyright Clearance Center, Inc., 222 Rosewood Drive, Danvers, MA 01923, (978) 750-8400, fax (978) 750-4470, or on the web at www.copyright.com. Requests to the Publisher for permission should be addressed to the Permissions Department, John Wiley & Sons, Inc., 111 River Street, Hoboken, NJ 07030, (201) 748-6011, fax (201) 748-6008, or online at http://www.wiley.com/go/permission. Limit of Liability/Disclaimer of Warranty: While the publisher and author have used their best efforts in preparing this book, they make no representations or warranties with respect to the accuracy or completeness of the contents of this book and specifically disclaim any implied warranties of merchantability or fitness for a particular purpose. -

Sporothrix Schenckii: ➢ Thermal Dimorphic
Subcutaneous mycoses ➢1-Mycetoma ➢2-Sporotrichosis ➢3-Chromoblastomycosis ➢4-Rhinosporidiosis ➢5- Lobomycosis ➢6- Entomophthoramycosis Sporotrichosis Rose gardener’s disease Chronic desease Agent Sporothrix schenckii: ➢ Thermal dimorphic ➢ In soil ➢ On decaying vegetation,plants,plant products (hay, straw, sphagnum moss), and a variety of animals (cats) ➢ less than 37° C (hyphal) ➢ 37° C (yeast) ➢ Sporothrix brasiliensis ➢ Sporothrix globosa Epidemiology ➢Worldwide ➢Tropical regions ➢Mexico ➢Brazile ➢France ➢USA Occupational disease: ➢Farmers ➢ ➢Workers ➢Gardeners ➢Florists Predisposing factors: ➢Trauma ➢Inhalation (very rarely) ➢HIV Clinical Syndromes 1-lymphocutaneous 2-Fixed cutaneous 3- Osteoarticular involvement 4-Pulmonary 5-Systemic Primary infection 1-Lymphocutaneous sporotrichosis 2-Fixed cutaneous sporotrichosis: Fixed cutaneous sporotrichosis verrucous-type sporotrichosis localized cutaneous type Paronychia sporotrichosis Osteoarticular involvement Pulmonary sporotrichosis: ➢Alcoholic ➢Pulmonary tuberculosis, diabetes mellitus and steroid ➢A productive cough ➢Low-grade fever ➢Weight loss Systemic sporotrichosis Transmission: ➢Dog bite ➢parrot bite ➢Insects bite ➢Cases of animal-to-human transmission Laboratory Diagnosis: 1-Collection of samples: ➢Drainage from skin lesions ➢Exudates ➢Pus ➢Blood ➢Pulmonary secretions ➢Tissue biopsy specimens 2-Direct examination ➢Gram ➢PAS ➢GMS ➢H & E ❖Yeast Cells ❖Asteroid body: Elongated Buds (“Cigar Body”) Wet Mount BHI Blood 37˚C Yeast with Elongated Daughter Cell Biopsy of subcutaneous tissue -

