Progression of Microalbuminuria to Proteinuria in Type 1 Diabetes Nonlinear Relationship with Hyperglycemia James H
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
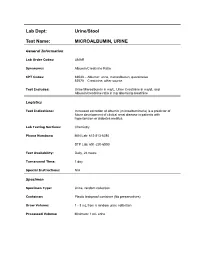
Lab Dept: Urine/Stool Test Name: MICROALBUMIN, URINE
Lab Dept: Urine/Stool Test Name: MICROALBUMIN, URINE General Information Lab Order Codes: UMAR Synonyms: Albumin/Creatinine Ratio CPT Codes: 82043 – Albumin: urine, microalbumin, quantitative 82570 – Creatinine; other source Test Includes: Urine Microalbumin in mg/L, Urine Creatinine in mg/dL and Albumin/creatinine ratio in mg albumin/g creatinine Logistics Test Indications: Increased excretion of albumin (microalbuminuria) is a predictor of future development of clinical renal disease in patients with hypertension or diabetes mellitus. Lab Testing Sections: Chemistry Phone Numbers: MIN Lab: 612-813-6280 STP Lab: 651-220-6550 Test Availability: Daily, 24 hours Turnaround Time: 1 day Special Instructions: N/A Specimen Specimen Type: Urine, random collection Container: Plastic leakproof container (No preservatives) Draw Volume: 1 - 3 mL from a random urine collection Processed Volume: Minimum: 1 mL urine Collection: A random urine sample may be obtained by voiding into a urine cup and is often performed at the laboratory. Bring the refrigerated container to the lab. Make sure all specimens submitted to the laboratory are properly labeled with the patient’s name, medical record number and date of birth. Special Processing: Lab Staff: Centrifuge specimen before analysis. Patient Preparation: Sample should not be collected after exertion, in the presence of a urinary tract infection, during acute illness, immediately after surgery, or after acute fluid load. Sample Rejection: Mislabled or unlabeled specimens; samples contaminated with blood Interpretive Reference Range: Albumin/creatinine ratio (A/C <30 mg/g Normal ratio) 30 - 299 mg/g Microalbuminuria >300 mg/g Clinical albuminuria Urine Creatinine: No reference ranges established Critical Values: N/A Limitations: Due to variability in urinary albumin excretion, at least two of three test results measured within a 6-month period should show elevated levels before a patient is designated as having microalbuminuria. -

A Dipstick Test Combined with Urine Specific Gravity Improved the Accuracy of Proteinuria Determination in Pregnancy Screening
Kobe J. Med. Sci., Vol. 56, No. 4, pp. E165-E172, 2010 A Dipstick Test Combined with Urine Specific Gravity Improved the Accuracy of Proteinuria Determination in Pregnancy Screening NATSUKO MAKIHARA1, MINEO YAMASAKI1,2, HIROKI MORITA1, and HIDETO YAMADA1* 1Division of Obstetrics and Gynecology, Department of Surgery-related, and 2Division of Integrated Medical Education, Department of Community Medicine and Social Healthcare Science, Kobe University Graduate School of Medicine, 7-5-1 Kusunoki-cho, Chuo-ku, Kobe, 650-0017, Japan. Received 12 July 2010/ Accepted 20 August 2010 Key Words: dipstick test, pregnancy proteinuria, protein/creatinine ratio, urine specific gravity Proteinuria screening using a semi-quantitative dipstick test of the spot urine in antenatal clinic is known to have high false-positive rates. The aim of this study was to assess availability of a dipstick test combined with the urine specific gravity for the determination of pathological proteinuria. A dipstick test was performed on 582 urine samples obtained from 283 pregnant women comprising 260 with normal blood pressure and 23 with pregnancy-induced hypertension. The urine protein (P) and creatinine (C) concentrations, specific gravity (SG), P/C ratio were determined, and compared with dipstick test results. The P concentration increased along the stepwise augmentations in dipstick test result. Frequencies of the urine samples with 0.265 or more P/C ratio were 0.7% with − dipstick test result, 0.7% with the ± result, 3.3% with the 1+ result, and 88.9% with the ≥2+ result. However, if the urine specific gravity was low, frequencies of the high P/C ratio were 5.0% with ± dipstick test result and 9.3% with the 1+ result. -

