Strategies That Work: NTD Control and Elimination in the Philippines
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Nd Drrm C Upd Date
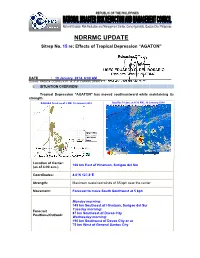
NDRRMC UPDATE Sitrep No. 15 re: Effects of Tropical Depression “AGATON” Releasing Officer: USEC EDUARDO D. DEL ROSARIO Executive Director, NDRRMC DATE : 19 January 2014, 6:00 AM Sources: PAGASA, OCDRCs V,VII, IX, X, XI, CARAGA, DPWH, PCG, MIAA, AFP, PRC, DOH and DSWD I. SITUATION OVERVIEW: Tropical Depression "AGATON" has moved southeastward while maintaining its strength. PAGASA Track as of 2 AM, 19 January 2014 Satellite Picture at 4:32 AM., 19 January 2014 Location of Center: 166 km East of Hinatuan, Surigao del Sur (as of 4:00 a.m.) Coordinates: 8.0°N 127.8°E Strength: Maximum sustained winds of 55 kph near the center Movement: Forecast to move South Southwest at 5 kph Monday morninng: 145 km Southeast of Hinatuan, Surigao del Sur Tuesday morninng: Forecast 87 km Southeast of Davao City Positions/Outlook: Wednesday morning: 190 km Southwest of Davao City or at 75 km West of General Santos City Areas Having Public Storm Warning Signal PSWS # Mindanao Signal No. 1 Surigao del Norte (30-60 kph winds may be expected in at Siargao Is. least 36 hours) Surigao del Sur Dinagat Province Agusan del Norte Agusan del Sur Davao Oriental Compostela Valley Estimated rainfall amount is from 5 - 15 mm per hour (moderate - heavy) within the 300 km diameter of the Tropical Depression Tropical Depression "AGATON" will bring moderate to occasionally heavy rains and thunderstorms over Visayas Sea travel is risky over the seaboards of Luzon and Visayas. The public and the disaster risk reduction and management councils concerned are advised to take appropriate actions II. -

Province, City, Municipality Total and Barangay Population AURORA
2010 Census of Population and Housing Aurora Total Population by Province, City, Municipality and Barangay: as of May 1, 2010 Province, City, Municipality Total and Barangay Population AURORA 201,233 BALER (Capital) 36,010 Barangay I (Pob.) 717 Barangay II (Pob.) 374 Barangay III (Pob.) 434 Barangay IV (Pob.) 389 Barangay V (Pob.) 1,662 Buhangin 5,057 Calabuanan 3,221 Obligacion 1,135 Pingit 4,989 Reserva 4,064 Sabang 4,829 Suclayin 5,923 Zabali 3,216 CASIGURAN 23,865 Barangay 1 (Pob.) 799 Barangay 2 (Pob.) 665 Barangay 3 (Pob.) 257 Barangay 4 (Pob.) 302 Barangay 5 (Pob.) 432 Barangay 6 (Pob.) 310 Barangay 7 (Pob.) 278 Barangay 8 (Pob.) 601 Calabgan 496 Calangcuasan 1,099 Calantas 1,799 Culat 630 Dibet 971 Esperanza 458 Lual 1,482 Marikit 609 Tabas 1,007 Tinib 765 National Statistics Office 1 2010 Census of Population and Housing Aurora Total Population by Province, City, Municipality and Barangay: as of May 1, 2010 Province, City, Municipality Total and Barangay Population Bianuan 3,440 Cozo 1,618 Dibacong 2,374 Ditinagyan 587 Esteves 1,786 San Ildefonso 1,100 DILASAG 15,683 Diagyan 2,537 Dicabasan 677 Dilaguidi 1,015 Dimaseset 1,408 Diniog 2,331 Lawang 379 Maligaya (Pob.) 1,801 Manggitahan 1,760 Masagana (Pob.) 1,822 Ura 712 Esperanza 1,241 DINALUNGAN 10,988 Abuleg 1,190 Zone I (Pob.) 1,866 Zone II (Pob.) 1,653 Nipoo (Bulo) 896 Dibaraybay 1,283 Ditawini 686 Mapalad 812 Paleg 971 Simbahan 1,631 DINGALAN 23,554 Aplaya 1,619 Butas Na Bato 813 Cabog (Matawe) 3,090 Caragsacan 2,729 National Statistics Office 2 2010 Census of Population and -

Philippine Port Authority Contracts Awarded for CY 2018
