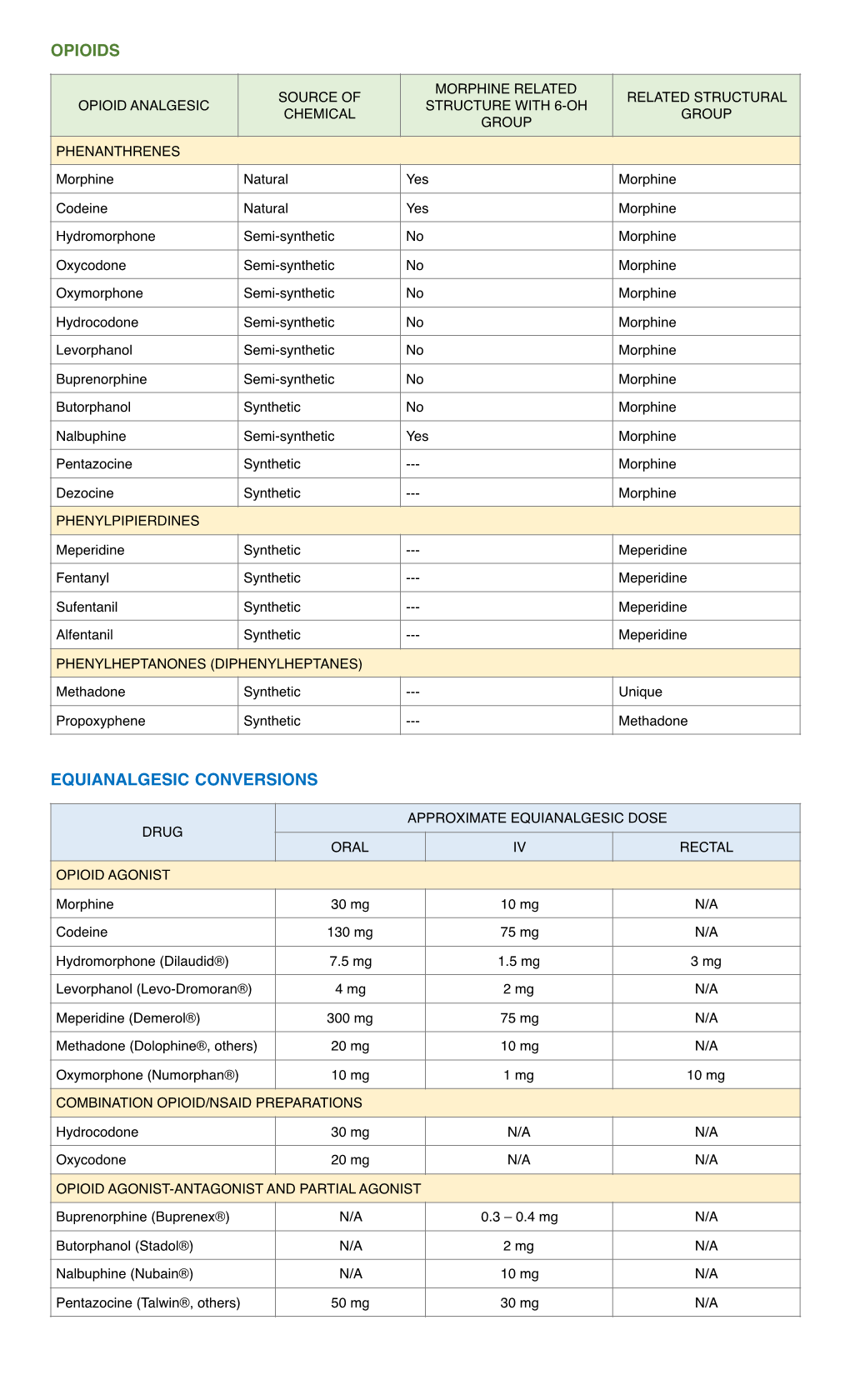
Opioid Conversion Chart
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dezocine Exhibits Antihypersensitivity Activities in Neuropathy Through
www.nature.com/scientificreports OPEN Dezocine exhibits antihypersensitivity activities in neuropathy through spinal Received: 09 November 2016 Accepted: 19 January 2017 μ-opioid receptor activation and Published: 23 February 2017 norepinephrine reuptake inhibition Yong-Xiang Wang1, Xiao-Fang Mao1, Teng-Fei Li1, Nian Gong1 & Ma-Zhong Zhang2 Dezocine is the number one opioid painkiller prescribed and sold in China, occupying 44% of the nation’s opioid analgesics market today and far ahead of the gold-standard morphine. We discovered the mechanisms underlying dezocine antihypersensitivity activity and assessed their implications to antihypersensitivity tolerance. Dezocine, given subcutaneously in spinal nerve-ligated neuropathic rats, time- and dose-dependently produced mechanical antiallodynia and thermal antihyperalgesia, significantly increased ipsilateral spinal norepinephrine and serotonin levels, and induced less antiallodynic tolerance than morphine. Its mechanical antiallodynia was partially (40% or 60%) and completely (100%) attenuated by spinal μ-opioid receptor (MOR) antagonism or norepinephrine depletion/α2-adrenoceptor antagonism and combined antagonism of MORs and α2-adenoceptors, respectively. In contrast, antagonism of spinal κ-opioid receptors (KORs) and δ-opioid receptors (DORs) or depletion of spinal serotonin did not significantly alter dezocine antiallodynia. In addition, dezocine- delayed antiallodynic tolerance was accelerated by spinal norepinephrine depletion/α2-adenoceptor antagonism. Thus dezocine produces antihypersensitivity activity through spinal MOR activation and norepinephrine reuptake inhibition (NRI), but apparently not through spinal KOR and DOR activation, serotonin reuptake inhibition or other mechanisms. Our findings reclassify dezocine as the first analgesic of the recently proposed MOR-NRI, and reveal its potential as an alternative to as well as concurrent use with morphine in treating pain. -

Supplemental Information
REVIEW ARTICLE Supplemental Information SEARCH STRATEGIES 7. exp Congenital Abnormalities/ or remifentanil or sufentanil or 8. (defect or cleft or heart defect tapentadol or tramadol or heroin Database: Ovid MEDLINE(R) In- or nalmefene or naloxone or Process and Other Nonindexed or gastroschisis or cryptorchidism or atresia or congenital or clubfoot naltrexone).mp. Citations and Ovid MEDLINE(R), or renal or craniosynostosis or 4. 1 or 2 or 3 1946 to Present hypospadias or malformation or 5. exp pregnancy/or exp pregnancy spina bifida or neural tube defect). outcome/ mp. 1. exp Analgesics, Opioid/ 6. exp teratogenic agent/ 9. 5 or 6 or 7 or 8 2. (opioid* or opiate*).mp. 7. exp congenital disorder/ 10. 4 and 9 3. (alfentanil or alphaprodine or 11. Limit 10 to (English language and 8. (defect or cleft or heart defect buprenorphine or butorphanol humans) or gastroschisis or cryptorchidism or codeine or dezocine or or atresia or congenital or clubfoot dihydrocodeine or fentanyl or Database: Ovid Embase, 1988– or renal or craniosynostosis or hydrocodone or hydromorphone 2016, Week 7 hypospadias or malformation or or levomethadyl or levorphanol spina bifida or neural tube defect). or meperidine or methadone or mp. 1. exp opiate/ morphine or nalbuphine or opium 9. 5 or 6 or 7 or 8 or oxycodone or oxymorphone 2. (opioid* or opiate*).mp. or pentazocine or propoxyphene 10. 4 and 9 3. (alfentanil or alphaprodine or or remifentanil or sufentanil or buprenorphine or butorphanol 11. Limit 10 to (human and English tapentadol or tramadol or heroin or codeine or dezocine or language and (article or book or or nalmefene or naloxone or book series or conference paper dihydrocodeine or fentanyl or “ ” naltrexone).mp. -

