From Electronic Health Records to Digital Health Biographies Robert F
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Artificial Intelligence in Health Care: the Hope, the Hype, the Promise, the Peril
Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril Michael Matheny, Sonoo Thadaney Israni, Mahnoor Ahmed, and Danielle Whicher, Editors WASHINGTON, DC NAM.EDU PREPUBLICATION COPY - Uncorrected Proofs NATIONAL ACADEMY OF MEDICINE • 500 Fifth Street, NW • WASHINGTON, DC 20001 NOTICE: This publication has undergone peer review according to procedures established by the National Academy of Medicine (NAM). Publication by the NAM worthy of public attention, but does not constitute endorsement of conclusions and recommendationssignifies that it is the by productthe NAM. of The a carefully views presented considered in processthis publication and is a contributionare those of individual contributors and do not represent formal consensus positions of the authors’ organizations; the NAM; or the National Academies of Sciences, Engineering, and Medicine. Library of Congress Cataloging-in-Publication Data to Come Copyright 2019 by the National Academy of Sciences. All rights reserved. Printed in the United States of America. Suggested citation: Matheny, M., S. Thadaney Israni, M. Ahmed, and D. Whicher, Editors. 2019. Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril. NAM Special Publication. Washington, DC: National Academy of Medicine. PREPUBLICATION COPY - Uncorrected Proofs “Knowing is not enough; we must apply. Willing is not enough; we must do.” --GOETHE PREPUBLICATION COPY - Uncorrected Proofs ABOUT THE NATIONAL ACADEMY OF MEDICINE The National Academy of Medicine is one of three Academies constituting the Nation- al Academies of Sciences, Engineering, and Medicine (the National Academies). The Na- tional Academies provide independent, objective analysis and advice to the nation and conduct other activities to solve complex problems and inform public policy decisions. -

DOCUMENT RESUME AUTHOR Webnet 96 Conference Proceedings
DOCUMENT RESUME ED 427 649 IR 019 168 AUTHOR Maurer, Hermann, Ed. TITLE WebNet 96 Conference Proceedings (San Francisco, California, October 15-19, 1996). INSTITUTION Association for the Advancement of Computing in Education, Charlottesville, VA. PUB DATE 1996-10-00 NOTE 930p.; For selected individual papers, see IR 019 169-198. Many figures and tables are illegible. AVAILABLE FROM Web site: http://aace.virginia.edu/aace/conf/webnet/proc96.html; also archived on WebNet 98 CD-ROM (includes 1996, 1997, 1998) AACE Membership/CD orders, P.O. Box 2966, Charlottesville, VA 22902; Fax: 804-978-7449 ($35, AACE members, $40, nonmembers). PUB TYPE Collected Works Proceedings (021) EDRS PRICE MF06/PC38 Plus Postage. DESCRIPTORS Access to Information; Authoring Aids (Programming); Computer Science; Computer Software; Courseware; Databases; Distance Education; Educational Media; Educational Strategies; *Educational Technology; Electronic Libraries; Elementary Secondary Education; *Hypermedia; Information Technology; Instructional Design; Multimedia Materials; Postsecondary Education; *World Wide Web IDENTIFIERS Electronic Commerce; Software Tools; Virtual Classrooms; *Web Sites ABSTRACT This proceedings contains 80 full papers, 12 posters/demonstrations, 108 short papers, one panel, and one tutorial, all focusing on World Wide Web applications. Topics include: designing hypertext navigation tools; Web site design; distance education via the Web; instructional design; the world-wide market and censorshipon the Web; customer support via the Web; VRML; -

Regulating Search Engines: Taking Stock and Looking Ahead
GASSER: REGULATING SEARCH ENGINES REGULATING SEARCH ENGINES: TAKING STOCK AND LOOKING AHEAD "To exist is to be indexed by a search engine" (Introna & Nissenbaum) URS GASSER TABLE OF CONTENTS I. IN TR O D UCTIO N ....................................................................................... 202 II. A BRIEF (AND CASUAL) HISTORY OF SEARCH ENGINES ..................... 203 Il. SEARCH ENGINE REGULATION: PAST AND PRESENT ........................ 208 A. OVERVIEW OF SEARCH ENGINE-RELATED CASES ............................ 208 B. LEGISLATION AND REGULATION ................................................. 216 C . SU M M AR Y .......................................................................................... 2 19 III. POSSIBLE FUTURE: HETEROGENEOUS POLICY DEBATES AND THE NEED FOR A NORMATIVE FRAMEWORK ......................................... 220 A. THEMES OF FUTURE POLICY DEBATES ............................................. 220 B . C HALLENGES A HEAD ........................................................................ 224 C. NORMATIVE FOUNDATIONS .............................................................. 227 IV . C ON CLU SIO N ....................................................................................... 234 * Associate Professor of Law, S.J.D. (St. Gallen), J.D. (St. Gallen), LL.M. (Harvard), Attorney at Law, Director, Research Center for Information Law, Univ. of St. Gallen, Faculty Fellow, Berkman Center for Internet & Society, Harvard Law School. I owe special thanks to my colleague James Thurman and the -

