Bihar School-Based Deworming Programme
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

District Plan 2011 - 12
I DISTRICT PLAN 2011 - 12 SUPAUL - i I Submitted by : District Planning Committee, Supaul Submitted to: Department of Planning & Development, Government of Bihar DISTRICT PLAN 2011 - 12 SUPAUL ¥ V *k g f II A © H f: © f&T SJkH*»»* Submitted by : District Planning Committee, Supaul Submitted to: Department of Planning & Development, Government of Bihar ACKNOWLEDGEMENTS For sustainable and planned economic development it is essential to formulate the Annual District Plan on the basis of available resources. As per the direction of the Department of Planning and Development, Government of Bihar, with an objective to prepare the effective Plan, we have collected relevant information and data ensuring the assimilation of district level important components from various departments as well as the priority sectors like Health, Education, Livelihood and Infrastructure etc. Keeping in view the past experience of formulation and implementation of various sectoral Action Annual Plans and recent directions of the department the Annual District Plan 2011 -12 for Rs. 103142.3 89 lakh has been prepared for the maximum utilization of available resources, so that the socio-economic development of the district can be further accelerated. I would like to thank Mr. Kunwar Jung Bahadur, Deputy Development Commissioner, Mr. D.N. Mishra, Regional Planning officer, Kosi Division, Mr. Prakash Yadav, District Planning Officer, Mr. Vivek Sharan (Ex. District Facihtator) and Mr. D P Karn, District Facihtator, GoI-UN Joint Convergence Program for their important contribution in formulation of Annual District Plan 2011 -12 for the district of Supaul. Mr. Brajesh Kumar Vikal, DPRO also deserves special thanks for his support in the Plan formulation. -

Brief Industrial Profile of PURNEA District
P a g e | 1 G o v e r n m e n t o f I n d i a M in is t r y of M S M E Brief Industrial Profile of PURNEA District Carried out by MS ME - D e v e l opme nt I ns ti tute , M uz a ff a r pur (Ministry of MSME, Govt. of India,) Phone :-0621-2284425 Fax: 0621-2282486 e-mail:[email protected] Web- www.msmedimzfpur.bih.nic.in Page | 2 Contents S. No. Topic Page No. 1. General Characteristics of the District 3 1.1 Location & Geographical Area 4 1.2 Topography 5-6 1.3 Availability of Minerals. 7 1.4 Forest 8 1.5 Administrative set up 8-9 2. District at a glance 9-14 2.1 Existing Status of Industrial Area in the District Purnia 14 3. Industrial Scenario Of Purnia 15 3.1 Industry at a Glance - 3.2 Year Wise Trend Of Units Registered 16 3.3 Details Of Existing Micro & Small Enterprises & Artisan Units In The 17 District 3.4 Large Scale Industries / Public Sector undertakings 18 3.5 Major Exportable Item 18 3.6 Growth Trend 18 3.7 Vendorisation / Ancillarisation of the Industry 18 3.8 Medium Scale Enterprises 18 3.8.1 List of the units in –PURNEA ---- & near by Area 18 3.8.2 Major Exportable Item 18 3.9.1 Coaching Industry 19 3.9.2 Potentials areas for service industry 19 3.10 Potential for new MSMEs 19 4. -

(SJAMS) Studies on Urinary Risk Factors in Urolithiasis Patients Of
Scholars Journal of Applied Medical Sciences (SJAMS) ISSN 2320-6691 (Online) Abbreviated Key Title: Sch. J. App. Med. Sci. ISSN 2347-954X (Print) ©Scholars Academic and Scientific Publisher A Unit of Scholars Academic and Scientific Society, India Chemistry www.saspublisher.com Studies on Urinary Risk Factors in Urolithiasis Patients of Purnia Division of Bihar, India T.V.R.K. Rao*, Gunja Kumari Department of Chemistry, Purnea College, Purnia-854301 Bihar, India Abstract: Urolithiasis disease is a function of a number of risk factors. Present Original Research Article objective is to study the urinary risk factors in urolithiasis patients from Purnia division of Bihar (India). The study would lead to an understanding of the various metabolic *Corresponding author abnormalities leading to urinary stone formation in this region. Twenty four hour T.V.R.K. Rao urinary calcium, magnesium, oxalate, phosphate, uric acid and citrate were estimated in 100 urolithiasis patients (66 males & 34 females) in the age group of 18-55 yrs. Fifty Article History normal healthy persons (30 males & 20 females) in the age group of 20-55 yrs, who Received: 01.08.2018 served as controls, were also studied for the above urinary parameters. Results revealed Accepted: 05.08.2018 that hypercalciuria, hyperoxaluria and hypocitraturia are the main risk factors of Published: 30.08.2018 urolithiasis in the region. Hyperuricosuria, hypophosphaturia and hypomagnesuria also showed up as marginal risk factors in the urinary stone patients. As such, urolithiasis DOI: patient from Purnia division of Bihar should invariably be tested for urinary calcium, 10.21276/sjams.2018.6.8.28 oxalate and citrate levels. -