VHA/Dod CLINICAL PRACTICE GUIDELINE for the MANAGEMENT of POSTOPERATIVE PAIN
VHA/DoD CLINICAL PRACTICE GUIDELINE FOR THE MANAGEMENT OF POSTOPERATIVE PAIN Veterans Health Administration Department of Defense Prepared by: THE MANAGEMENT OF POSTOPERATIVE PAIN Working Group with support from: The Office of Performance and Quality, VHA, Washington, DC & Quality Management Directorate, United States Army MEDCOM VERSION 1.2 JULY 2001/ UPDATE MAY 2002 VHA/DOD CLINICAL PRACTICE GUIDELINE FOR THE MANAGEMENT OF POSTOPERATIVE PAIN TABLE OF CONTENTS Version 1.2 Version 1.2 VHA/DoD Clinical Practice Guideline for the Management of Postoperative Pain TABLE OF CONTENTS INTRODUCTION A. ALGORITHM & ANNOTATIONS • Preoperative Pain Management.....................................................................................................1 • Postoperative Pain Management ...................................................................................................2 B. PAIN ASSESSMENT C. SITE-SPECIFIC PAIN MANAGEMENT • Summary Table: Site-Specific Pain Management Interventions ................................................1 • Head and Neck Surgery..................................................................................................................3 - Ophthalmic Surgery - Craniotomies Surgery - Radical Neck Surgery - Oral-maxillofacial • Thorax (Non-cardiac) Surgery.......................................................................................................9 - Thoracotomy - Mastectomy - Thoracoscopy • Thorax (Cardiac) Surgery............................................................................................................16 -

Measures and CDS for Safer Opioid Prescribing: a Literature Review
Measures and CDS for Safer Opioid Prescribing: A Literature Review Measures and CDS for Safer Opioid Prescribing: A Literature Review Executive Summary The U.S. opioid epidemic continues to pose significant challenges for patients, families, clinicians, and public health policy. Opioids are responsible for an estimated 315,000 deaths (from 1999 to 2016) and have caused 115 deaths per day.1 In 2017, the U.S. Department of Health and Human Services declared the opioid epidemic a public health crisis.2 The total economic burden of opioid abuse in the United States has been estimated to be $78.5 billion per year.3 Although providing care for chronic opioid users is important, equally vital are efforts to prevent so-called opioid-naïve patients (patients with no history of opioid use) from developing regular opioid use, misuse, or abuse. However, much remains unclear regarding what role clinician prescribing habits play and what duration or dose of opioids may safely be prescribed without promoting long-term use.4,5 In 2013, ECRI Institute convened the Partnership for Health IT Patient Safety, and its component, single-topic-focused workgroups followed. For this subject, the Electronic Health Record Association (EHRA): Measures and Clinical Decision Support (CDS) for Safer Opioid Prescribing workgroup included members from the Healthcare Information and Management Systems Society (HIMSS) EHRA and the Partnership team. The project was oriented towards exploring methods to enable a synergistic cycle of performance measurement and identifying electronic health record (EHR)/health information technology (IT)–enabled approaches to support healthcare organizations’ ability to assess and measure opioid prescribing. -