Histopathology of Important Fungal Infections
Journal of Pathology of Nepal (2019) Vol. 9, 1490 - 1496 al Patholo Journal of linic gist C of of N n e o p ti a a l- u i 2 c 0 d o n s 1 s 0 a PATHOLOGY A m h t N a e K , p d of Nepal a l a M o R e d n i io ca it l A ib ss xh www.acpnepal.com oc g E iation Buildin Review Article Histopathology of important fungal infections – a summary Arnab Ghosh1, Dilasma Gharti Magar1, Sushma Thapa1, Niranjan Nayak2, OP Talwar1 1Department of Pathology, Manipal College of Medical Sciences, Pokhara, Nepal. 2Department of Microbiology, Manipal College of Medical Sciences , Pokhara, Nepal. ABSTRACT Keywords: Fungus; Fungal infections due to pathogenic or opportunistic fungi may be superficial, cutaneous, subcutaneous Mycosis; and systemic. With the upsurge of at risk population systemic fungal infections are increasingly common. Opportunistic; Diagnosis of fungal infections may include several modalities including histopathology of affected tissue Systemic which reveal the morphology of fungi and tissue reaction. Fungi can be in yeast and / or hyphae forms and tissue reactions may range from minimal to acute or chronic granulomatous inflammation. Different fungi should be differentiated from each other as well as bacteria on the basis of morphology and also clinical correlation. Special stains like GMS and PAS are helpful to identify fungi in tissue sections. INTRODUCTION Correspondence: Dr Arnab Ghosh, MD Fungal infections or mycoses may be caused by Department of Pathology, pathogenic fungi which infect healthy individuals or by Manipal College of Medical Sciences, Pokhara, Nepal. -
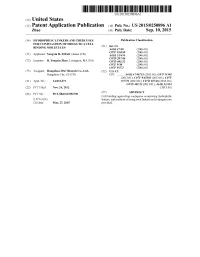
(12) Patent Application Publication (10) Pub. No.: US 2015/0250896 A1 Zhao (43) Pub
US 20150250896A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2015/0250896 A1 Zhao (43) Pub. Date: Sep. 10, 2015 (54) HYDROPHILIC LINKERS AND THEIR USES Publication Classification FOR CONUGATION OF DRUGS TO A CELL (51) Int. Cl BNDING MOLECULES A647/48 (2006.01) (71) Applicant: Yongxin R. ZHAO, Henan (CN) Ek E. 30.8 C07D 207/216 (2006.01) (72) Inventor: R. Yongxin Zhao, Lexington, MA (US) C07D 40/12 (2006.01) C07F 9/30 (2006.01) C07F 9/572 (2006.01) (73) Assignee: Hangzhou DAC Biotech Co., Ltd., (52) U.S. Cl. Hangzhou City, ZJ (CN) CPC ........... A61K47/48715 (2013.01); C07F 9/301 (2013.01); C07F 9/65583 (2013.01); C07F (21) Appl. No.: 14/432,073 9/5721 (2013.01); C07D 207/46 (2013.01); C07D 401/12 (2013.01); A61 K3I/454 (22) PCT Filed: Nov. 24, 2012 (2013.01) (86). PCT No.: PCT/B2O12/0567OO Cell(57) binding- agent-drugABSTRACT conjugates comprising hydrophilic- S371 (c)(1), linkers, and methods of using Such linkers and conjugates are (2) Date: Mar. 27, 2015 provided. Patent Application Publication Sep. 10, 2015 Sheet 1 of 23 US 2015/0250896 A1 O HMDS OSiMe 2n O Br H-B-H HPC 3 2 COOEt essiop-\5. E B to NH 120 °C, 2h OsiMe3 J 50 °C, 2h eSiO OEt 120 oC, sh 1 2 3. 42% from 1 Bra-11a1'oet - Brn 11-1 or a 1-1 or ÓH 140 °C ÓEt ÓEt 4 5 6 - --Messio. 8 B1a-Br aus 20 cc, hP-1}^-'ot Br1-Y. -

Mucormycosis and Entomophthoramycosis (Zygomycosis) by Assistant Prof
Mucormycosis and Entomophthoramycosis (Zygomycosis) By Assistant Prof. Dr. Thekra Ahmed Fungi causing Subcutaneous Zygomycosis • Classification based on molecular phylogenetic studies of rRNA, tef1, and rpb1, has abolished the class Zygomycetes and instead distributes fungi previously in the phylum Zygomycota into the phylum Glomeromycota and four subphyla, including Mucoromycotina, Kickxellomycotina, Zoopagomycotina, and Entomophthoromycotina. Mycology • Fungi of the order Mucorales are classified into six different families based on morphologic analysis of the fungi, including the presence and location of rhizoids, the presence of apophyses, and the morphology of the columellae. Other taxonomically relevant features include carbohydrate assimilation and the maximal growth temperature. Zygomycosis (Mucorales). Mucorales infections Definition: •Angiotropic (blood vessel-invading) •The most common genera causing disease are: Rhizopus Rhizomucor Mucor Absidia •Fast growing non-septate molds Epidemiology • Agents of mucormycosis are ubiquitous and thermotolerant organisms that usually grow in decaying matter, including bread, vegetables, fruits, and seeds. They can also be recovered from soil, compost piles, and animal excreta. Most of the Mucorales can grow and sporulate abundantly on any carbohydrate- containing source. • Abundant growth with sporulation is usually seen in culture media within 2–5 days. The spores are easily airborne, and Mucorales are readily recovered as contaminants in laboratory cultures. • Indeed, the ability of R. -