Prevalence of Microalbuminuria and Associated Risk Factors Among Adult Korean Hypertensive Patients in a Primary Care Setting
Hypertension Research (2013) 36, 807–823 & 2013 The Japanese Society of Hypertension All rights reserved 0916-9636/13 www.nature.com/hr ORIGINAL ARTICLE Prevalence of microalbuminuria and associated risk factors among adult Korean hypertensive patients in a primary care setting Yon Su Kim 1, Han Soo Kim2, Ha Young Oh3, Moon-Kyu Lee4, Cheol Ho Kim5, Yong Soo Kim6,DavidWu6, Amy O Johnson-Levonas6 and Byung-Hee Oh7 Microalbuminuria is an early sign of nephropathy and an independent predictor of end-stage renal disease. The purpose of this study was to assess microalbuminuria prevalence and its contributing factors in Korean hypertensive patients. This cross-sectional study enrolled male and female patients of X35 years old with an essential hypertension diagnosis as made by 841 physicians in primary care clinics and 17 in general hospitals in the Republic of Korea between November 2008 and July 2009. To assess microalbuminuria prevalence, urine albumin/creatinine ratio (UACR) was measured in patients with a positive dipstick test. Of the 40 473 enrolled patients, 5713 (14.1%) had a positive dipstick test. Of 5393 patients with a positive dipstick test and valid UACR values, 2657 (6.6%) had significantly elevated UACR (X30 lgmgÀ1), 2158 (5.4%) had microalbuminuria (30 lgmgÀ1pUACR o300 lgmgÀ1) and 499 (1.2%) had macroalbuminuria (UACR X300 lgmgÀ1). Based on multivariate analysis, independent factors associated with elevated UACR included low adherence to antihypertensive medication (23% higher; P ¼ 0.042), poorly controlled blood pressure (BP; 38% higher for systolic BP/diastolic BP X130 mm Hg/X80 mm Hg; Po0.001), obesity (47% higher for body mass index (BMI) X25.0 kg m À2; Po0.001), age (17% lower and 58% higher for age categories 35–44 years (P ¼ 0.043) and 475 years (Po0.001), respectively) and a prior history of diabetes (151% higher; Po0.001) and kidney-related disease (71% higher; Po0.001). -

Proteinuria and Albuminuria: What’S the Difference? Cynthia A
EXPERTQ&A Proteinuria and Albuminuria: What’s the Difference? Cynthia A. Smith, DNP, CNN-NP, FNP-BC, APRN, FNKF What exactly is the difference between TABLE Q the protein-to-creatinine ratio and the Persistent Albuminuria Categories microalbumin in the lab report? How do they compare? Category Description UACR For the non-nephrology provider, the options for A1 Normal to mildly < 30 mg/g evaluating urine protein or albumin can seem con- increased (< 3 mg/mmol) fusing. The first thing to understand is the impor- tance of assessing for proteinuria, an established A2 Moderately 30-300 mg/g marker for chronic kidney disease (CKD). Higher increased (3-30 mg/mmol) protein levels are associated with more rapid pro- A3 Severely > 300 mg/g gression of CKD to end-stage renal disease and in- increased (> 30 mg/mmol) creased risk for cardiovascular events and mortality in both the nondiabetic and diabetic populations. Abbreviation: UACR, urine albumin-to-creatinine ratio. Monitoring proteinuria levels can also aid in evaluat- Source: KDIGO. Kidney Int. 2012.1 ing response to treatment.1 Proteinuria and albuminuria are not the same low-up testing. While the UACR is typically reported thing. Proteinuria indicates an elevated presence as mg/g, it can also be reported in mg/mmol.1 Other of protein in the urine (normal excretion should be options include the spot urine protein-to-creatinine < 150 mg/d), while albuminuria is defined as an “ab- ratio (UPCR) and a manual reading of a reagent strip normal loss of albumin in the urine.”1 Albumin is a (urine dipstick test) for total protein. -
Understanding What It Means to Have Protein in Your Urine Understanding What It Means to Have Protein in Your Urine
UNDERSTANDINGUnderstanding WHAT ITYour MEANS TO HAVE Hemodialysis PROTEINAccess Options IN YOUR URINE 2 AAKP: Understanding What It Means to Have Protein in Your Urine Understanding What It Means to Have Protein in Your Urine The kidneys are best known for making urine. This rather simple description does not tell the whole story. This brochure describes other important functions of the kidneys; including keeping protein in the blood and not letting any of the protein in the liquid (plasma) part of blood escape into the urine. Proteinuria is when “Proteinuria” is when kidneys allow proteins to kidneys appear in the urine and be lost from the body. allow Proteinuria is almost never normal, but it can proteins to be normal - rarely - in some healthy, active appear in the urine children or young adults. and be The kidneys are paired organs located on either lost from the body. side of the backbone. They are located at the Proteinuria level of the lowest part of the rib cage. They are is almost the size of an adult fist (4.5 – 5 inches in length). never Together the two kidneys receive a quarter of normal, but it can the blood that is pumped from the heart every be normal minute. This large blood flow is needed in order - rarely - for the kidneys to do one of the kidneys’ main in some jobs: healthy, active • remove waste products in the blood every children day or young adults. • keep the body in balance by eliminating the extra fluids and salts we consume on a regular basis. -