Original Article Preoperative Intravenous Administration Of
Int J Clin Exp Med 2016;9(9):18451-18457 www.ijcem.com /ISSN:1940-5901/IJCEM0016462 Original Article Preoperative intravenous administration of dezocine for cesarean section under epidural anesthesia: effects on maternal well-being and neonatal outcome Keqiang He, Jianhui Pan, Liguo Hu, Ruiting Wang, Ling Hu Department of Anesthesia, Affiliated Provincial Hospital of Anhui Medical University, Hefei 230001, China Received September 19, 2015; Accepted January 21, 2016; Epub September 15, 2016; Published September 30, 2016 Abstract: We evaluated the efficacy and safety of preoperative intravenous administration of dezocine for comfort- able birth by cesarean section under epidural anesthesia. Sixty primigravida women with full-term singletons un- derwent elective cesarean section, and were randomly divided into three groups. Patients in groups A and B were intravenously injected with 5 and 10 mg of dezocine, 10 min before skin incision, whereas patients in group C were intravenously injected with saline. We recorded data on visceral traction responses and intraoperative adverse reactions, such as nausea and vomiting. While the neonate was being delivered, the umbilical arterial and venous blood gas values were determined. The Apgar scores at 1, 5, and 10 min after delivery, as well as the Neurologic Adaptive and Capacity Score (NACS) at 15 min, 2 h, and 24 h, were recorded. The “fineness rate” required to relieve the traction reaction in group B was higher than that in group C (P < 0.05). The intraoperative Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) scores of groups A and B were lower than that of group C, and the time period that the intraoperative MOAA/S score was ≤ 4 points was longer in group B (P < 0.05). -

Drug and Medication Classification Schedule
KENTUCKY HORSE RACING COMMISSION UNIFORM DRUG, MEDICATION, AND SUBSTANCE CLASSIFICATION SCHEDULE KHRC 8-020-1 (11/2018) Class A drugs, medications, and substances are those (1) that have the highest potential to influence performance in the equine athlete, regardless of their approval by the United States Food and Drug Administration, or (2) that lack approval by the United States Food and Drug Administration but have pharmacologic effects similar to certain Class B drugs, medications, or substances that are approved by the United States Food and Drug Administration. Acecarbromal Bolasterone Cimaterol Divalproex Fluanisone Acetophenazine Boldione Citalopram Dixyrazine Fludiazepam Adinazolam Brimondine Cllibucaine Donepezil Flunitrazepam Alcuronium Bromazepam Clobazam Dopamine Fluopromazine Alfentanil Bromfenac Clocapramine Doxacurium Fluoresone Almotriptan Bromisovalum Clomethiazole Doxapram Fluoxetine Alphaprodine Bromocriptine Clomipramine Doxazosin Flupenthixol Alpidem Bromperidol Clonazepam Doxefazepam Flupirtine Alprazolam Brotizolam Clorazepate Doxepin Flurazepam Alprenolol Bufexamac Clormecaine Droperidol Fluspirilene Althesin Bupivacaine Clostebol Duloxetine Flutoprazepam Aminorex Buprenorphine Clothiapine Eletriptan Fluvoxamine Amisulpride Buspirone Clotiazepam Enalapril Formebolone Amitriptyline Bupropion Cloxazolam Enciprazine Fosinopril Amobarbital Butabartital Clozapine Endorphins Furzabol Amoxapine Butacaine Cobratoxin Enkephalins Galantamine Amperozide Butalbital Cocaine Ephedrine Gallamine Amphetamine Butanilicaine Codeine -

Effect of Dezocine on the Ratio of Th1/Th2 Cytokines in Patients