Chromoblastomycosis in Solid Organ Transplant Recipients
Current Fungal Infection Reports (2019) 13:139–145 https://doi.org/10.1007/s12281-019-00351-9 FUNGAL INFECTIONS OF SKIN AND SUBCUTANEOUS TISSUE (A BONIFAZ AND M PEREIRA, SECTION EDITORS) Chromoblastomycosis in Solid Organ Transplant Recipients Raaka Kumbhakar1 & Benjamin A. Miko2 Published online: 7 November 2019 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Purpose of review There is growing recognition of melanized fungi as uncommon but important causes of infection among solid organ transplant recipients. Chromoblastomycosis and phaeohyphomycosis exist at opposing ends of the spectrum of disease caused by these fungi. We aim to systematically review the reports of chromoblastomycosis among transplant recipients to assess for trends in epidemiology and clinical outcomes. Recent Findings We identified 19 reported cases of histologically confirmed chromoblastomycosis among solid organ transplant recipients published between 1985 and 2018. Despite these patients’ impaired immunity, chromoblastomycosis remained local- ized to the skin and subcutaneous tissue in the majority of patients. Clinical outcomes were generally good with medical, surgical, or combined management. Summary Although chromoblastomycosis has a low incidence in this population, it is important to consider as a cause of chronic, non-healing skin infections. Further research is needed to better elucidate the impact of transplantation on the natural course of this condition. Keywords Chromoblastomycosis . Melanized fungi . Dematiaceous fungi . Transplantation Introduction CBM dematiaceous fungal infections, entities that are clinically and pathologically distinct [1–3]. Chromoblastomycosis (CBM) falls under the umbrella of “im- plantation mycosis” or “subcutaneous mycoses.” Its precise def- inition in the literature is made difficult by differentiation from phaeohyphomycosis (PHM), a term for other melanized, or Microbiology dematiaceous, fungal infections. -

Cutaneous Mucormycosis in a Diabetic Patient Following Traditional Dressing
Hindawi Publishing Corporation Case Reports in Dermatological Medicine Volume 2013, Article ID 894927, 3 pages http://dx.doi.org/10.1155/2013/894927 Case Report Cutaneous Mucormycosis in a Diabetic Patient following Traditional Dressing Zahra Ahmadinejad,1 Hamideh Khazraiyan,1 Fahime Ghanbari,1 Bahram Ahmadi,2 and Mohsen Gerami Shoar2 1 Department of Infectious Diseases, Imam Khomeini Hospital, Tehran University of Medical Sciences, Keshavarz Boulevard, Tehran 14195, Iran 2 Department of Medical Mycology and Parasitology, Tehran University of Medical Sciences, Tehran 14195, Iran Correspondence should be addressed to Zahra Ahmadinejad; [email protected] Received 26 May 2013; Accepted 6 July 2013 Academic Editors: G. E. Pierard´ and E. Schmidt Copyright © 2013 Zahra Ahmadinejad et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Cutaneous mucormycosis is a rare manifestation of an aggressive fungal infection. Early diagnosis and treatment are vitally important in improving outcome. We report an unusual case presenting with progressive necrotizing fasciitis due to mucormycosis following trauma and dressing by man-made herbal agents. 1. Introduction which resulted in wrist dislocation. The patient had been visited by an alternative practitioner and a wrist reduction Mucormycosis is a rare infection. The infection is more com- was done unprofessionally for her. He bandaged up her wrist mon among people with suppressed immune systems, but with some man-made herbal combination (including egg, it can rarely occur in healthy people. Known risk factors flour, and turmeric). for developing mucormycosis are uncontrolled diabetes mel- On the fourth day after injury, the pain was progressive litus, metabolic acidosis, high dose of corticosteroid, pro- despite herbal dressing and taking analgesic. -