Storm in a Pee Cup: Hematuria and Proteinuria
Storm in a Pee Cup: Hematuria and Proteinuria Sudha Garimella MD Pediatric Nephrology, Children's Hospital-Upstate Greenville SC Conflict of Interest • I have no financial conflict of interest to disclose concerning this presentation. Objectives • Interpret the current guidelines for screening urinalysis, and when to obtain a urinalysis in the pediatric office. • Interpret the evaluation of asymptomatic/isolated proteinuria and definitions of abnormal ranges. • Explain the evaluation and differential diagnosis of microscopic hematuria. • Explain the evaluation and differential diagnosis of gross hematuria. • Explain and discuss appropriate referral patterns for hematuria. • Racial disparities in nephrology care 1. APOL-1 gene preponderance in African Americans and risk of proteinuria /progression(FSGS) 2. Race based GFR calculations which have caused harm 3. ACEI/ARB usage in AA populations: myths and reality Nephrology Problems in the Office • Hypertension • Proteinuria • Microscopic Hematuria • Abnormal Renal function The Screening Urinalysis • Choosing Wisely: • Don’t order routine screening urine analyses (UA) in healthy, asymptomatic pediatric patients as part of routine well child care. • One study showed that the calculated false positive/transient abnormality rate approaches 84%. • Population that deserves screening UA: • patients who are at high risk for chronic kidney disease (CKD), including but not necessarily limited to patients with a personal history of CKD, acute kidney injury (AKI), congenital anomalies of the urinary tract, acute nephritis, hypertension (HTN), active systemic disease, prematurity, intrauterine growth retardation, or a family history of genetic renal disease. • https://www.choosingwisely.org/societies/american-academy-of-pediatrics-section-on- nephrology-and-the-american-society-of-pediatric-nephrology/ Screening Urinalysis: Components A positive test for leukocyte esterase may be seen in genitourinary inflammation, irritation from instrumentation or catheterization, glomerulonephritis, UTIs and sexually transmitted infections. -

Hematuria in the Child
Hematuria and Proteinuria in the Pediatric Patient Laurie Fouser, MD Pediatric Nephrology Swedish Pediatric Specialty Care Hematuria in the Child • Definition • ³ 1+ on dipstick on three urines over three weeks • 5 RBCs/hpf on three fresh urines over three weeks • Prevalence • 4-6% for microscopic hematuria on a single specimen in school age children • 0.3-0.5% on repeated specimens Sources of Hematuria • Glomerular or “Upper Tract” – Dysmorphic RBCs and RBC casts – Tea or cola colored urine – Proteinuria, WBC casts, renal tubular cells • Non-Glomerular or “Lower Tract” – RBCs have normal morphology – Clots/ Bright red or pink urine The Glomerular Capillary Wall The Glomerular Capillary Wall Glomerular Causes of Hematuria • Benign or self-limiting – Benign Familial Hematuria – Exercise-Induced Hematuria – Fever-Induced Hematuria Glomerular Causes of Hematuria • Acute Glomerular Disease – Poststreptococcal/ Postinfectious – Henoch-Schönlein Purpura – Sickle Cell Disease – Hemolytic Uremic Syndrome Glomerular Causes of Hematuria • Chronic Glomerular Disease – IgA Nephropathy – Henoch-Schönlein Purpura or other Vasculitis – Alport Syndrome – SLE or other Collagen Vascular Disease – Proliferative Glomerulonephritis Non-Glomerular Hematuria • Extra-Renal • UTI • Benign urethralgia +/- meatal stenosis • Calculus • Vesicoureteral Reflux, Hydronephrosis • Foreign body • Rhabdomyosarcoma • AV M • Coagulation disorder Non-Glomerular Hematuria • Intra-Renal • Hypercalciuria • Polycystic Kidney Disease • Reflux Nephropathy with Renal Dysplasia • -

