Eczemas Due to Mites and Microorganisms
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gianotti-Crosti Syndrome
GIANOTTI-CROSTI SYNDROME http://www.aocd.org Gianotti-Crosti Syndrome (GCS) is also known as ‘papular acrodermatitis of childhood’ and ‘papulovesicular acrolated syndrome’. GCS is a viral eruption that typically begins on the buttocks and spreads to other areas of the body. The rash also affects the face and the extremities. The chest, back, belly, palms and soles are usually spared. In the United States, it is most commonly caused by Epstein-Barr virus infection. Hepatitis B is a common cause in parts of the world where the vaccination is not given. Other viruses that cause the rash include hepatitis A and C, cytomegalovirus, enterovirus, coxsackievirus, rotavirus, adenovirus, human herpes virus-6, respiratory syncytial virus, parvovirus B10, rubella, HIV, and parainfluenza. It has also been associated with viral immunizations for poliovirus, hepatitis A, diphtheria, small pox, pertussis and influenza. GCS most commonly occurs in children between the ages of one to three but can occur at any time from the ages of three months to fifteen years. The condition manifests more commonly in the spring and summer and lasts for four weeks but can last up to eight weeks. The rash has been known to occur more commonly in children with atopic dermatitis. The lesions present as single, red to pink to brown colored bumps that may be fluid-filled. The size of the lesions can range from one to ten millimeters and present symmetrically. The bumps can come together and form larger lesions. Sometimes the child may present with a fever, enlarged tender lymph nodes and an enlarged spleen or liver. -

Urticaria from Wikipedia, the Free Encyclopedia Jump To: Navigation, Search "Hives" Redirects Here
Urticaria From Wikipedia, the free encyclopedia Jump to: navigation, search "Hives" redirects here. For other uses, see Hive. Urticaria Classification and external resourcesICD-10L50.ICD- 9708DiseasesDB13606MedlinePlus000845eMedicineemerg/628 MeSHD014581Urtic aria (or hives) is a skin condition, commonly caused by an allergic reaction, that is characterized by raised red skin wheals (welts). It is also known as nettle rash or uredo. Wheals from urticaria can appear anywhere on the body, including the face, lips, tongue, throat, and ears. The wheals may vary in size from about 5 mm (0.2 inches) in diameter to the size of a dinner plate; they typically itch severely, sting, or burn, and often have a pale border. Urticaria is generally caused by direct contact with an allergenic substance, or an immune response to food or some other allergen, but can also appear for other reasons, notably emotional stress. The rash can be triggered by quite innocent events, such as mere rubbing or exposure to cold. Contents [hide] * 1 Pathophysiology * 2 Differential diagnosis * 3 Types * 4 Related conditions * 5 Treatment and management o 5.1 Histamine antagonists o 5.2 Other o 5.3 Dietary * 6 See also * 7 References * 8 External links [edit] Pathophysiology Allergic urticaria on the shin induced by an antibiotic The skin lesions of urticarial disease are caused by an inflammatory reaction in the skin, causing leakage of capillaries in the dermis, and resulting in an edema which persists until the interstitial fluid is absorbed into the surrounding cells. Urticarial disease is thought to be caused by the release of histamine and other mediators of inflammation (cytokines) from cells in the skin. -

Dyshidrotic Eczema
University of Calgary PRISM: University of Calgary's Digital Repository Cumming School of Medicine Cumming School of Medicine Research & Publications 2014-09-16 Dyshidrotic eczema Leung, Alexander K.C.; Barankin, Benjamin; Hon, Kam Lun Enliven Archive Leung AK, Barankin B, Hon KL (2014) Dyshidrotic Eczema. Enliven: Pediatr Neonatol Biol 1(1): 002. http://hdl.handle.net/1880/50267 journal article Downloaded from PRISM: https://prism.ucalgary.ca Research Article www.enlivenarchive.org Enliven: Pediatrics and Neonatal Biology Dyshidrotic Eczema Alexander K. C. Leung1*, Benjamin Barankin2, and Kam Lun Hon3 1Clinical Professor of Pediatrics, University of Calgary, Pediatric Consultant, Alberta Children’s Hospital 2Medical Director and Founder, Toronto Dermatology Centre 3Professor of Pediatrics, Chinese University of Hong Kong * Corresponding author: Alexander K. C. Leung, MBBS, FRCPC, FRCP Citation: Leung AK, Barankin B, Hon KL (2014) Dyshidrotic Eczema. (UK & Irel), FRCPCH, FAAP, Clinical Professor of Pediatrics, University Enliven: Pediatr Neonatol Biol 1(1): 002. of Calgary, Pediatric Consultant, Alberta Children’s Hospital, Canada, Tel: Copyright:@ 2014 Dr. Alexander K. C. Leung. This is an Open Access (403) 230-3322; Fax: (403) 230-3322; E-mail: [email protected] article published and distributed under the terms of the Creative Commons th Received Date: 14 August 2014 Attribution License, which permits unrestricted use, distribution and th Accepted Date: 10 September 2014 reproduction in any medium, provided the original author and source are th Published Date: 16 September 2014 credited. Abstract Dyshidrotic eczema, also known as dyshidrotic dermatitis or pompholyx, is characterized by pruritic, tense, deep-seated vesicles mainly on the palms and lateral surfaces of the fingers. -