Oral Entomophthoramycosis: a Rare Fungal Infection
Oral Entomophthoramycosis: A Rare Fungal Infection KD Shah*, RA Bradoo**, UV Warwantkar***, AA Joshi**** Abstract Entomophthoramycosis is a rare fungal infection which primarily affects the nose and can later spread to involve the paranasal sinuses, nasopharnyx, oropharynx, palate and the cervical region. It usually has a nodular appearance with infiltration of the underlying tissues and no clear demarcation from the surrounding tissues. We present the case of a 28 year old man, who presented with entomophthoramycosis affecting the palate, oropharynx and nasopharnyx with- out involvement of the nose. The diagnosis was confirmed by histopathology, which showed invasive mycotic inflammation, and the fungal culture revealed entomophthoramycosis. The patient was treated with oral Itraconazole (400 mg / day) for a period of one year. He responded very well to this single-drug therapy with clinical resolution of the lesion within 6 months. Further, the patient was kept under a regular follow-up for a period of one year, without any recurrence. This case is reported due to the absence of a nasal lesion of a rare fungal infection which usually originates in the nose. Introduction The disease is essentially chronic, evolving ntomophthoramycosis is a fungal over the course of years. No incubation period E infection which affects individuals with or cases of spontaneous involution are known. an apparently intact immunological status Diagnosis is made by clinical, and occurs primarily in tropical areas. Two histopathological, and mycological 4 zygomycetes belonging to the order examination. Entomophthorales are the aetiologic agents A review of medical literature indicates of subcutaneous entomophthoramycosis, viz., that the condition can be treated with Basodiobolus ranarum (= B. -

Mucormycosis: Botanical Insights Into the Major Causative Agents
Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 8 June 2021 doi:10.20944/preprints202106.0218.v1 Mucormycosis: Botanical Insights Into The Major Causative Agents Naser A. Anjum Department of Botany, Aligarh Muslim University, Aligarh-202002 (India). e-mail: [email protected]; [email protected]; [email protected] SCOPUS Author ID: 23097123400 https://www.scopus.com/authid/detail.uri?authorId=23097123400 © 2021 by the author(s). Distributed under a Creative Commons CC BY license. Preprints (www.preprints.org) | NOT PEER-REVIEWED | Posted: 8 June 2021 doi:10.20944/preprints202106.0218.v1 Abstract Mucormycosis (previously called zygomycosis or phycomycosis), an aggressive, liFe-threatening infection is further aggravating the human health-impact of the devastating COVID-19 pandemic. Additionally, a great deal of mostly misleading discussion is Focused also on the aggravation of the COVID-19 accrued impacts due to the white and yellow Fungal diseases. In addition to the knowledge of important risk factors, modes of spread, pathogenesis and host deFences, a critical discussion on the botanical insights into the main causative agents of mucormycosis in the current context is very imperative. Given above, in this paper: (i) general background of the mucormycosis and COVID-19 is briefly presented; (ii) overview oF Fungi is presented, the major beneficial and harmFul fungi are highlighted; and also the major ways of Fungal infections such as mycosis, mycotoxicosis, and mycetismus are enlightened; (iii) the major causative agents of mucormycosis -