Business Plan for Makhana Clusters in Bihar
Business Plan for Makhana Clusters in Bihar 1 INDEX BUSINESS PLAN FOR MAKHANA CLUSTERS IN BIHAR .................................... 1 EXECUTIVE SUMMARY .............................................................................................. 4 Botany ......................................................................................................................... 8 Distribution and Habitat ............................................................................................. 9 Nutritional Value ...................................................................................................... 10 Uses ........................................................................................................................... 10 Cultivation and Harvesting of Makhana................................................................... 10 Processing of Makhana............................................................................................. 11 OBJECTIVE ..................................................................................................................... 12 APPROACH & METHODOLOGY ....................................................................................... 13 MAKHANA SECTOR ........................................................................................................ 18 CLUSTER MAPPING.................................................................................................... 19 CLUSTER DIAGRAM ...................................................................................................... -
Town Wise Revised Action Plan for Polluted River Stretches in the State of Bihar Original Application No: 200/2014 (Matter : M.C
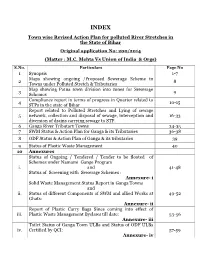
INDEX Town wise Revised Action Plan for polluted River Stretches in the State of Bihar Original application No: 200/2014 (Matter : M.C. Mehta Vs Union of India & Orgs) S.No. Particulars Page No 1 Synopsis 1-7 Maps showing ongoing /Proposed Sewerage Scheme in 2 8 Towns under Polluted Stretch & Tributaries Map showing Patna town division into zones for Sewerage 3 9 Schemes Compliance report in terms of progress in Quarter related to 4 10-15 STPs in the state of Bihar Report related to Polluted Stretches and Lying of sewage 5 network, collection and disposal of sewage, interception and 16-33 diversion of drains carrying sewage to STP. 6 Ganga River Tributary Towns 34-35 7 SWM Status & Action Plan for Ganga & its Tributaries 36-38 8 ODF Status & Action Plan of Ganga & its tributaries 39 9 Status of Plastic Waste Management 40 10 Annexures Status of Ongoing / Tendered / Tender to be floated of Schemes under Namami Gange Program i. and 41-48 Status of Screening with Sewerage Schemes : Annexure- i Solid Waste Management Status Report in Ganga Towns and ii. Status of different Components of SWM and allied Works at 49-52 Ghats: Annexure- ii Report of Plastic Carry Bags Since coming into effect of iii. Plastic Waste Management Byelaws till date: 53-56 Annexure- iii Toilet Status of Ganga Town ULBs and Status of ODF ULBs iv. Certified by QCI: 57-59 Annexure- iv 60-68 and 69 11 Status on Utilization of treated sewage (Column- 1) 12 Flood Plain regulation 69 (Column-2) 13 E Flow in river Ganga & tributaries 70 (Column-4) 14 Assessment of E Flow 70 (Column-5) 70 (Column- 3) 15 Adopting good irrigation practices to Conserve water and 71-76 16 Details of Inundated area along Ganga river with Maps 77-90 17 Rain water harvesting system in river Ganga & tributaries 91-96 18 Letter related to regulation of Ground water 97 Compliance report to the prohibit dumping of bio-medical 19 98-99 waste Securing compliance to ensuring that water quality at every 20 100 (Column- 5) point meets the standards. -
The Report of the Patna Iniversity Committee
CRITICISMS ON THE REPORT OF THE PATNA INIVERSITY COMMITTEE. T o D - t i < f |- 37S>-^STr-1sV'' i ' N l ^ C ¥ * l U - C . CRITICISMS ON THE REPORT OF THE PATNA UNIVEE SITY COMMITTEE; TABLE OF CONTENTS. P a g e Babu Badri Nath Upadhya, Korha, Pumea ... 1 Mr. P. Walfordj Principal, Bihar School of Engineering , 3 Rai Upendra Nath Ghosh, Bahadur, Deputy Collector in charge 6 of Orissa Canals, Revenue Division, iCuttack. Bihar Planters'Association ... ... ... 11 The National Society, Balasore ... ... 12 Mr. E. Schroder, Headmaster, Zila School, Bhagalpur , 13 Church Missionary Society, Calcutta ... ... , 16 Bihar Provincial Moslem League, Bankipore ... , 17 Ranchi Bihari Public ... ... ... 19 Bengali Settlers’ Association, Bhagalpur ... 20 Hon’ble Babu Bishun Prasad ... 22 Dr. Lakshmipati ... ... ... , 25 Mr. R. N . Gilchrist, Professor, Presidency College, Calcutta . 29 Mahamahopadhya Pandit Ganga Nath Jha 32 Hon’ble Maulvi Saiyid Muhammad Tahir ... 33 Edward Memorial Ayurvedic Pathshala, Aurangabad, Gaya , 36 Muhammadan Association, Bhagalpur ... ... 38 Moslem League, Bhagalpur ... ... • •• < 39 Patna Bar Association, Bankipore cat I 40 Fifth Bihar Provincial Conference ... ... 47, 63 Bengali Settlers' Association, Bihar and Orissa, Bankipore , 53 Commissioner, Bhagalpur Division ... ... 55 District Magistrate, Monghyr _ ' ' ^ ... 55 Commissioner, Patna Division ... 59 District Magistrate, Shahabad ... ... 59 Khan Sahib Saiyid Ahmad Ali Khan ••• I 60 Snbdivisional OfSoer, Buxar ... ... 61 Subdivisional Officer, Sasaram ... 61 District Magistrate, Gaya ... ... ... 61 Hon'ble Maharaja Sir Ravaneswar Praead Singh, Bahadnr, . 62 k .c.i j :.. of Gidhaur. Muhammadans of Chota Nagpur ,.l ... • 66 Commissioner, Orissa Division ... ... • 67 District Magistrate, Balasore ... ••• • 68, Pasgb District Magistrate, P’atna ... 71 Malthil Mahasabha, Darblianga 73, 86 Mr. S. Q. Huda ... ... 74 Calcutta Weekly Notes .. -
Saharsa Introduction
DISTRICT PROFILE SAHARSA INTRODUCTION Saharsa is one of the thirty-eight districts of Bihar. Saharsa district became a separate district in 1954 prior to which it was a part of Kosi division. The important rivers flowing through the district are Kosi, Baghmati. HISTORICAL BACKGROUND Earlier Saharsa district was within the Bhagalpur Division. Kosi Division was formed on 2nd October 1972 comprising of Saharsa, Purnia and Katihar district with its head quarters at Saharsa. Formerly it had no independent status and parts of Saharsa were included in the old districts of Munger & Bhagalpur. Ancient Times: In ancient times, Vaishali was the strongest republic in North-Bihar and beyond that lay the famous territory of Anguttarap. There was a small Janpad, named Apna, in Anguttarap and it included a portion of the district of Saharsa. Various sites of the district, now completely eroded and destroyed by the Kosi, viz. Biratpur, Budhiagarhi, Budhnaghat, Buddhadi, Pitahahi and Mathai are associated with Buddhism Both Anga and North Bihar (including Saharsa) continued to be independent till the early part of the sixth century B.C Between 320 and 1097 A.D Under the Guptas (from 320 A.D.), the entire North Bihar was consolidated as a Tirbhukti (province) with its capital at Vaishali. The extent of Saharsa during the period under review was upto the confines of Pundravardhanbhukti which included some of its present area. From the geographical point of view, Saharsa was the most strategically suited from being the Jayaskandharar (temporary Capital) of the Palas at the time when they were surrounded on all sides by enemies. -