Drug Design, Development and Therapy Dovepress open access to scientific and medical research Open Access Full Text Article ORIGINAL RESEARCH Effect of Dezocine on the Ratio of Th1/Th2 Cytokines in Patients Receiving Postoperative Analgesia Following Laparoscopic Radical Gastrectomy: A Prospective Randomised Study Man Feng1 Purpose: To evaluate the effect of dezocine on the postoperative ratio of Th1/Th2 cytokines Qinli Feng2 in patients undergoing laparoscopic radical gastrectomy. Yujie Chen3 Patients and Methods: Sixty patients undergoing laparoscopic radical gastrectomy were Ge Liu 2 randomly divided into two groups (n=30): dezocine group (Group D) and sufentanil group Zhuanglei Gao4 (Group S). They received patient-controlled intravenous analgesia (PCIA) after the operation with either dezocine 0.8 mg/kg (Group D) or sufentanil 2 µg/kg (Group S). Both groups also Juan Xiao5 received ondansetron 8 mg diluted to 100 mL with saline. The primary outcome was the Th1/ Chang Feng 2 Th2 cytokines ratio at predetermined intervals, 30 min before the induction of general 1Department of Pathology, Affiliated anaesthesia and 0, 12, 24 and 48 h after surgery. The secondary endpoints were patients’ Hospital of Shandong Academy of pain scores, measured on a visual analogue scale (VAS) at predetermined intervals (0, 12, 24 Medical Sciences, Shandong First Medical University, Jinan, 250000, People’s and 48 h after surgery), and side effects at follow-up 48 h after surgery. 2 Republic of China; Department of Results: The Th1/Th2 cytokines ratio in Group D was significantly higher than Group Anesthesiology, The Second Hospital, Cheeloo College of Medicine, Shandong S (P<0.05) 12, 24 and 48 h after the operation. -

Levorphanol Use: Past, Present and Future
Postgraduate Medicine ISSN: 0032-5481 (Print) 1941-9260 (Online) Journal homepage: http://www.tandfonline.com/loi/ipgm20 Levorphanol Use: Past, Present and Future Jeffrey Gudin, Jeffrey Fudin & Srinivas Nalamachu To cite this article: Jeffrey Gudin, Jeffrey Fudin & Srinivas Nalamachu (2015): Levorphanol Use: Past, Present and Future, Postgraduate Medicine, DOI: 10.1080/00325481.2016.1128308 To link to this article: http://dx.doi.org/10.1080/00325481.2016.1128308 Accepted author version posted online: 03 Dec 2015. Submit your article to this journal View related articles View Crossmark data Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ipgm20 Download by: [Jeffrey Fudin] Date: 03 December 2015, At: 20:32 Publisher: Taylor & Francis Journal: Postgraduate Medicine DOI: 10.1080/00325481.2016.1128308 Levorphanol Use: Past, Present and Future Authors: Jeffrey Gudin1, Jeffrey Fudin2, and Srinivas Nalamachu3 Affiliations: 1Director, Pain Management and Palliative Care, Englewood Hospital and Medical Center, Englewood, NJ, and Clinical Instructor, Anesthesiology, Icahn School of Medicine at Mount Sinai, New York, NY. 2Adjunct Associate Professor, Albany College of Pharmacy and Health Sciences and also Western New England University College of Pharmacy Director, PGY2 Pain Residency and Clinical Pharmacy, Specialist, Pain Management Stratton VA Medical Center, Albany, NY 3President and Medical Director, International Clinical Research Institute, Overland Park, KS, and Adjunct Associate Professor, Temple University School of Medicine, Downloaded by [Jeffrey Fudin] at 20:32 03 December 2015 Philadelphia, PA. Running Title: Levorphanol Use: Past, Present and Future Corresponding Author Srinivas Nalamachu Srinivas R. Nalamachu MD International Clinical Research Institute, Inc. -

Darvon® (Propoxyphene Hydrochloride Capsules, Usp) Pulvules®