Philippine Port Authority Contracts Awarded for CY 2018 Head Office Project Contractor Amount of Project Date of NOA Date of Contract Procurement of Security Services for PPA, Port Security Cluster - National Capital Region, Central and Northern Luzon Comprising PPA Head Office, Port Management Offices (PMOs) of NCR- Lockheed Global Security and Investigation Service, Inc. 90,258,364.20 27-Nov-19 23-Dec-19 North, NCR-South, Bataan/Aurora and Northern Luzon and Terminal Management Offices (TMO's) Ports Under their Respective Jurisdiction Proposed Construction and Offshore Installation of Aids to Marine Navigation at Ports of JARZOE Builders, Inc./ DALEBO Construction and General. 328,013,357.76 27-Nov-19 06-Dec-19 Estancia, Iloilo; Culasi, Roxas City; and Dumaguit, New Washington, Aklan Merchandise/JV Proposed Construction and Offshore Installation of Aids to Marine Navigation at Ports of Lipata, Goldridge Construction & Development Corporation / JARZOE 200,000,842.41 27-Nov-19 06-Dec-19 Culasi, Antique; San Jose de Buenavista, Antique and Sibunag, Guimaras Builders, Inc/JV Consultancy Services for the Conduct of Feasibility Studies and Formulation of Master Plans at Science & Vision for Technology, Inc./ Syconsult, INC./JV 26,046,800.00 12-Nov-19 16-Dec-19 Selected Ports Davila Port Development Project, Port of Davila, Davila, Pasuquin, Ilocos Norte RCE Global Construction, Inc. 103,511,759.47 24-Oct-19 09-Dec-19 Procurement of Security Services for PPA, Port Security Cluster - National Capital Region, Central and Northern Luzon Comprising PPA Head Office, Port Management Offices (PMOs) of NCR- Lockheed Global Security and Investigation Service, Inc. 90,258,364.20 23-Dec-19 North, NCR-South, Bataan/Aurora and Northern Luzon and Terminal Management Offices (TMO's) Ports Under their Respective Jurisdiction Rehabilitation of Existing RC Pier, Port of Baybay, Leyte A. -

Eisai Announces Results and Continued Support Of
No.17-18 April 19, 2017 Eisai Co., Ltd. EISAI ANNOUNCES RESULTS AND CONTINUED SUPPORT OF INITIATIVES FOR ELIMINATION OF LYMPHATIC FILARIASIS 5 YEAR ANNIVERSARY OF LONDON DECLARATION ON NEGLECTED TROPICAL DISEASES Eisai Co., Ltd. (Headquarters: Tokyo, CEO: Haruo Naito, “Eisai”) has announced the results of its initiatives for the elimination of lymphatic filariasis (LF), and its continued support of this cause in the future. This announcement was made at an event held in Geneva, Switzerland, on April 18, marking the 5th anniversary of the London Declaration on Neglected Tropical Diseases (NTDs), an international public-private partnership. Announced in January 2012, the London Declaration is the largest public-private partnership in the field of global health, and represents a coordinated effort by global pharmaceutical companies, the Bill & Melinda Gates Foundation, the World Health Organization (WHO), the United States, United Kingdom and NTD-endemic country governments, as well as other partners, to eliminate 10 NTDs by the year 2020. Since the signing of the London Declaration, donations of medical treatments by pharmaceutical companies have increased by 70 percent, and these treatments contribute to the prevention and cure of disease in approximately 1 billion people every year. Under the London Declaration, Eisai signed an agreement with WHO to supply 2.2 billion high-quality diethylcarbamazine (DEC) tablets, which were running in short supply worldwide, at Price Zero (free of charge) by the year 2020. These DEC tablets are manufactured at Eisai’s Vizag Plant in India. As of the end of March 2017, 1 billion tablets have been supplied to 27 endemic countries. -

Pathophysiology and Gastrointestinal Impacts of Parasitic Helminths in Human Being
