New Construction Homeownership Program This Program Is An
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Talking Stone: Cherokee Syllabary Inscriptions in Dark Zone Caves
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Masters Theses Graduate School 12-2017 Talking Stone: Cherokee Syllabary Inscriptions in Dark Zone Caves Beau Duke Carroll University of Tennessee, [email protected] Follow this and additional works at: https://trace.tennessee.edu/utk_gradthes Recommended Citation Carroll, Beau Duke, "Talking Stone: Cherokee Syllabary Inscriptions in Dark Zone Caves. " Master's Thesis, University of Tennessee, 2017. https://trace.tennessee.edu/utk_gradthes/4985 This Thesis is brought to you for free and open access by the Graduate School at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Masters Theses by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. To the Graduate Council: I am submitting herewith a thesis written by Beau Duke Carroll entitled "Talking Stone: Cherokee Syllabary Inscriptions in Dark Zone Caves." I have examined the final electronic copy of this thesis for form and content and recommend that it be accepted in partial fulfillment of the requirements for the degree of Master of Arts, with a major in Anthropology. Jan Simek, Major Professor We have read this thesis and recommend its acceptance: David G. Anderson, Julie L. Reed Accepted for the Council: Dixie L. Thompson Vice Provost and Dean of the Graduate School (Original signatures are on file with official studentecor r ds.) Talking Stone: Cherokee Syllabary Inscriptions in Dark Zone Caves A Thesis Presented for the Master of Arts Degree The University of Tennessee, Knoxville Beau Duke Carroll December 2017 Copyright © 2017 by Beau Duke Carroll All rights reserved ii ACKNOWLEDGMENTS This thesis would not be possible without the following people who contributed their time and expertise. -

Dangerously Free: Outlaws and Nation-Making in Literature of the Indian Territory
DANGEROUSLY FREE: OUTLAWS AND NATION-MAKING IN LITERATURE OF THE INDIAN TERRITORY by Jenna Hunnef A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Graduate Department of English University of Toronto © Copyright by Jenna Hunnef 2016 Dangerously Free: Outlaws and Nation-Making in Literature of the Indian Territory Jenna Hunnef Doctor of Philosophy Department of English University of Toronto 2016 Abstract In this dissertation, I examine how literary representations of outlaws and outlawry have contributed to the shaping of national identity in the United States. I analyze a series of texts set in the former Indian Territory (now part of the state of Oklahoma) for traces of what I call “outlaw rhetorics,” that is, the political expression in literature of marginalized realities and competing visions of nationhood. Outlaw rhetorics elicit new ways to think the nation differently—to imagine the nation otherwise; as such, I demonstrate that outlaw narratives are as capable of challenging the nation’s claims to territorial or imaginative title as they are of asserting them. Borrowing from Abenaki scholar Lisa Brooks’s definition of “nation” as “the multifaceted, lived experience of families who gather in particular places,” this dissertation draws an analogous relationship between outlaws and domestic spaces wherein they are both considered simultaneously exempt from and constitutive of civic life. In the same way that the outlaw’s alternately celebrated and marginal status endows him or her with the power to support and eschew the stories a nation tells about itself, so the liminality and centrality of domestic life have proven effective as a means of consolidating and dissenting from the status quo of the nation-state. -

Redbird Sixkiller Was Born on July 1, 1807 in Cherokee Nation East, Near Lookout Mountain, Georgia
Redbird A06 Sixkiller 1868 Washington, DC Redbird Sixkiller was born on July 1, 1807 in Cherokee Nation East, near Lookout Mountain, Georgia. As a youth he attended elementary and secondary school in that area, and later he received a scholarship from the Guess Family, a Quaker family, and attended school in New Ark, Delaware, where he studied law and phi- losophy. About 1836, just prior to the Cherokee Removal, Redbird married Pamelia Whaley. She was also born in the Cherokee Nation East. In 1837 Red- bird and Pamelia were informed that they would be forcibly removed from Georgia and would be relocated to Indian Territory, west of the Missis- sippi River. The Indian Removal has become known as The Trail of Tears. Redbird and Pamelia arrived in the Goingsnake District of Indian Territory in the Spring of 1838. They settled near the present day village of Westville, Oklahoma, where they raised a family of eight, five boys and three girls. In 1861 the Civil War started. One would think that an Indian who had been forcibly evicted from his home in Georgia and moved to Indian Territory would not have warm feelings about the United States. Redbird enlisted in the Union Army, and after training he was commissioned a First Lieutenant in the Union Artillery of the Second Brigade. Redbird’s son Samuel served as an enlisted man in the same unit. Redbird served in the Union Army from July 11,1862 until May 31,1865. He was mustered out at Fort Gibson, Indian Territory. His unit was in the battle of Newtonia, Missouri during Sept. -