District Census Handbook Madhepura
lR;eso t;rs CENSUS OF INDIA 2011 BIHAR SERIES-11 PART XII-A DISTRICT CENSUS HANDBOOK MADHEPURA VILLAGE AND TOWN DIRECTORY dh tux r .k kj u k k H C A E I Directorate of Census Operations, Bihar N D S I N U S O F B I H A R S U DISTRICT MADHEPURA P KILOMETRES T r 5 0 5 u A p o C h g a R o r T u p a U I t a h h S C H o T L R R R A T SHANKARPUR I GAMHARIA R A R KUMARKHAND A S T R C I R SINGHESHWAR ( T S R R I I GHAILARH D D I D SH S RS H ! To Jankinagar P RS arsa Sah RS m S Fro ! MADHEPURA R A MURLIGANJ T S o B R a n T m A a n k H h i A I N D I A R S I T R GWALPARA C C I BIHARIGANJ R R T T S R KISHANGANJ P I S H D U A R I PURAINI R R A R N G ALAMNAGAR A H I K T CHAUSA A C R I R R T r u Note:- District Headquarter is also the CD Block Headquarter. p U h i S B I P m o r F D L BOUNDARY, STATE ................ .......................................... D I A '' DISTRICT ...................................................... S T G R I A HEADQUARTERS: DISTRICT, C.D.BLOCK ....................... P R C T B H STATE HIGHWAY ............................................................... -