Tinea Capitis 2014 L.C
BJD GUIDELINES British Journal of Dermatology British Association of Dermatologists’ guidelines for the management of tinea capitis 2014 L.C. Fuller,1 R.C. Barton,2 M.F. Mohd Mustapa,3 L.E. Proudfoot,4 S.P. Punjabi5 and E.M. Higgins6 1Department of Dermatology, Chelsea & Westminster Hospital, Fulham Road, London SW10 9NH, U.K. 2Department of Microbiology, Leeds General Infirmary, Leeds LS1 3EX, U.K. 3British Association of Dermatologists, Willan House, 4 Fitzroy Square, London W1T 5HQ, U.K. 4St John’s Institute of Dermatology, Guy’s and St Thomas’ NHS Foundation Trust, St Thomas’ Hospital, Westminster Bridge Road, London SE1 7EH, U.K. 5Department of Dermatology, Hammersmith Hospital, 150 Du Cane Road, London W12 0HS, U.K. 6Department of Dermatology, King’s College Hospital, Denmark Hill, London SE5 9RS, U.K. 1.0 Purpose and scope Correspondence Claire Fuller. The overall objective of this guideline is to provide up-to- E-mail: [email protected] date, evidence-based recommendations for the management of tinea capitis. This document aims to update and expand Accepted for publication on the previous guidelines by (i) offering an appraisal of 8 June 2014 all relevant literature since January 1999, focusing on any key developments; (ii) addressing important, practical clini- Funding sources cal questions relating to the primary guideline objective, i.e. None. accurate diagnosis and identification of cases; suitable treat- ment to minimize duration of disease, discomfort and scar- Conflicts of interest ring; and limiting spread among other members of the L.C.F. has received sponsorship to attend conferences from Almirall, Janssen and LEO Pharma (nonspecific); has acted as a consultant for Alliance Pharma (nonspe- community; (iii) providing guideline recommendations and, cific); and has legal representation for L’Oreal U.K. -

Guías Diagnósticas Y Terapeúticas De Las 10 Patologías Más Frecuentes
HOSPITAL INFANTIL DE MÉXICO “FEDERICO GÓMEZ” SERVICIO DE DERMATOLOGÍA GUÍAS DIAGNÓSTICAS Y TERAPÉUTICAS DE LAS 10 PATOLOGÍAS MÁS FRECUENTES DR CARLOS ALFREDO MENA CEDILLOS, JEFE DEL SERVICIO DRA ADRIANA MARÍA VALENCIA HERRERA DERMATITIS ATOPICA SINONIMIA. Neurodermatitis, prurigo de Besnier, eccema del lactante. DEFINICION. Enfermedad reaccional, crónica y recidivante de la piel, con un patrón clínico e historia natural característicos. No se conoce la causa específica, pero se ha relacionado con susceptibilidad genética, disturbios inmuológicos y constitucionales, sobre los que actúan factores desencadenantes. EPIDEMIOLOGIA: Es la dermatosis más frecuente en población pediátrica. La prevalencia ha mostrando incremento en las últimas décadas, siendo del 18-20%. Es mas frecuente en áreas urbanas de países industrializados, especialmente en inmigrantes provenientes de países con menor prevalencia. No existe clara predilección racial ni diferencia en cuanto al sexo. Puede presentarse a cualquier edad, con claro predominio en la población pediátrica, 60-85% de los casos inicia en el primer año de vida y 85-95% antes de los 5 años; 10-25% de los casos persiste con recaídas en la edad adulta. ETIOPATOGENIA. La etiología es desconocida pero parece ser resultado de una compleja interacción aspectos genéticos, inmunológicos y defectos en la barrera epidérmica, existiendo múltiples factores descencadenantes, queactúan sobre un terreno constitucionalmente alterado. 1. Anomalías genéticas. Tiene clara naturaleza familiar, pero no se ha precisado el mecanismo de herencia, existiendo en 70% de los pacientes antecedentes de atopia. Los antígenos de histocompatibilidad HL-A9, HL-A3, HL-B12 y HL-Bw40 se han descrito en estos pacientes. 2. Disturbios inmunológicos. Existen cambios significativos en la inmunidad humoral y celular. -