DARVON® (PROPOXYPHENE HYDROCHLORIDE CAPSULES, USP) PULVULES® CIV Rx only WARNINGS • There have been numerous cases of accidental and intentional overdose with propoxyphene products either alone or in combination with other CNS depressants, including alcohol. Fatalities within the first hour of overdosage are not uncommon. Many of the propoxyphene-related deaths have occurred in patients with previous histories of emotional disturbances or suicidal ideation/attempts and/or concomitant administration of sedatives, tranquilizers, muscle relaxants, antidepressants, or other CNS-depressant drugs. Do not prescribe propoxyphene for patients who are suicidal or have a history of suicidal ideation. • The metabolism of propoxyphene may be altered by strong CYP3A4 inhibitors (such as ritonavir, ketoconazole, itraconazole, troleandomycin, clarithromycin, nelfinavir, nefazadone, amiodarone, amprenavir, aprepitant, diltiazem, erythromycin, fluconazole, fosamprenavir, grapefruit juice, and verapamil) leading to enhanced propoxyphene plasma levels. Patients receiving propoxyphene and any CYP3A4 inhibitor should be carefully monitored for an extended period of time and dosage adjustments should be made if warranted (see CLINICAL PHARMACOLOGY – Drug Interactions and WARNINGS, PRECAUTIONS and DOSAGE AND ADMINISTRATION for further information). DESCRIPTION Darvon contains propoxyphene hydrochloride, USP which is an odorless, white crystalline powder with a bitter taste. It is freely soluble in water. Chemically, it is (2S,3R)-(+)-4-(Dimethylamino)-3-methyl-1,2-diphenyl-2-butanol propionate (ester) hydrochloride, which can be represented by the accompanying structural formula. Its molecular weight is 375.94. Each pulvule contains 65 mg (172.9 μmol) propoxyphene hydrochloride. It also contains D & C Red No. 33, F D & C Yellow No. 6, gelatin, magnesium stearate, silicone, starch, titanium dioxide, and other inactive ingredients. -

Use of Chronic Opioid Therapy in Chronic Noncancer Pain CHRONIC NONCANCER PAINNONCANCER CHRONIC Evidence Review
CLINICAL GUIDELINE FOR THE USE OF CHRONIC OPIOID THERAPY IN CLINICAL GUIDELINE FOR THE USE OF CHRONIC OPIOID THERAPY IN GUIDELINE FOR THE Use of Chronic Opioid Therapy in Chronic Noncancer Pain CHRONIC NONCANCER PAIN Evidence Review The American Pain Society in Conjunction with The American Academy of Pain Medicine EVIDENCE REVIEW APS-AAPM Clinical Guidelines for the Use of Chronic Opioid Therapy in Chronic Noncancer Pain TABLE OF CONTENTS Page Introduction 1 Purpose of evidence review ...................................................................... 1 Background 1 Previous guidelines ................................................................................... 2 Scope of evidence review 3 Key questions............................................................................................ 3 Populations................................................................................................ 7 Interventions.............................................................................................. 8 Outcomes.................................................................................................. 8 Conflict of interest............................................................................................. 10 Methods 10 Literature search and strategy................................................................... 10 Inclusion and exclusion criteria.................................................................. 11 Data extraction and synthesis .................................................................. -
Pharmacological Characterization of Dezocine, a Potent Analgesic Acting As a Κ Partial Agonist and Μ Partial Agonist