Cherokees in Arkansas
CHEROKEES IN ARKANSAS A historical synopsis prepared for the Arkansas State Racing Commission. John Jolly - first elected Chief of the Western OPERATED BY: Cherokee in Arkansas in 1824. Image courtesy of the Smithsonian American Art Museum LegendsArkansas.com For additional information on CNB’s cultural tourism program, go to VisitCherokeeNation.com THE CROSSING OF PATHS TIMELINE OF CHEROKEES IN ARKANSAS Late 1780s: Some Cherokees began to spend winters hunting near the St. Francis, White, and Arkansas Rivers, an area then known as “Spanish Louisiana.” According to Spanish colonial records, Cherokees traded furs with the Spanish at the Arkansas Post. Late 1790s: A small group of Cherokees relocated to the New Madrid settlement. Early 1800s: Cherokees continued to immigrate to the Arkansas and White River valleys. 1805: John B. Treat opened a trading post at Spadra Bluff to serve the incoming Cherokees. 1808: The Osage ceded some of their hunting lands between the Arkansas and White Rivers in the Treaty of Fort Clark. This increased tension between the Osage and Cherokee. 1810: Tahlonteeskee and approximately 1,200 Cherokees arrived to this area. 1811-1812: The New Madrid earthquake destroyed villages along the St. Francis River. Cherokees living there were forced to move further west to join those living between AS HISTORICAL AND MODERN NEIGHBORS, CHEROKEE the Arkansas and White Rivers. Tahlonteeskee settled along Illinois Bayou, near NATION AND ARKANSAS SHARE A DEEP HISTORY AND present-day Russellville. The Arkansas Cherokee petitioned the U.S. government CONNECTION WITH ONE ANOTHER. for an Indian agent. 1813: William Lewis Lovely was appointed as agent and he set up his post on CHEROKEE NATION BUSINESSES RESPECTS AND WILL Illinois Bayou. -

800.438.1601
Cherokee Welcome Center VisitCherokeeNC.com 800.438.1601 Oconaluftee Indian Village, “ Unto These Hills” Outdoor Drama VisitCherokeeNC.com 866.554.4557 Fisheries & Wildlife Management FishCherokee.com 828.554.6110 Museum of the Cherokee Indian CherokeeMuseum.org 828.497.3481 Sequoyah National Golf Club SequoyahNational.com 828.497.3000 Qualla Arts and Crafts Mutual, Inc. QuallaArtsAndCrafts.com 828.497.3103 VisitCherokeeNC.com | 800.438.1601 This is what Chapter II: Strangers I was told In 1540, Spanish explorer and conquistador Hernando de perception of the region. Peace made Soto came through here looking for gold, demanding food, alliances irrelevant and mounting when I was young. fighting, enslaving—despite what you may have heard, he pressure from land speculators made wasn’t a great guy. Worse were the diseases that came with the Cherokees an inconvenience. Cherokees begin a story the way their people have him. Lacking the immunity to combat these afflictions, In 1830 Andrew Jackson signed the for generations. It’s only fitting to start the story of indigenous peoples were nearly eradicated, victim to Indian Removal Act offering the Eastern Band of Cherokee Indians the same way. plagues such as smallpox, measles, and influenza. territory out west in exchange for Chapter I: A Long Time Ago Nevertheless, the Cherokees continued their homeland. Five years later came the to work through diplomacy with the Treaty of New Echota, which ceded to the The Cherokees were hunters and gatherers, foraging newcomers for the next 200 years. federal government most of the Cherokee lands the Great Smoky Mountains and the lowlands east of the Mississippi, resulting in what is now By the late eighteenth century, seventy-five percent of the Southern Appalachians for food while referred to as the “Trail of Tears.” of Cherokee land had been lost through treaties with hunting, fishing, and trapping game. -