Case Series Rhinofacial Entomophthoramycosis
SOUTHEAST ASIAN J TROP MED PUBLIC HEALTH CASE SERIES RHINOFACIAL ENTOMOPHTHORAMYCOSIS; A CASE SERIES AND REVIEW OF THE LITERATURE Juvady Leopairut1, Noppadol Larbcharoensub1, Wichit Cheewaruangroj2, Somnuek Sungkanuparph3 and Boonmee Sathapatayavongs3 1Department of Pathology, 2Department of Otolaryngology, 3Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand Abstract. Rhinofacial entomophthoramycosis is an uncommon chronic mycotic disease caused by exposure to the organism Conidiobolus coronatus. The authors report a case series of 5 patients with rhinofacial entomophthoramycosis and re- view the literature. All patients had typical involvement of the rhinofacial area with formation of subcutaneous lesions causing a chronic granulomatous inflam- matory response with tissue eosinophilia and Splendore-Hoeppli reaction. Diag- noses were made based on histopathologic examination in all cases and fungi were isolated and identified in one case. The clinicopathologic features and therapeutic management of rhinofacial entomophthoramycosis are described. Key words: entomophthoramycosis, phycomycosis, zygomycosis, Conidiobolus spp, rhinofacial INTRODUCTION 2004; Sugar, 2005; Chayakulkeeree et al, 2006). Entomophthoramycosis conidio- Rhinofacial entomophthoramycosis is balae occurs predominantly in immuno- an uncommon chronic mycotic disease in competent patients, and involves the head humans occuring in tropical and subtropi- and face. The disease is characterized by cal regions of the world. The term rhino- slowly progressive swelling of the soft tis- facial entomophthoramycosis encom- sue of the rhinofacial area and is occasion- passes various diseases caused by fungi ally mistaken for malignancy or tubercu- of the order Entomophthorales and class losis in clinical practice. Histopathologic Zygomycetes (Phycomycetes). The Ento- features reveal broad mycelial filaments mophthorales has two genera, Conidio- with infrequently septation surround by bolus and Basidiobolus, producing rhino- a Splendore-Hoeppli reaction. -

Subcutaneous Phycomycosis: a Case Report
DOI: 10.5958/2319-5886.2015.00042.9 International Journal of Medical Research & Health Sciences www.ijmrhs.com Volume 4 Issue 1 Coden: IJMRHS Copyright @2014 ISSN: 2319-5886 Received: 8th Nov 2014 Revised: 4th Dec 2014 Accepted: 25th Dec 2014 Case report SUBCUTANEOUS PHYCOMYCOSIS: A CASE REPORT *Thilak Sundararaj1, Meera Govindaraju2, Brindha Thangaraj3 1Associate Professor, 2Assistant Professor, 3PostGraduate Student, Department of Dermatology, Venereology and Leprosy, Meenakshi Medical College & Research Institute, Enathur, Kanchipuram,Tamilnadu *Corresponding author email: [email protected] ABSTRACT Subcutaneous Phycomycosis is a rare tropical Mycoses characterized by the development of a chronic, firm swelling of the subcutaneous tissue. Infection caused by Basidiobolus species commonly affects young children. In this article we present a case of Subcutaneous Phycomycosis which presented as a diffuse swelling in the posterior aspect of the knee. Early diagnosis and treatment with Itraconazole caused complete clearance of the lesion. We highlight the merits of accurate diagnosis and early therapeutic intervention in this rare case. Keywords: Phycomycosis, Basidiobolus, Conidiobolus, Subcutaneous, Aseptate hyphae INTRODUCTION Subcutaneous Phycomycosis is also called nodes were not palpable. The finger insinuation test Basidiobolomycosis, Subcutaneous Zygomycosis, was positive. Her general, physical and systemic Conidiobolomycosis, Rhinoentomophthromycosis. It examination was normal. Routine lab investigations is a rare tropical subcutaneous mycosis1. It is caused were also normal. Biopsy was done from the swelling by Basidiobolus ranarum and Conidiobolus and sent for histopathological examination and fungal coronatus2. The lesion usually starts as a small culture. subcutaneous nodule that slowly increases in size On Histopathological examination, multiple over a period of months. Lesions are usually painless eosinophilic, broad, aseptate fungal hyphae were seen and ulceration over skin is uncommon.