Digital Health in a Broadband Land: the Role of Digital Health Literacy Within Rural Environments Wuyou Sui1*, Danica Facca2
Health Science Inquiry Volume 11 | 2020 Digital health in a broadband land: The role of digital health literacy within rural environments Wuyou Sui1*, Danica Facca2 1Department of Kinesiology, Western University, London, ON, Canada 2Faculty of Information and Media Sciences, Western University, London, ON, Canada *Author for correspondence ([email protected]) Abstract: The rapid rise and widespread integration of digital technologies (e.g., smartphones, personal computers) into the fabric of our society has birthed a modern means of delivering healthcare, known as digital health. Through leveraging the accessibility and ubiquity of digital technologies, digital health represents an unprecedented level of reach, impact, and scalability for health- care interventions, known as digital behaviour change interventions (DBCIs). The potential benefits associated with employing DBCIs are of particular interest for populations that are disadvantaged to receiving traditional healthcare, such as rural popu- lations. However, several factors should be considered before implementing a DBCI into a rural environment, notably, digital health literacy. Digital health literacy describes the skills necessary to successful navigate and utilize a digital health solution (e.g., DBCI). Given their limited access to high-speed internet, higher cost associated for similar services, and poorer development of information and communication technologies (ICTs), most rural populations likely report lower digital health literacy – specif- ically, computer literacy, the ability to utilize and leverage digital technologies to solve problems. Hence, DBCIs should address this ‘digital divide’ between urban and rural populations before implementation. Practical solutions could include evaluating rural communities’ access to ICTs, needs assessments with rural community members, as well as integrating rural community stakeholders into the design of digital literacy education and interventions. -

Cybersecurity and the Digital-Health: the Challenge of This Millennium
healthcare Editorial Cybersecurity and the Digital-Health: The Challenge of This Millennium Daniele Giansanti Centre Tisp, Istituto Superiore di Sanità, Via Regina Elena 299, 00161 Roma, Italy; [email protected]; Tel.: +39-06-4990-2701 1. Cybersecurity The problem of computer security is as old as computers themselves and dates back decades. The transition from: (a) a single-user to multi-user assignment to the resource and (b) access to the computer resource of the standalone type to one of the types distributed through a network made it necessary to start talking about computer security. All network architectures, from peer to peer to client-server type, are subject to IT security problems. The term Cybersecurity has recently been introduced to indicate the set of procedures and methodologies used to defend computers, servers, mobile devices, electronic systems, networks and data from malicious attacks. Cybersecurity [1–3] is therefore applied to various contexts, from the economic one to that relating to mobile technologies and includes various actions: • Network security: the procedures for using the network safely; • Application Security: the procedures and solutions for using applications safely; • Information security: the management of information in a secure way and in a privacy- sensitive manner in accordance with pre-established regulations; • Operational security: the security in IT operations, such as, for example, in bank- type transactions; • Disaster recovery and operational continuity: the procedures for restarting after problems Citation: Giansanti, D. Cybersecurity that have affected the regular/routine operation of a system and to ensure operational and the Digital-Health: The Challenge continuity. For example, using informatic solutions such as an efficient disk mirroring of This Millennium. -

Search Engines : Tools for Exploring the Internet
CALIBER-98. 4-5 March 1998. Bhubaneswar. pp.193-199 @ 1NFLIBNET Centre. Ahmedabad Search Engines : Tools For Exploring The Internet SWAPAN KUMAR DASGUPTA Central Library, Kalyani University, Klyuniv @giasclOl. vsnl.net.in Abstract A software package for searching a particular information or topic from the vast amount of information available in INTERNET is called a search engine. The common search engines are Altavista. Webcrawler, Yahoo, Lycos, Infoseek, Aliweb. The author provides a list of search engines in INTERNET covering wide areas of interest and then brief description of URLs. After mentioning about the role of the INFLIBNET in modemising the university libraries and in improving the on-line access by creating its web page, the author says that in order to improve upon the education and research infrastructure of the country. some changes are necessary in our present thinking and approach. Introdution Internet is a global mesh and may be called a large repository of information put up by the user. Searching in a particular information or topic of interest, is an intricate task due to the fabulous size of Internet, and vast amount of information, and its many possible methods of storage. A software package for this purpose is called a search engine. Common Search Engines The common WWW search engines are Altavista, Webcrawler, Yahoo, Lycos, Infoseek, Aliweb. Some of these sites may be very busy, then the user has to try for another site, or may press G key for going to another URL. People are not aware that, netsurf can be of various ways. They may say it seems to be time consuming, but the fact is it is free from traditional constraints of time and space. -