Cherokee Genealogy Resource Presentation
FindingFinding youryour CherokeeCherokee AncestorsAncestors ““MyMy GrandmotherGrandmother waswas aa CherokeeCherokee Princess!Princess! ”” WhereWhere toto begin?begin? Information to collect: Names (including maiden names of females) Date and place of birth Date and place of marriage Date and place of death Names of siblings (i.e., brothers and sisters) and Rolls and Roll Numbers SampleSample IndividualIndividual InformationInformation Name:Name: WilliamWilliam CoxCox Born:Born: 77--JuneJune --18941894 inin DelawareDelaware Dist,Dist, CherokeeCherokee NationNation Married:Married: 1515 --OctoberOctober --19191919 inin BlountBlount County,County, TennesseeTennessee toto PollyPolly MorrisMorris Died:Died: 33--AprilApril --19731973 inin Nashville,Nashville, TennesseeTennessee RollRoll // CensusCensus Information:Information: 18961896 CensusCensus // DelawareDelaware DistDist -- RollRoll #517#517 BirthBirth RecordsRecords Oklahoma birth records have been kept since 1925 and are availab le from: Division of Vital Records Oklahoma State Dept. of Health 100 NE 10th Ave PO Box 53551 Oklahoma City, OK 73152 -3551 NOTE: Before 1947, all birth records are filed under the father' s name. After 1947, all birth records are filed under the child's name. Birth Affidavits for Minor Cherokees born (1902 to 1906) were in cluded in the Dawes Applications, and are available from: Oklahoma Historical Society 2401 N Laird Oklahoma City, OK 73105 -4997 Guion Miller Applications also include birthdates and proof of family relationships. These are available -

SEQUOYAH FUND ANNUAL REPORT 2016 CONNECTED SEQUOYAH FUND 2016 2016 Was a Year of Connections for Sequoyah Fund
SEQUOYAH FUND ANNUAL REPORT 2016 CONNECTED SEQUOYAH FUND 2016 2016 was a year of connections for Sequoyah Fund LETTER FROM RUSS Dear Stakeholders: Connections to New Markets The Authentically Cherokee program is gaining 2016 was a year of connections for Sequoyah momentum, accessing markets outside tradition- Fund. As a Community Development Financial In- al sales channels. Artists are now able to directly stitution (CDFI), our role is more than just a lender; access the tourists who visit The Gilded Basket in after all, “Community Development” comes first the heart of Harrah’s Casino. They are also able to in our description. That aspect of what we do was sell globally through the Authentically Cherokee. prominent in 2016, as we focused on connecting com website. Our next step is to help other types our clients to resources, new markets, and other of businesses reach new markets. clients. CONNECTED Connections to Other Clients Connecting Clients to Resources Our clients are stronger when they work together. Sequoyah Fund clients often need more than mon- Sequoyah Fund has the unique ability to connect ey – they need to be connected with consultants local businesses that buy from and barter with one and other experts, academic programs, peers, and another, share expertise and experiences, and TO ONE different forms of capital. In 2016, we renewed and work together to build their businesses and the strengthened relationships with the Small Business local economy. Centers located at the area’s three community LEFT: “The Smokies Awaken” colleges, SCORE (Service Corps of Retired Execu- We look forward to continuing making connections Jeremy Wilson Photography tives), and other area CDFIs, all while maintaining in 2017 and beyond, because all of us are stronger our strong relationship with our closest resource than each of us. -