Research and Reviews on Healthcare: Open Access Journal DOI: 10.32474/RRHOAJ.2020.06.000226 ISSN: 2637-6679 Research Article Pathophysiology and Gastrointestinal Impacts of Parasitic Helminths in Human Being Firew Admasu Hailu1*, Geremew Tafesse1 and Tsion Admasu Hailu2 1Dilla University, College of Natural and Computational Sciences, Department of Biology, Dilla, Ethiopia 2Addis Ababa Medical and Business College, Addis Ababa, Ethiopia *Corresponding author: Firew Admasu Hailu, Dilla University, College of Natural and Computational Sciences, Department of Biology, Dilla, Ethiopia Received: November 05, 2020 Published: November 20, 2020 Abstract Introduction: This study mainly focus on the major pathologic manifestations of human gastrointestinal impacts of parasitic worms. Background: Helminthes and protozoan are human parasites that can infect gastrointestinal tract of humans beings and reside in intestinal wall. Protozoans are one celled microscopic, able to multiply in humans, contributes to their survival, permits serious infections, use one of the four main modes of transmission (direct, fecal-oral, vector-borne, and predator-prey) and also helminthes are necked multicellular organisms, referred as intestinal worms even though not all helminthes reside in intestines. However, in their adult form, helminthes cannot multiply in humans and able to survive in mammalian host for many years due to their ability to manipulate immune response. Objectives: The objectives of this study is to assess the main pathophysiology and gastrointestinal impacts of parasitic worms in human being. Methods: Both primary and secondary data were collected using direct observation, books and articles, and also analyzed quantitativelyResults and and conclusion: qualitatively Parasites following are standard organisms scientific living temporarily methods. in or on other organisms called host like human and other animals. -
CENTRAL VISAYAS Regional Development Investment Program
CENTRAL VISAYAS Regional Development Investment Program 2018-2022 CENTRAL VISAYAS Regional Development Investment Program 2018-2022 ©2018 by the National Economic and Development Authority Region 7 All rights reserved. Any part of this publication may be used and reproduced provided proper acknowledgment is made. Central Visayas Regional Development Investment Program 2018-2022 Published by: National Economic and Development Authority Regional Office 07 Government Center, Sudlon, Lahug, Cebu City, Philippines Tel: (032) 414-5254 / (032) 414-5263 Email: [email protected] RDC 07 Website: www.rdc7.net.ph NEDA Website: www.neda7.ph Contents Page Message RDC Chairman iii Message RDC Vice-Chairman iv Executive Summary 1 Chapter 1 Enhancing the Social Fabric 3 Chapter 2 Inequality-Reducing Transformation 6 Chapter 3 Increasing Growth Potential 53 Chapter 4 Foundations for Sustainable Development 57 List of Tables and Figures Page Tables 1 Summary of Programs, Activities, and Projects by 1 Development Outcome 1 Enhancing the Social Fabric PAPs 5 2 Inequality-Reducing Transformation PAPs 9 3 Increasing Growth Potential PAPs 55 4 Foundations for Sustainable Development PAPs 61 Figures 1 Distribution of the Investment Requirement by 2 Development Outcome 1.1 Annual Investment Requirement (Chapter 1) 3 1.2 Investment Requirement by Agency (Chapter 1) 3 1.3 Investment Requirement by Location (Chapter 1) 4 2.1 Annual Investment Requirement (Chapter 2) 6 2.2 Investment Requirement by Agency (Chapter 2) 7 2.3 Number of PAPs by Location (Chapter 2) 7 2.4 Investment Requirement by Location (Chapter 2) 8 3.1 Annual Investment Requirement (Chapter 3) 53 4.1 Annual Investment Requirement (Chapter 4) 57 4.2 Number of PAPs by Implementing Agency 58 4.3 Investment Requirement by Implementing Agency (Chapter 4) 59 4.4 Investment Requirement by Location (Chapter 4) 59 Executive Summary Background The Central Visayas RDC coordinated the preparation of the Regional Development Investment Program (RDIP). -