My Approach to Superficial Inflammatory Dermatoses K O Alsaad, D Ghazarian
1233 J Clin Pathol: first published as 10.1136/jcp.2005.027151 on 25 November 2005. Downloaded from REVIEW My approach to superficial inflammatory dermatoses K O Alsaad, D Ghazarian ............................................................................................................................... J Clin Pathol 2005;58:1233–1241. doi: 10.1136/jcp.2005.027151 Superficial inflammatory dermatoses are very common and diagnosis of inflammatory skin diseases, there are limitations to this approach. The size of the comprise a wide, complex variety of clinical conditions. skin biopsy should be adequate and representa- Accurate histological diagnosis, although it can sometimes tive of all four compartments and should also be difficult to establish, is essential for clinical include hair follicles. A 2 mm punch biopsy is too small to represent all compartments, and often management. Knowledge of the microanatomy of the skin insufficient to demonstrate a recognisable pat- is important to recognise the variable histological patterns tern. A 4 mm punch biopsy is preferred, and of inflammatory skin diseases. This article reviews the non- usually adequate for the histological evaluation of most inflammatory dermatoses. However, a vesiculobullous/pustular inflammatory superficial larger biopsy (6 mm punch biopsy), or even an dermatoses based on the compartmental microanatomy of incisional biopsy, might be necessary in panni- the skin. culitis or cutaneous lymphoproliferative disor- ders. A superficial or shave biopsy should be .......................................................................... -

Dermatological Indications of Disease - Part II This Patient on Dialysis Is Showing: A
“Cutaneous Manifestations of Disease” ACOI - Las Vegas FR Darrow, DO, MACOI Burrell College of Osteopathic Medicine This 56 year old man has a history of headaches, jaw claudication and recent onset of blindness in his left eye. Sed rate is 110. He has: A. Ergot poisoning. B. Cholesterol emboli. C. Temporal arteritis. D. Scleroderma. E. Mucormycosis. Varicella associated. GCA complex = Cranial arteritis; Aortic arch syndrome; Fever/wasting syndrome (FUO); Polymyalgia rheumatica. This patient missed his vaccine due at age: A. 45 B. 50 C. 55 D. 60 E. 65 He must see a (an): A. neurologist. B. opthalmologist. C. cardiologist. D. gastroenterologist. E. surgeon. Medscape This 60 y/o male patient would most likely have which of the following as a pathogen? A. Pseudomonas B. Group B streptococcus* C. Listeria D. Pneumococcus E. Staphylococcus epidermidis This skin condition, erysipelas, may rarely lead to septicemia, thrombophlebitis, septic arthritis, osteomyelitis, and endocarditis. Involves the lymphatics with scarring and chronic lymphedema. *more likely pyogenes/beta hemolytic Streptococcus This patient is susceptible to: A. psoriasis. B. rheumatic fever. C. vasculitis. D. Celiac disease E. membranoproliferative glomerulonephritis. Also susceptible to PSGN and scarlet fever and reactive arthritis. Culture if MRSA suspected. This patient has antithyroid antibodies. This is: • A. alopecia areata. • B. psoriasis. • C. tinea. • D. lichen planus. • E. syphilis. Search for Hashimoto’s or Addison’s or other B8, Q2, Q3, DRB1, DR3, DR4, DR8 diseases. This patient who works in the electronics industry presents with paresthesias, abdominal pain, fingernail changes, and the below findings. He may well have poisoning from : A. lead. B. -