Screening for Microalbuminuria in Patients with Diabetes
Screening for Microalbuminuria in Patients with Diabetes Why? How? To identify patients with diabetic kidney disease (DKD). Test for microalbuminuria To distinguish DKD patients from diabetic patients with chronic kidney disease (CKD) from other causes. The latter require further investigation and possibly different No clinical management. + for albumin Because markers of kidney damage are required to detect early stages of CKD. Yes Estimated glomerular filtration rate (eGFR) alone can only detect CKD stage 3 or worse. Condition that may invalidate* urine albumin excretion When? Yes Begin screening: No Treat and/or wait until No resolved. Repeat test. In type 1 diabetes – 5 years after diagnosis, then annually + for protein? In type 2 diabetes – at diagnosis, then annually Yes Repeat microalbuminuria test twice within 3-6 month period. Is it Microalbuminuria? Measure urinary albumin-creatinine ratio (ACR) Yes Rescreen No in a spot urine sample. 2 of 3 tests positive? in one year Category Spot (mg/g creatinine) Yes Normoalbuminuria <30 Microalbuminuria, begin treatment Microalbuminuria 30-300 Macroalbuminuria >300 * Exercise within 24 hours, infection, fever, congestive heart failure, marked hyperglycemia, pregnancy, marked hypertension, urinary tract infection, and hematuria. Screening for Microalbuminuria in Patients with Diabetes Is it DKD? CKD should be attributable to diabetes if: Macroalbuminuria is present; or Microalbuminuria is present: • in the presence of diabetic retinopathy • in type 1 diabetes of at least 10 years’ duration Albuminuria GFR (mL/min) CKD Stage* Normoalbuminuria Microalbuminuria Macroalbuminuria >60 1 + 2 At risk† Possible DKD DKD 30-60 3 Unlikely DKD‡ Possible DKD DKD <30 4 + 5 Unlikely DKD‡ Unlikely DKD DKD * Staging may be confounded by treatment because RAS blockade could render microalbuminuric patients normoalbuminuric and macroalbuminuric patients microalbuminuric. -

Blood Or Protein in the Urine: How Much of a Work up Is Needed?
Blood or Protein in the Urine: How much of a work up is needed? Diego H. Aviles, M.D. Disclosure • In the past 12 months, I have not had a significant financial interest or other relationship with the manufacturers of the products or providers of the services discussed in my presentation • This presentation will not include discussion of pharmaceuticals or devices that have not been approved by the FDA Screening Urinalysis • Since 2007, the AAP no longer recommends to perform screening urine dipstick • Testing based on risk factors might be a more effective strategy • Many practices continue to order screening urine dipsticks Outline • Hematuria – Definition – Causes – Evaluation • Proteinuria – Definition – Causes – Evaluation • Cases You are about to leave when… • 10 year old female seen for 3 day history URI symptoms and fever. Urine dipstick showed 2+ for blood and no protein. Questions? • What is the etiology for the hematuria? • What kind of evaluation should be pursued? • Is this an indication of a serious renal condition? • When to refer to a Pediatric Nephrologist? Hematuria: Definition • Dipstick > 1+ (large variability) – RBC vs. free Hgb – RBC lysis common • > 5 RBC/hpf in centrifuged urine • Can be – Microscopic – Macroscopic Hematuria: Epidemiology • Microscopic hematuria occurs 4-6% with single urine evaluation • 0.1-0.5% of school children with repeated testing • Gross hematuria occurs in 1/1300 Localization of Hematuria • Kidney – Brown or coke-colored urine – Cellular casts • Lower tract – Terminal gross hematuria – (Blood -

Sympathetic Overactivity Predicts Microalbuminuria in Pregnancy
Original Article DOI: 10.7860/JCDR/2018/36738.12412 Sympathetic Overactivity Predicts Section Biochemistry Microalbuminuria in Pregnancy INDER PAL KAUR1, SUKANYA GANGOPADHYAY2, KIRAN SINGH3, MAMTA TYAGI4, GAUTAM SARKAR5 ABSTRACT pregnancy-induced hypertension. Statistical analysis was done Introduction: Microalbuminuria is a frequent feature in with appropriate tests using Graphpad Prizm (version 7.04). pregnancy, as the latter is a state of haemodynamic changes Results: The level of urinary microalbumin was found to be and sympathetic overactivity. Both sympathetic overactivity {as high in the pregnant group. Albumin Creatinine Ratio (ACR) was measured by Heart Rate Variability (HRV)} and microalbuminuria raised in pregnancy (72.35±50.29 in third trimester, 84.48±52.61 are individually linked with hypertension. So, presence of these in second trimester and 17.59±6.19 in non-pregnant control conditions in pregnant women could be the reason for the group; p<0.001). The HRV study shows that sympathetic increasing prevalence of Pregnancy Induced Hypertension dominance is more during pregnancy as compared to non- (PIH)/Preeclampsia. pregnant (2.09±0.91 in pregnant and 1.04±0.65 in non-pregnant Aim: To measure HRV and urinary microalbumin excretion group). simultaneously in pregnant women. Conclusion: It was concluded that there is a neurogenic role Materials and Methods: In this hospital-based study, pregnant for the causation of microalbuminuria in pregnancy. As this women in 2nd and 3rd trimester were recruited along with age- condition predicts the development of pre-eclampsia/eclampsia matched controls. Their sympathetic activity and urinary in later pregnancy, all the methods targeting generalised stress albumin-creatinine ratio were recorded. -