LTFRB-MC-2020-051B.Pdf
Republic of the Philippines Department of Transportation LAND TRANSPORTATION FRANCHISING & REGULATORY BOARD East Avenue, Quezon City MEMORANDUM CIRCULAR NO. 2020-051-B SUBJECT : ADDITIONAL ROUTES ALLOWED FOR THE OPERATION OF PROVINCIAL BUSESENTERING METRO MANILA DURING THE PERIOD OF GCQ/MGCQ WHEREAS, pursuant to the guidelines of the Department of Transportation (DOTr) for a calibrated and gradual opening of public transportation in Metro Manila and those in nearby provinces, the Board has since then made the necessary monitoring on the daily operations of the initial routes allowed to operate; WHEREAS, on 25 September 2020, the Board issued Memorandum Circular No. 2020- 051which allowed the resumption of operations of select Provincial Bus routes entering Metro Manila; WHEREAS, under Item IIof MC 2020-051, the Board may issue additional routes to resume operations upon approval and coordination with the concerned Local Government Unit (LGU); WHEREAS, based on the monitoring and coordination with local government units across the country, the concerned LGUs of Ormoc, Palompon, Tacloban, Maasin, Catarman, and Laoang have allowed the resumption of operations of PUBs travelling to and from Metro Manila; NOW THEREFORE, for and in consideration of the foregoing, the Board hereby allows the additional routes (attached as ANNEX “A”) for Provincial Buses to operate to and from Metro Manila starting 02 November 2020or as may be allowed by the Inter-Agency Task Force on Emerging Infectious Diseases (IATF-EIF). The provisions of MC 2020-051 shall be applicable herein. In lieu of the Special Permit, the corresponding QR CODE shall be issued to the operator prior to operation. Said QR Code shall be downloaded at www.ltfrb.gov.ph and which must be printed by the operator (size : 8.5”x 11” short bond paper) and displayed conspicuously by the operator in the front windshield of authorized unit (without affecting view of the driver). -

The Immunology of Filariasis*
Articles in the Update series Les articles de la rubrique give a concise, authoritative, Le point fournissent un and up-to-date survey of the bilan concis et fiable de la present position in the se- situation actuelle dans le a e lected fields, and, over a domaine considere. Des ex- ,,v period of years, will cover / perts couvriront ainsi suc- / many different aspects of cessivement de nombreux the biomedical sciences aspects des sciences bio- e nVlfo l l gZ / / and public health. Most of medicales et de la sante the articles will be writ- publique. La plupart de ces ten, by invitation, by ac- articles auront donc ee knowledged experts on the rediges sur demande par les subject. specialistes les plus autorises. Bulletin of the World Health Organization, 59 (1): 1-8 (1981) The immunology of filariasis* SCIENTIFIC WORKING GROUP ON FILARIASIS1 This report summarizes the available information on the immunology of filariasis, and discusses immunodiagnosis and the immunologicalfactors influencing the host-parasite relationship in lymphaticfilariasis and onchocerciasis. Severalareas that requirefurther research are identifed, particularly concerning the development of new serological techniques, and the fractionation of specific antigens. The problems associated with vaccine development are considered and the importance of finding better animal modelsfor research is stressed. Lymphatic filariasis and onchocerciasis are recognized as important public health problems in many tropical and subtropical areas. However, until recently, little was known about the natural history of filariasis or the immune mechanisms involved. This report summarizes current knowledge on various aspects of the immunology of the disease and outlines areas for future research. -