Cherokee National Records
Indian Archives Microfilm Guide Series 1: Cherokee National Records Compiled by Katie Bush Series 1: Cherokee National Records Table of Contents Census p. 4 Cherokee National Records (bound volumes) p. 8, 87 Canadian District Records p. 16 Cooweescoowee District Court Records p. 18 Delaware District Records p. 25 Flint District Records p. 31 Going Snake District Records p. 33 Illinois District Records p. 36 Saline District Records p. 40 Sequoyah District Records p. 43 Tahlequah District Records p. 45 Cherokee Citizenship p. 51 Cherokee National Records: Letters Sent, Letters Received, and other Documents (topics arranged in alphabetical order) p. 62 Volume Microfilm # Volume Microfilm # Volume Microfilm # Volume 1 CHN 22 Volume 42 CHN 28 Volume 84 CHN 35 Volume 1A CHN 22 Volume 43 CHN 31 Volume 85 CHN 36 Volume 1B CHN 22 Volume 44 CHN 28 Volume 86 CHN 36 Volume 2 CHN 22 Volume 45 CHN 24 Volume 87 CHN 34 Volume 3 CHN 22 Volume 46 CHN 25 Volume 88 CHN 33 Volume 4 CHN 22 Volume 47 CHN 25 Volume 89 CHN 36 Volume 5 CHN 22 Volume 48 CHN 28 Volume 90 CHN 35 Volume 6 CHN 23 Volume 49 CHN 29 Volume 91 CHN 33 Volume 7 CHN 23 Volume 50 CHN 27 Volume 92 CHN 33 Volume 8 CHN 23 Volume 51 CHN 29 Volume 93 CHN 34 Volume 9 CHN 23 Volume 51A CHN 24 Volume 94 CHN 33 Volume 10 CHN 23 Volume 52 CHN 28 Volume 95 CHN 35 Volume 11 CHN 23 Volume 53 CHN 31 Volume 96 CHN 33 Volume 12 CHN 23 Volume 54 CHN 31 Volume 97 CHN 32 Volume 13 CHN 23 Volume 55 CHN 25 Volume 97A CHN 38 Volume 14 CHN 23 Volume 56 CHN 117 Volume 97B CHN 38 Volume 15 Not microfilmed Volume 57 -
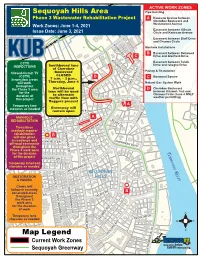
Sequoyah Hills Area Map Legend
NORTH BELLEMEADE AVE ACTIVE WORK ZONES Sequoyah Hills Area Pipe-bursting Phase 3 Wastewater Rehabilitation Project A Kenesaw Avenue between Cherokee Boulevard and Work Zones: June 1-4, 2021 Westerwood Avenue Easement between Hillvale Issue Date: June 3, 2021 KINGSTON PIKE Circle and Kenesaw Avenue Easement between Bluff Drive and Cheowa Circle BOXWOOD SQ Manhole Installations B Easement between Dellwood C Drive and Glenfield Drive KITUWAH TRL CCTV Easement between Talahi Southbound lane Drive and Iskagna Drive INSPECTIONS EAST HILLVALE TURN of Cherokee Paving & Restoration Closed-Circuit TV BoulevardWEST HILLVALE TURN CLOSED (CCTV) D C Boxwood Square Inspection crews 7 a.m. – 3 p.m., will work Thursday, June 4 Natural Gas System Work throughout LAKE VIEW DR the Phase 3 area Northbound D Cherokee Boulevard for the lane will be used between Kituwah Trail and to alternate Cheowa Circle (June 4 ONLY duration of weather permitting) this project traffic flow with flaggers present Temporary lane A closures as needed WOODHILLGreenway PL will remain openHILLVALE CIR MANHOLE A BLUFF DR REHABILITATION CHEOWA CIR Trenchless DELLWOOD DR manhole repairs/ OAKHURST DR KENESAW AVE TOWANDArehabilitation TRL B will take place in roadwaysSCENIC DR and GLENFIELD DR CHEROKEE BLVD off-road easements throughout the Phase 3 work zone Tennessee River for the duration of this project KENILWORTH DR Temporary lane/road closures as needed ALTA VISTA WAY WINDGATE ST ISKAGNA DR WOODLAND DR SEQUOYAH RESTORATION HILLS & PAVING Crews will EAST NOKOMIS CIR follow in recently B excavated areas WEST NOKOMIS CIR throughoutSAGWA DR TALAHI DR the Phase 3 work area SOUTHGATE RD for the duration of work KENESAW AVE TemporaryBLUFF VIEW RD lane closures as needed KEOWEE AVE TUGALOO DR W E S Map LegendAGAWELA AVE TALILUNA AVE Current Work Zones Sequoyah Greenway CHEROKEE BLVD. -