Digital Health and the Global Pandemic | 1
Introduction As the world grapples with the tragic COVID-19 pandemic, it is tempting to imagine a post-COVID future that includes some silver linings. As terrible as the situation is today, this calamity will lead to some lasting, positive changes, particularly in healthcare. Virtual Care (often referred to in common parlance as simply telemedicine, and we will use them interchangeably here) has emerged as the poster child for this line of thinking. Providers and patients have dramatically increased the use of telemedicine to ensure continued access to quality healthcare services while maintaining social distance and modulating the enormous burden on our healthcare workers and facilities. Regulators and payers are encouraging and enabling this shift by temporarily relaxing policies that have historically limited telemedicine. Adjacent areas of digital health including digital therapeutics, digital disease management, and remote monitoring have followed suit, finding similarly relaxed policies, more accessible reimbursement, and increased adoption by providers and patients alike. Many have questioned whether these changes will endure as life returns to a “new normal”, or if policies will be reverted and accelerated growth will subside. We begin by examining the potential for COVID-19 to drive lasting change for various categories of digital health technologies. Given the large scale of virtual care, in combination with its potential for lasting COVID-19 impact, we then will dive deeply into this category as a leading indicator of other areas of digital health. Because the US experience has been so widely covered (and to some degree it is still playing out in real time) we highlight key characteristics and trends across Asia Pacific (APAC) and European markets. -

United States Patent (19) 11 Patent Number: 6,094,649 Bowen Et Al
US006094649A United States Patent (19) 11 Patent Number: 6,094,649 Bowen et al. (45) Date of Patent: Jul. 25, 2000 54) KEYWORD SEARCHES OF STRUCTURED “Charles Schwab Broadens Deployment of Fulcrum-Based DATABASES Corporate Knowledge Library Application', Uknown, Full 75 Inventors: Stephen J Bowen, Sandy; Don R crum Technologies Inc., Mar. 3, 1997, pp. 1-3. Brown, Salt Lake City, both of Utah (List continued on next page.) 73 Assignee: PartNet, Inc., Salt Lake City, Utah 21 Appl. No.: 08/995,700 Primary Examiner-Hosain T. Alam 22 Filed: Dec. 22, 1997 Assistant Examiner Thuy Pardo Attorney, Agent, or Firm-Computer Law---- (51) Int. Cl." ...................................................... G06F 17/30 52 U.S. Cl. ......................................... 707/3; 707/5; 707/4 (57 ABSTRACT 58 Field of Search .................................... 707/1, 2, 3, 4, 707/5, 531, 532,500 Methods and Systems are provided for Supporting keyword Searches of data items in a structured database, Such as a 56) References Cited relational database. Selected data items are retrieved using U.S. PATENT DOCUMENTS an SQL query or other mechanism. The retrieved data values 5,375,235 12/1994 Berry et al. ................................. is are documented using a markup language such as HTML. 5,469,354 11/1995 Hatakeyama et al. ... 707/3 The documents are indexed using a web crawler or other 5,546,578 8/1996 Takada ................. ... 707/5 indexing agent. Data items may be Selected for indexing by 5,685,003 11/1997 Peltonen et al. .. ... 707/531 5,787.295 7/1998 Nakao ........... ... 707/500 identifying them in a data dictionary. The indexing agent 5,787,421 7/1998 Nomiyama .. -
Best Practices of Cybersecurity in the Healthcare Industries
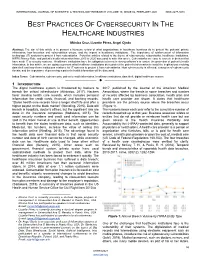
INTERNATIONAL JOURNAL OF SCIENTIFIC & TECHNOLOGY RESEARCH VO`LUME 10, ISSUE 02, FEBRUARY 2021 ISSN 2277-8616 BEST PRACTICES OF CYBERSECURITY IN THE HEALTHCARE INDUSTRIES Mónica Cruz, Lizzette Pérez, Angel Ojeda Abstract: The aim of this article is to present a literature review of what organizations in healthcare business do to protect the patients‘ private information, how breaches and vulnerabilities occurs, and the impact in healthcare institutions. The importance of reinforcement of information technology (IT) systems to protect it from cyberattacks. Forty-five articles related to the theme of cybersecurity, cyberattacks, healthcare institutions, HIPPA Privacy Rule, and patient‘s health information from 2015 to 2020 was used to write this article. Cyberattacks are easy to execute in devices that have weak IT or security systems. Healthcare institutions have the obligation to invest in strong software‘s to ensure the protection of patient‘s health information. In this article, we are going to present what healthcare institutions do to protect the patient's information to avoid the implications involving data theft and how these institutions reinforce its‘ IT systems to protect it from cyberattacks. How cybersecurity is affected, examples of cybersecurity threats, and the importance of preserving a patient‘s health information will be discussed. Index Terms: Cyberattacks, cybersecurity, patient‘s health information, healthcare institutions, data theft, digital healthcare system —————————— —————————— 1 INTRODUCTION The digital healthcare system is threatened by hackers to 2017, published by the Journal of the American Medical breach the critical infrastructure (Athinaiou, 2017). Hackers Association, where the trends in some breaches and number favor stealing health care records, which includes personal of records affected by business association, health plan and information like credit cards, financial, and banking records. -