Parachuters Vs. Climbers: Economic Consequences of Barriers to Political Entry in a Democracy
PLEASE DO NOT CIRCULATE WITHOUT PERMISSION FROM THE AUTHOR Parachuters vs. Climbers: Economic Consequences of Barriers to Political Entry in a Democracy Aaditya Dar∗ Please click here for the latest version Abstract How does political selection impact local economic growth? I study the role of a legisla- tor’s background prior to joining politics and conduct primary research to compile an original dataset of politicians’ biographies. Observing the entry route of politicians allows me to clas- sify them as ‘parachuters’ — those who are hereditary/dynastic or are part of the local socio- economic/cultural elite — and ‘climbers’, those who have made their way by rising up the ranks. I document three key results: one, barriers to political entry and post-colonial elite persistence have perverse economic consequences. Findings from a close election regression discontinuity design indicate that electing parachuters leads to 0.2 percentage point lower GDP growth per year compared to constituencies where climbers are elected. Two, a leader’s entry route is a sig- nicant feature of political selection, even after controlling for conventional ascriptive identities such as sex, religion and ethnicity. Three, there is suggestive evidence that the impact is driven by misallocation of bureaucratic resources and neither regulation of technology adoption nor factor price manipulation are the underlying mechanisms. Keywords: Political Economy, Political selection, Dynastic politics, Economic Development. JEL codes: D72, O12, N45 ∗George Washington University. Address: Department of Economics, 2115 G St., NW, Monroe 340, Washington, DC 20052; Email: [email protected]. I am indebted to Ashwani Kumar, Sanjay Kabir, Sanjay Paswan, Shaibal Gupta, Srikant and all anonymous respondents for their time and support in completing the data collection for this study. -

Bengal District Gazetteers
BENGAL DISTRICT GAZETTEERS. [ Price *—India, Rt- 3 ; in JSngland, 4*. 6d.~] BENGAL DISTRICT GAZETTEERS. BHAG-ALPXJB- BPATC LIBRARY Accession No. BY Source. Cortf J. b t b n b , IS PUN CIV1J. SERVICE CALCUTTA:. B E N G A L SBCEETAEIAT BOOK DEPOT. p r e f a c e ; ------- ♦------- T h is volume follows the plan of the various volumes of District Gazetteers compiled by Mr. O’Malley. I desire to express my sincere acknowledgments for assistance rendered to me by Messrs. Hammond (r.c.s., Collector of Bhagalpur): and Hubback (i.c.s., Assistant Settlement Officer, Bihar): also to Captain Barnardo, I.M .S ., Civil Surgeon of Bhagalpur, and to Mr. Gr. E. Fawcus of the Indian Educational Service, for the revision of Chapters IV and X III, respectively. Babu Nilmoni Dey, Asisstant Settlement Officer, has also helped me very much.' Eurseong, 1910. J. BYRNE. PLAN OF CONTENTS. C h a t t e r P a g e s . f . P h y sical A s p e c t s ....................................................... 1 — 25 II . H i s t o r y .............................................................................26— 42 IIT . T h e P e o p l e ................................................... 43— &7 IV , P u b l ic H e a l t h ....................................................58— 68 V . A g r i c u l t u r e ....................................................69— 92 V I . N at u r al Ca l a m i t i e s ..........................................93— 108 V IT . R ents, W ages and P rices .... 109— 121 VIII. Occupations, Manufactures and Trade . -