1 Summary of the Thirteenth Meeting of the ITFDE (II) October 29, 2008
Summary of the Thirteenth Meeting of the ITFDE (II) October 29, 2008 The Thirteenth Meeting of the International Task Force for Disease Eradication (ITFDE) was convened at The Carter Center from 8:30am to 4:00 pm on October 29, 2008. Topics discussed at this meeting were the status of the global campaigns to eliminate lymphatic filariasis (LF) and to eradicate dracunculiasis (Guinea worm disease), an update on efforts to eliminate malaria and LF from the Caribbean island of Hispaniola (Dominican Republic and Haiti), and a report on the First Program Review for Buruli ulcer programs. The Task Force members are Dr. Olusoji Adeyi, The World Bank; Sir George Alleyne, Johns Hopkins University; Dr. Julie Gerberding, Centers for Disease Control and Prevention (CDC); Dr. Donald Hopkins, The Carter Center (Chair); Dr. Adetokunbo Lucas, Harvard University; Professor David Molyneux, Liverpool School of Tropical Medicine (Rtd.); Dr. Mark Rosenberg, Task Force for Child Survival and Development; Dr. Peter Salama, UNICEF; Dr. Lorenzo Savioli, World Health Organization (WHO); Dr. Harrison Spencer, Association of Schools of Public Health; Dr. Dyann Wirth, Harvard School of Public Health, and Dr. Yoichi Yamagata, Japan International Cooperation Agency (JICA). Four of the Task Force members (Hopkins, Adeyi, Lucas, Rosenberg) attended this meeting, and three others were represented by alternates (Dr. Stephen Blount for Gerberding, Dr. Mark Young for Dr. Salama, Dr. Dirk Engels for Savioli). Presenters at this meeting were Dr. Eric Ottesen of the Task Force for Child Survival and Development, Dr. Patrick Lammie of the CDC, Dr. Ernesto Ruiz-Tiben of The Carter Center, Dr. David Joa Espinal of the National Center for Tropical Disease Control (CENCET) in the Dominican Republic, and Dr. -

2. Studies on the Multiplication of Chkunya Virus (CHV), and on Physical and Chemical Structure of Its Virion
71 PAPER IN SCIENTIFIC SESSION GROUP A: Immunology and Viral Diseases 1. Principles and Applications of Fluorescent Antibody Technique in Tropical Medicine Akira Kawamura Department of Immunology, Institute of Medical Science, University of Tokyo, Tokyo, Japan 2. Studies on the Multiplication of Chkunya Virus (CHV), and on Physical and Chemical Structure of its Virion Noboru Higashi,Yasuko Nagatomo, Akira Tamura and Toshio Ametani Virus Institute, Kyoto University, Kyoto, Japan 3. Electronmicroscopic Studies on the Multiplications of Japanese Encephalitis Viurs Noboru Higashi*, Toshiko Ametani*, Yasuko Nagatomo*, Eiichi Fujiwara* and Takashi Tsuruhara** *Virus Institute, Kyoto Uniuersity, Kyoto, Japan and **NIH of Japan , Tokyo, Japan 4. Electromicroscopic Studies on the Multiplication of Dengue Virus Noboru Higashi*, Masao Tokuda*, Toshio Ametani*, Mya-Tu, My My Khin** and Toe Myint** *Virus Institute, Kyoto University, Kyoto, Japan and **Viral Section , Burma Medical Institute, Buruma 72 5. A Plaque Assay of Dengue and Other Arboviruses in Monolayer Cultures of BHK-21 Cells Hideo Aoki Department of Microbiology, School of Medicine Kobe University, Kobe, Japan A cell line of baby hamster kidney (BHK-21, clone 13) was found suitable for titration and multiplication of many kinds of arboviruses, including all types of dengue and related viruses. For instance, dengue (type 1, Hawaiian, Mochizuki ; type 2, New Guinea B ; type 3, H-87 ; type 4, H-241 ; type 5 ? Th-36 ; type 6 ? Th-Sman), JBE Nakayama, JaGar # 01, Gl) and Chikungunya (African) viruses are capable of producing clear plaques in monolayer cultures of the cells under a methyl cellulose overlay medium. By means of this plaque assay system, titration and neutralization of these arboviruses are possible. -