Be He@Lthy, Be Mobile – 2018 Annual Report
BE HE@LTHY, BE MOBILE Annual Report 2018 Be He@lthy, Be Mobile Annual Report 2018 ISBN: 978-92-4-151625-9 WHO ISBN: 978-92-61-29451-9 ITU ISBN: 978-92-61-29461-8 ITU (PDF) Some rights reserved. This work is available under the Creative Commons Attribution- NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons. org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO or ITU endorses any specific organization, products or services. The unauthorized use of the WHO or ITU names or logos is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO) or the International Telecommunication Union (ITU). Neither WHO nor ITU are responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization (http://www.wipo.int/ amc/en/mediation/rules). Suggested citation. Be He@lthy, Be Mobile Annual Report 2018. Geneva: World Health Organization and International Telecommunication Union, 2019. -

Electronic Health Records in India
CSD Working Paper Series: Towards a New Indian Model of Information and Communications Technology-Led Growth and Development Electronic Health Records in India ICT India Working Paper #25 Manisha Wadhwa March 2020 CSD Working Paper Series: Towards a New Indian Model of Information and Communications Technology-Led Growth and Development Table of Contents Abbreviations ................................................................................................................................................ 4 Abstract ......................................................................................................................................................... 5 Introduction .................................................................................................................................................. 6 Benefits of EHR ............................................................................................................................................. 8 Initiatives by the Government of India ......................................................................................................... 8 EHR Standards ........................................................................................................................................... 8 Goals of EHR Standards ......................................................................................................................... 9 Need for EHR Standards ....................................................................................................................... -
Digital Health & AI
The Digital Health and AI Program The creation of large volumes of complex healthcare data means that artificial intelligence (AI) will increasingly be applied within every aspect of the field. AI algorithms are already being utilized by a number of healthcare organizations for diagnosis and treatment recommendations, patient engagement and adherence, and administrative activities. Our vision at the Ottawa DOM-NFP is to build AI healthcare applications to accelerate the prevention, diagnosis and treatment of diseases, and provide universal access to medical expertise and care. To achieve this vision, we have assembled a multidisciplinary team of experts from diverse fields and we are building strategic partnerships with world-leading AI organizations. As part of our effort to build world class partnerships with leading organizations in the field of AI, we reached out to Microsoft to explore opportunities to work together. Microsoft has shown great interest in our work and have agreed to build long-term collaboration to support our Digital Health and AI Program. Additionally, Microsoft offered the Ottawa DOM-NFP an Azure grant. We are in discussion with other world leading organizations and will continue building such strategic collaborations in the future. Our goal is to provide medical researchers with a springboard to accelerate knowledge implementation by helping them translate their research into AI powered healthcare applications. We are creating in-house resources for technology development, market research, knowledge translation and business strategy, and building strategic partnerships with external organizations, healthcare investors and public sector funders. We envision that the digital health applications developed through such multi- functional collaborations will empower physicians, patients and other care professionals to make informed decisions quicker and more accurately than ever before.