BSDMA DDMA Inception Report
District Disaster Management Plan Banka District, Bihar Inception Report August 2015 Submitted by RMSI A-8, Sector-16 Noida-201301, INDIA Tel: +91-120-251-1102, 2101 Fax: +91-120-251-1109, 0963 www.rmsi.com Contact: Rakesh Ranjan Project Team Leader Email: [email protected] District Disaster Management Plan for Banka District, Bihar For the attention of: The Secretary, Mr. Anuj Tiwari Bihar State Disaster Management Authority Senior Advisor (HRD, CB and Trg) (BSDMA), Bihar State Disaster Management Authority 2nd Floor, Pant Bhawan, Patna (BSDMA), 2nd Floor, Pant Bhawan, Patna Bihar- 800 001 Bihar- 800 001 Email: [email protected] Company Information: Name RMSI Private Limited CIN U74899DL1992PTC047149 Registered Office Address SEATING 3, UNIT NO. 119, FIRST FLOOR, VARDHMAN STAR CITI MALL, SECTOR-7, DWARKA NEW DELHI Delhi-110075 INDIA Corporate Office Address A-8, Sector-16 NOIDA, 201 301 India Tel:+91 120 251 1102, 251 2101 Fax:+91 120 251 1109, 251 0963 E-mail: [email protected] Inception Report Confidential Page 2 of 63 District Disaster Management Plan for Banka District, Bihar Acknowledgements RMSI appreciates the Bihar State Disaster Management Authority (BSDMA), Patna for awarding this contract. We would like to acknowledge the support extended by Mr. Naresh Paswan, Secretary, BSDMA; Mr. Anil Kumar Jha, Under Secretary, BSDMA; Mr. Anuj Tiwari, Senior Advisor, BSDMA; Dr Shankar Dayal, Senior Advisor, BSDMA; Dr. Madhu Bala, Project Officer (Natural Disaster), BSDMA; and District officials of all four districts during the project kick off and inception meetings. Advice and directions provided by Mr. Anuj Tiwari and Dr. Shankar Dayal while drafting this inception report are highly appreciated. -

Mapping of Shgs in Bihar
MMAAPPPPIINNGG OOFF SSEELLFF HHEELLPP GGOOUUPPSS IINN BBIIHHAARR Study conducted by APMAS December 2011 APMAS Plot No. 20, Rao & Raju Colony Road No.2, Banjara Hills Hyderabad- 500 034 2 ACKNOWLEDGEMENTS We are highly indebted to all the Self Help Group Members and leaders of Self Help Group Promoting Institutions / NGOs (SHPI) who have spared their valuable time, extended cooperation in visiting SHGs and shared their experiences with us. They are the purpose of our study and they are the real champions of this movement. At the outset, we are thankful to Ms. Geeta Verma, who initiated this study and provided a great opportunity to APMAS to conduct this study, which has been a great learning for us. She also gave us an understanding of the origin of SHG movement and guided the study all through. Our sincere thanks to Ms. Madhuri, for her valuable inputs in the preparation of study design, finalization of data collection tools and cooperation provided in conducting fieldwork in all the study areas. We are thankful to our APMAS Chairman, Mr. K. Madhava Rao, IAS (Retd.) who has given encouragement in bringing out this report. We are extremely grateful to our CEO, Mr. C.S. Reddy, who has been deeply involved and added value to the study with his rich experience at all stages, since formulation of the research design to finalization of the study report. We are highly thankful to all the DDCs, Project Directors of DRDA, Lead Bank District Managers, DDMs of NABARD, District Project Managers of BRLPS, WDC and Mahila Samakhya who gave us individual interviews in spite of their busy schedule, and in providing secondary data relating to SHGs and federations.