2007 Census of Population
VISAYAS 2007 CENSUS OF POPULATION BY PROVINCE, CITY / MUNICIPALITY AND BARANGAY Republic of the Philippines NATIONAL STATISTICS OFFICE Manila, Philippines TABLE OF CONTENTS P A G E EXPLANATORY NOTE v HIGHLIGHTS xiii Population and Annual Growth Rates for Provinces and Highly Urbanized Cities Based on Censuses 1995, 2000 and 2007 xv REGION/PROVINCE/HIGHLY URBANIZED CITY LUZON 1 - 638 NATIONAL CAPITAL REGION (NCR) CITY OF LAS PIÑAS 1 CITY OF MAKATI 1 CITY OF MALABON 2 CITY OF MANDALUYONG 3 CITY OF MANILA 4 CITY OF MARIKINA 29 CITY OF MUNTINLUPA 30 CITY OF NAVOTAS 30 CITY OF PARAÑAQUE 31 CITY OF PASIG 31 CITY OF SAN JUAN 32 CITY OF VALENZUELA 33 KALOOKAN CITY 34 PASAY CITY 39 PATEROS 45 QUEZON CITY 45 TAGUIG 49 CORDILLERA ADMINISTRATIVE REGION ABRA 51 APAYAO 61 BENGUET 66 IFUGAO 75 KALINGA 81 MOUNTAIN PROVINCE 86 REGION I - ILOCOS REGION ILOCOS NORTE 91 ILOCOS SUR 108 LA UNION 132 PANGASINAN 150 TABLE OF CONTENTS REGION/PROVINCE/HIGHLY URBANIZED CITY P A G E REGION II - CAGAYAN VALLEY BATANES 191 CAGAYAN 193 ISABELA 218 NUEVA VIZCAYA 250 QUIRINO 259 REGION III - CENTRAL LUZON AURORA 263 BATAAN 268 BULACAN 276 NUEVA ECIJA 294 PAMPANGA 320 TARLAC 338 ZAMBALES 354 REGION IVA - CALABARZON BATANGAS 363 CAVITE 395 LAGUNA 420 QUEZON 441 RIZAL 477 REGION IVB - MIMAROPA MARINDUQUE 484 OCCIDENTAL MINDORO 491 ORIENTAL MINDORO 497 PALAWAN 510 ROMBLON 525 REGION V - BICOL ALBAY 533 CAMARINES NORTE 554 CAMARINES SUR 563 CATANDUANES 595 MASBATE 605 SORSOGON 622 VISAYAS 639 - 990 REGION VI - WESTERN VISAYAS AKLAN 639 ii TABLE OF CONTENTS REGION/PROVINCE/HIGHLY -
List of Ecpay Cash-In Or Loading Outlets and Branches
LIST OF ECPAY CASH-IN OR LOADING OUTLETS AND BRANCHES # Account Name Branch Name Branch Address 1 ECPAY-IBM PLAZA ECPAY- IBM PLAZA 11TH FLOOR IBM PLAZA EASTWOOD QC 2 TRAVELTIME TRAVEL & TOURS TRAVELTIME #812 EMERALD TOWER JP RIZAL COR. P.TUAZON PROJECT 4 QC 3 ABONIFACIO BUSINESS CENTER A Bonifacio Stopover LOT 1-BLK 61 A. BONIFACIO AVENUE AFP OFFICERS VILLAGE PHASE4, FORT BONIFACIO TAGUIG 4 TIWALA SA PADALA TSP_HEAD OFFICE 170 SALCEDO ST. LEGASPI VILLAGE MAKATI 5 TIWALA SA PADALA TSP_BF HOMES 43 PRESIDENTS AVE. BF HOMES, PARANAQUE CITY 6 TIWALA SA PADALA TSP_BETTER LIVING 82 BETTERLIVING SUBD.PARANAQUE CITY 7 TIWALA SA PADALA TSP_COUNTRYSIDE 19 COUNTRYSIDE AVE., STA. LUCIA PASIG CITY 8 TIWALA SA PADALA TSP_GUADALUPE NUEVO TANHOCK BUILDING COR. EDSA GUADALUPE MAKATI CITY 9 TIWALA SA PADALA TSP_HERRAN 111 P. GIL STREET, PACO MANILA 10 TIWALA SA PADALA TSP_JUNCTION STAR VALLEY PLAZA MALL JUNCTION, CAINTA RIZAL 11 TIWALA SA PADALA TSP_RETIRO 27 N.S. AMORANTO ST. RETIRO QUEZON CITY 12 TIWALA SA PADALA TSP_SUMULONG 24 SUMULONG HI-WAY, STO. NINO MARIKINA CITY 13 TIWALA SA PADALA TSP 10TH 245- B 1TH AVE. BRGY.6 ZONE 6, CALOOCAN CITY 14 TIWALA SA PADALA TSP B. BARRIO 35 MALOLOS AVE, B. BARRIO CALOOCAN CITY 15 TIWALA SA PADALA TSP BUSTILLOS TIWALA SA PADALA L2522- 28 ROAD 216, EARNSHAW BUSTILLOS MANILA 16 TIWALA SA PADALA TSP CALOOCAN 43 A. MABINI ST. CALOOCAN CITY 17 TIWALA SA PADALA TSP CONCEPCION 19 BAYAN-BAYANAN AVE. CONCEPCION, MARIKINA CITY 18 TIWALA SA PADALA TSP JP RIZAL 529 OLYMPIA ST. JP RIZAL QUEZON CITY 19 TIWALA SA PADALA TSP LALOMA 67 CALAVITE ST.