Microalbuminuria: a Potential Marker for Adverse 2018; 2(5): 64-68 Obstetric and Fetal Outcome Received: 11-07-2018 Accepted: 12-08-2018 Dr
International Journal of Clinical Obstetrics and Gynaecology 2018; 2(5): 64-68 ISSN (P): 2522-6614 ISSN (E): 2522-6622 © Gynaecology Journal Microalbuminuria: A potential marker for adverse www.gynaecologyjournal.com 2018; 2(5): 64-68 obstetric and fetal outcome Received: 11-07-2018 Accepted: 12-08-2018 Dr. K Lavanyakumari, Dr. Sangeereni, Dr. S Sethupathy and Dr. Chithra S Dr. K Lavanyakumari Professor and Head, Department of Obstetrics and Abstract Gynaecology, Rajah Muthiah Background: Obstetric and perinatal outcome is an index of health in society. Various markers are being [12, 13] Medical College, Annamalai searched so as to increase the well being of mother and fetus in pregnancy. Several Studies have University, Chidambaram, revealed an association between microalbuminuria and obstetric outcome. Microalbuminuria can be used as Tamil Nadu, India prognostic marker in evaluation of gestational hypertension, preterm labour, GDM, PPROM, IUGR. Objective: This study was done to evaluate whether microalbuminuria which was evaluated at late second Dr. Sangeereni trimester could serve as marker for adverse obstetric and neonatal outcome. Lecturer, Department of Obstetrics Materials and Methods: A Prospective case control study was carried out on 150 people. Urine tested for and Gynaecology, Rajah Muthiah urine micro albumin and creatinine and ACR ratio was calculated. Among 150 pregnant women 27 were Medical College, Annamalai positive for microalbuminuria and were categorised as group A. Pregnant women without University, Chidambaram, microalbuminuria were considered as group B (controls). Both group A and group B were compared for Tamil Nadu, India obstetric outcomes. Results: Significant association found between group A and gestational hypertension and preterm labour. -

Microalbuminuria in Essential Hypertension
Journal of Human Hypertension (2002) 16 (Suppl 1), S74–S77 2002 Nature Publishing Group All rights reserved 0950-9240/02 $25.00 www.nature.com/jhh Microalbuminuria in essential hypertension G Crippa Hypertension Unit, Department of Internal Medicine, Civil Hospital, Via Taverna 49, 29100 Piacenza, Italy Microalbuminuria (urinary albumin excretion equal to to blood pressure reduction, but angiotensin-converting 30–300 mg/24 h) is a reliable indicator of premature enzyme inhibitors and angiotensin-II-receptor antagon- cardiovascular mortality in diabetic patients and in the ists show an additional beneficial effect on urinary general population. In insulin-dependent and non-insu- albumin excretion. Whether the reduction of micro- lin-dependent diabetes mellitus microalbuminuria is a albuminuria obtained through pharmacological inter- marker of initial diabetic nephropathy and predicts the vention has favourable prognostic implications remain evolution toward renal insufficiency. In essential to be demonstrated. However, screening for micro- hypertension the clinical and prognostic role of micro- albuminuria is a relatively easy and inexpensive pro- albuminuria is more controversial. While it is a recog- cedure and reveals a potentially treatable abnormality. nised marker of cardiovascular complications and a Thus, considering that microalbuminuria identifies reliable predictor of ischaemic heart disease, its prog- hypertensive subjects at higher risk than standard, uri- nostic value on the risk of progressive renal alterations nary albumin excretion should be routinely measured in is still uncertain because no prospective studies, taking hypertensive patients and, in the presence of micro- microalbuminuria as a selection criterion and renal albuminuria, antihypertensive treatment should be insufficiency as an end point, are available. Blood intensified in order to obtain an optimal blood press- pressure control with antihypertensive drugs is ure control.