Differential Diagnosis in Dermatology
Differential Diagnosis in Dermatology ZohrehTehranchi Dermatologist COMMON ACNE AND CYSTIC ACNE Rosacea Rosacea PERIORAL DERMATITIS ECZEMA/DERMATITIS Chronic irritant dermatitis Dyshidrotic eczematous dermatitis Childood atopic dermatitis Autosensitization dermatitis (“id” reaction): dermatophytid Seborrheic dermatitis PSORIASIS VULGARIS Pemphigus vulgaris BULLOUS PEMPHIGOID (BP) Pityriasis rosea small-plaque parapsoriasis Large-plaque parapsoriasis (parapsoriasis en plaques) LICHEN PLANUS (LP) GRANULOMA ANNULARE (GA) Erythema multiforme ERYTHEMA NODOSUM Actinic keratoses Bowen disease (Squamous cell carcinoma in situ) Bowen disease and invasive SCC Squamous cell carcinoma: invasive on the lip Squamous cell carcinoma, well differentiated Squamous cell carcinoma, undifferentiated Squamous cell carcinoma, advanced, well differentiated, on the hand Keratoacanthoma showing different stages of evolution BASAL CELL CARCINOMA (BCC) Basal cell carcinoma, ulcerated: Rodent ulcer A large rodent ulcer in the nuchal and Bas cell calarcinoma: sclerosing type retroauricular area extending to the temple Basal cell carcinoma, sclerosing, nodular, Superficial basal cell carcinoma: solitary lesion and multiple lesions Superficial basal cell carcinoma, invasive Basal cell carcinoma, pigmented Dysplastic nevi Superficial spreading melanoma: arising within a dysplastic nevus Congenital nevomelanocytic nevus Melanoma: arising in small CNMN Melanoma in situ: lentigo maligna Melanoma in situ, superficial spreading type Superficial spreading melanoma, vertical -

Potential Approaches Towards Dermatitis
l of Derm na a r t u it i o s J ISSN: 2684-1436 Journal of Dermatitis Editorial Note Potential Approaches towards Dermatitis Nabanita Mukherjee* Department of Dermatology, University of Colorado, Anschutz Medical Campus, USA EDITORIAL NOTE An article titled “The Impact of Microanatomy and Changing Dermatitis, well known as eczema, is defined as a group of Physiology of Stratum Corneum, the Skin Barrier, on Evolution diseases causing skin inflammation. They are caused due to of Atopic Dermatitis”, written by Dr.Virendra N Sehgal which adverse drug reactions. It is generally characterized by rashes, discusses the effect of changing of pattern and characteristics of redness of skin, itchiness or growth of small blisters. Long term stratum corneum taking salient featuring stock of microanatomy causation of this disease may cause thickening of the skin and and physiology[1]. The article is about degradation of certain can vary to spread from small area of skin to the entire body. It proteins due to the up-regulation of serine protease activity, includes mainly allergic contact dermatitis, atopic dermatitis, filaggrin being the predisposing factor in the pathogenesis of irritant contact dermatitis and stasis dermatitis. It belongs to the AD, its treatments and preventive measures. branch of Dermatological immunology. It is not a life Other article titled “A Randomized Trial to Evaluate the Efficacy threatening and contagious disease. and Saftey of 1% Pimecrolimus Cream vs. 0.05% Clobetasol The Journal of Dermatitis is a peer-reviewed, open access Propionate Cream for the Treatment of Childhood Vitiligo”[2], scientific journal dealing with articles on various arenas of written by Dr, Preeti Sharma, et all. -
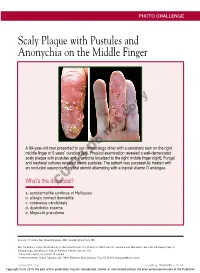
Scaly Plaque with Pustules and Anonychia on the Middle Finger
PHOTO CHALLENGE Scaly Plaque with Pustules and Anonychia on the Middle Finger copy not A 69-year-old man presented to our dermatology clinic with a persistent rash on the right middle finger of 5 years’ duration (left). PhysicalDo examination revealed a well-demarcated scaly plaque with pustules and anonychia localized to the right middle finger (right). Fungal and bacterial cultures revealed sterile pustules. The patient was successfully treated with an occluded superpotent topical steroid alternating with a topical vitamin D analogue. What’s the diagnosis?CUTIS a. acrodermatitis continua of Hallopeau b. allergic contact dermatitis c. cutaneous candidiasis d. dyshidrotic eczema e. Majocchi granuloma Joan A. Chandra, BA; Anand Rajpara, MD; Joseph Blackmon, MD Ms. Chandra is from the University of Missouri-Kansas City School of Medicine. Drs. Rajpara and Blackmon are from the Department of Dermatology, University of Kansas Medical Center, Kansas City. The authors report no conflict of interest. Correspondence: Anand Rajpara, MD, 3901 Rainbow Blvd, Kansas City, KS 66160 ([email protected]). WWW.CUTIS.COM VOLUME 96, DECEMBER 2015 E1 Copyright Cutis 2015. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. Photo Challenge Discussion The Diagnosis: Acrodermatitis Continua of Hallopeau crodermatitis continua of Hallopeau (ACH) Dermatology in General Medicine. 7th ed. New York, NY: is considered to be a form of acropustular McGraw-Hill; 2007:215-218. Apsoriasis that presents as a sterile, pustular 4. Yerushalmi J, Grunwald MH, Hallel-Halevy D, et al. eruption initially affecting the fingertips and/or Chronic pustular eruption of the thumbs. -