World Stage Curriculum
World Stage Curriculum Washington Irving’s Tour 1832 TEACHER You have been given a completed world stage and a world stage that your students can complete. This world stage is a snapshot of the world with Oklahoma, Cherokee Nation and Muscogee Creek Nation, at its center. The Pawnee, Comanche, and Kiowa were out to the west. Europe is to the north and east. Africa is to the south and east. South America is south and a bit east. Asia and the Pacific are to the west. Use a globe to show your students that these directions are accurate. Students - Directions 1. Your teacher will assign one of these actors to you. 2. After research, note the age of the actor in 1832, the year that Irving, Ellsworth, Pourtalès, and Latrobe took a Tour on the Oklahoma prairies. 3. Place the name and age of the actor in the right place on the World Stage. 4. Write a biographical sketch about the actor. 5. Make a report to the class, sharing the biographical sketch, the age of the actor in 1832, and the place the actor was at that time. 6. Listen to all the other reports and place all of the actors in their correct locations with their correct ages in 1832. Students - Information 1. The majority of the characters can be found in your public library in biographies and encyclopedia. You will need a library card to access this information. There is enough information about each actor for a biographical sketch. 2. Other actors can be found on the Internet. -

Researching Native Americans at the National Archives in Atlanta
Researching Individual Native Americans at the National Archives at Atlanta National Archives at Atlanta 5780 Jonesboro Road Morrow, GA 30260 770-968-2100 www.archives.gov/southeast E-Mail: [email protected] Spring, 2009 Researching Individual Native Americans at the National Archives at Atlanta Table of Contents Introduction ............................................................................................................................................... 1 Tribal Association ............................................................................................................................ 1 Race .................................................................................................................................................. 2 Tribal Membership ........................................................................................................................... 2 Textual Records ............................................................................................................................... 2 Native American Genealogy ............................................................................................................ 3 Published Resources ......................................................................................................................... 3 Online Resources ............................................................................................................................. 4 Dawes Commission .................................................................................................................................. -
Note to Users
NOTE TO USERS This reproduction is the best copy available. ® UMI Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. Reproduced with with permission permission of the of copyright the copyright owner. owner.Further reproductionFurther reproduction prohibited without prohibited permission. without permission. LIFE HISTORY OF SAMMY STILL, A TRADITIONAL WESTERN CHEROKEE IN MODERN AMERICA By Juliette E. Sligar Submitted to the Faculty of the College of Arts and Sciences of American University in PartialFulfillment of the Requirements for the Degree of Master of Arts In Public Anthropology Chair: Richard J. Dent"'' (\ Cesare Marino Dean of the College of Arts and Sciences Date 2005 American University Washington, D.C. 20016 AMERICAN UNIVERSITY LIBRARY Reproduced with permission of the copyright owner. Further reproduction prohibited without permission. UMI Number: 1425664 Copyright 2005 by Sligar, Juliette E. All rights reserved. INFORMATION TO USERS The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleed-through, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. ® UMI UMI Microform 1425664 Copyright 2005 by ProQuest Information and Learning Company. All rights reserved. This microform edition is protected against unauthorized copying under Title 17, United States Code. ProQuest Information and Learning Company 300 North Zeeb Road P.O. Box 1346 Ann Arbor, Ml 48106-1346 Reproduced with permission of the copyright owner.