www.nature.com/scientificreports OPEN Pharmacological Characterization of Dezocine, a Potent Analgesic Acting as a κ Partial Agonist and μ Received: 6 November 2017 Accepted: 31 August 2018 Partial Agonist Published: xx xx xxxx Yu-Hua Wang1, Jing-Rui Chai2, Xue-Jun Xu2, Ru-Feng Ye2, Gui-Ying Zan2, George Yun-Kun Liu3, Jian-Dong Long2, Yan Ma4, Xiang Huang2, Zhi-Chao Xiao2, Hu Dong2 & Yu-Jun Wang2 Dezocine is becoming dominated in China market for relieving moderate to severe pain. It is believed that Dezocine’s clinical efcacy and little chance to provoke adverse events during the therapeutic process are mainly attributed to its partial agonist activity at the μ opioid receptor. In the present work, we comprehensively studied the pharmacological characterization of Dezocine and identifed that the analgesic efect of Dezocine was a result of action at both the κ and μ opioid receptors. We frstly found that Dezocine displayed preferential binding to μ opioid receptor over κ and δ opioid receptors. Dezocine, on its own, weakly stimulated G protein activation in cells expressing κ and μ receptors, but in the presence of full κ agonist U50,488 H and μ agonist DAMGO, Dezocine inhibited U50,488H- and DAMGO-mediated G protein activation, indicating that Dezocine was a κ partial agonist and μ partial agonist. Then the in intro results were verifed by in vivo studies in mice. We observed that Dezocine- produced antinociception was signifcantly inhibited by κ antagonist nor-BNI and μ antagonist β-FNA pretreatment, indicating that Dezocine-mediated antinociception was via both the κ and μ opioid receptors. -

Interactions Between Opioid Agonists and Glutamate Receptor Antagonists (Under the Direction of Linda A
INTERACTIONS BETWEEN OPIOID AGONISTS AND GLUTAMATE RECEPTOR ANTAGONISTS Bradford D. Fischer A dissertation submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Psychology (Behavioral Neuroscience). Chapel Hill 2008 Approved by: Linda A. Dykstra, Ph.D. Clyde W. Hodge, Ph.D. Mark Hollins, Ph.D. Donald T. Lysle, Ph.D. Mitchell J. Picker, Ph.D. © 2008 Bradford D. Fischer ALL RIGHTS RESERVED ii ABSTRACT BRADFORD D. FISCHER: Interactions between Opioid Agonists and Glutamate Receptor Antagonists (Under the direction of Linda A. Dykstra) The following studies systematically examine the interactive effects of opioids and glutamate receptor antagonists in assays of schedule-controlled responding and thermal nociception. Experiment 1 examines the effects of morphine, buprenorphine, butorphanol, and nalbuphine alone and in combination with an N-Methyl-D-Aspartate (NMDA) receptor antagonist on schedule-controlled responding and thermal nociception. The results from this study indicate that NMDA antagonist/morphine and NMDA antagonist/buprenorphine mixtures produce additive or infra-additive effects on schedule-controlled responding, whereas NMDA antagonist/butorphanol and NMDA antagonist/nalbuphine mixtures produced additive or supra-additive effects. In addition, mixtures of an NMDA antagonist in combination with morphine, buprenorphine, butorphanol, and nalbuphine produce additive or supra-additive effects on thermal nociception. Experiment 2 examines the interactive effects of morphine in combination with metabotropic glutamate (mGlu) receptor antagonists selective for mGlu1, mGlu5, and mGlu2/3 receptor subtypes on schedule-controlled responding and thermal nociception. The results from this experiment suggest that mGlu1, mGlu5, and mGlu2/3 antagonists produce additive effects when administered in combination with morphine on schedule-controlled iii responding.