Peri-Orificial Rash in an Infant
BMJ 2017;358:j3606 doi: 10.1136/bmj.j3606 (Published 2017 September 07) Page 1 of 4 Endgames ENDGAMES CASE REVIEW Peri-orificial rash in an infant Hui Min Liew consultant, Jin Ho Chong consultant Dermatology, KK Women’s and Children’s Hospital, Singapore A 6 month old girl was brought to the paediatric dermatology outpatient clinic with a rash, irritability, and poor weight gain Answers for two months. She was born at 32 weeks’ gestation with intrauterine growth restriction as a result of placental 1. insufficiency. She was exclusively breastfed. There was no What are the differential diagnoses? family history of skin disorders. On examination, she had scaly Short answer erythematous plaques around her eyes, nose, mouth, ears, and Differential diagnoses include atopic dermatitis, psoriasis, neck (fig 1). impetigo, tinea infection, peri-orificial dermatitis, zinc deficiency, and, more rarely, Langerhans cell histiocytosis, other nutritional deficiencies, and metabolic disorders. Discussion The differentiating features of the aforementioned conditions1 are described in Table 1⇓. 2. Which differential diagnosis is most likely? Short answer The likely diagnosis is acquired zinc deficiency as a result of Fig 1 Scaly erythematous plaques around the eyes, nostril, poor nutrition in the breastfeeding mother and the increased mouth, ears, and neck demand for zinc in the premature baby. In an infant, symptoms of zinc deficiency include faltering weight, irritability, and peri-orificial dermatitis. She had been recently prescribed mild topical corticosteroids to treat presumed atopic dermatitis, but there had been no improvement. Discussion Skin swab and scraping for bacterial and fungal microscopy The serum zinc level in the child’s mother was low at 665 μg/L 2 and culture were taken. -

Dermatology Grand Rounds 2019 Skin Signs of Internal Disease
Dermatology Grand Rounds 2019 skin signs of internal disease John Strasswimmer, MD, PhD Affiliate Clinical Professor (Dermatology), FAU College of Medicine Research Professor of Biochemistry, FAU College of Science Associate Clinical Professor, U. Miami Miller School of Medicine Dermatologist and Internal Medicine “Normal” abnormal skin findings in internal disease • Thyroid • Renal insufficiency • Diabetes “Abnormal” skin findings as clue to internal disease • Markers of infectious disease • Markers of internal malignancy risk “Consultation Cases” • Very large dermatology finding • A very tiny dermatology finding Dermatologist and Internal Medicine The "Red and Scaly” patient “Big and Small” red rashes not to miss The "Red and Scaly” patient • 29 Year old man with two year pruritic eruption • PMHx: • seasonal allergies • childhood eczema • no medications Erythroderma Erythroderma • Also called “exfoliative dermatitis” • Not stevens-Johnson / toxic epidermal necrosis ( More sudden onset, associated with target lesions, mucosal) • Generalized erythema and scale >80-90% of body surface • May be associated with telogen effluvium It is not a diagnosis per se Erythroderma Erythroderma Work up 1) Exam for pertinent positives and negatives: • lymphadenopathy • primary skin lesions (i.e. nail pits of psoriasis) • mucosal involvement • Hepatosplenomagaly 2) laboratory • Chem 7, LFT, CBC • HIV • Multiple biopsies over time 3) review of medications 4) age-appropriate malignancy screening 5) evaluate hemodynamic stability Erythroderma Management 1)