Be He@Lthy, Be Mobile – 2018 Annual Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Artificial Intelligence in Health Care: the Hope, the Hype, the Promise, the Peril
Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril Michael Matheny, Sonoo Thadaney Israni, Mahnoor Ahmed, and Danielle Whicher, Editors WASHINGTON, DC NAM.EDU PREPUBLICATION COPY - Uncorrected Proofs NATIONAL ACADEMY OF MEDICINE • 500 Fifth Street, NW • WASHINGTON, DC 20001 NOTICE: This publication has undergone peer review according to procedures established by the National Academy of Medicine (NAM). Publication by the NAM worthy of public attention, but does not constitute endorsement of conclusions and recommendationssignifies that it is the by productthe NAM. of The a carefully views presented considered in processthis publication and is a contributionare those of individual contributors and do not represent formal consensus positions of the authors’ organizations; the NAM; or the National Academies of Sciences, Engineering, and Medicine. Library of Congress Cataloging-in-Publication Data to Come Copyright 2019 by the National Academy of Sciences. All rights reserved. Printed in the United States of America. Suggested citation: Matheny, M., S. Thadaney Israni, M. Ahmed, and D. Whicher, Editors. 2019. Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril. NAM Special Publication. Washington, DC: National Academy of Medicine. PREPUBLICATION COPY - Uncorrected Proofs “Knowing is not enough; we must apply. Willing is not enough; we must do.” --GOETHE PREPUBLICATION COPY - Uncorrected Proofs ABOUT THE NATIONAL ACADEMY OF MEDICINE The National Academy of Medicine is one of three Academies constituting the Nation- al Academies of Sciences, Engineering, and Medicine (the National Academies). The Na- tional Academies provide independent, objective analysis and advice to the nation and conduct other activities to solve complex problems and inform public policy decisions. -

Digital Health in a Broadband Land: the Role of Digital Health Literacy Within Rural Environments Wuyou Sui1*, Danica Facca2
Health Science Inquiry Volume 11 | 2020 Digital health in a broadband land: The role of digital health literacy within rural environments Wuyou Sui1*, Danica Facca2 1Department of Kinesiology, Western University, London, ON, Canada 2Faculty of Information and Media Sciences, Western University, London, ON, Canada *Author for correspondence ([email protected]) Abstract: The rapid rise and widespread integration of digital technologies (e.g., smartphones, personal computers) into the fabric of our society has birthed a modern means of delivering healthcare, known as digital health. Through leveraging the accessibility and ubiquity of digital technologies, digital health represents an unprecedented level of reach, impact, and scalability for health- care interventions, known as digital behaviour change interventions (DBCIs). The potential benefits associated with employing DBCIs are of particular interest for populations that are disadvantaged to receiving traditional healthcare, such as rural popu- lations. However, several factors should be considered before implementing a DBCI into a rural environment, notably, digital health literacy. Digital health literacy describes the skills necessary to successful navigate and utilize a digital health solution (e.g., DBCI). Given their limited access to high-speed internet, higher cost associated for similar services, and poorer development of information and communication technologies (ICTs), most rural populations likely report lower digital health literacy – specif- ically, computer literacy, the ability to utilize and leverage digital technologies to solve problems. Hence, DBCIs should address this ‘digital divide’ between urban and rural populations before implementation. Practical solutions could include evaluating rural communities’ access to ICTs, needs assessments with rural community members, as well as integrating rural community stakeholders into the design of digital literacy education and interventions. -

Cybersecurity and the Digital-Health: the Challenge of This Millennium
healthcare Editorial Cybersecurity and the Digital-Health: The Challenge of This Millennium Daniele Giansanti Centre Tisp, Istituto Superiore di Sanità, Via Regina Elena 299, 00161 Roma, Italy; [email protected]; Tel.: +39-06-4990-2701 1. Cybersecurity The problem of computer security is as old as computers themselves and dates back decades. The transition from: (a) a single-user to multi-user assignment to the resource and (b) access to the computer resource of the standalone type to one of the types distributed through a network made it necessary to start talking about computer security. All network architectures, from peer to peer to client-server type, are subject to IT security problems. The term Cybersecurity has recently been introduced to indicate the set of procedures and methodologies used to defend computers, servers, mobile devices, electronic systems, networks and data from malicious attacks. Cybersecurity [1–3] is therefore applied to various contexts, from the economic one to that relating to mobile technologies and includes various actions: • Network security: the procedures for using the network safely; • Application Security: the procedures and solutions for using applications safely; • Information security: the management of information in a secure way and in a privacy- sensitive manner in accordance with pre-established regulations; • Operational security: the security in IT operations, such as, for example, in bank- type transactions; • Disaster recovery and operational continuity: the procedures for restarting after problems Citation: Giansanti, D. Cybersecurity that have affected the regular/routine operation of a system and to ensure operational and the Digital-Health: The Challenge continuity. For example, using informatic solutions such as an efficient disk mirroring of This Millennium. -

Digital Health and the Global Pandemic | 1
Introduction As the world grapples with the tragic COVID-19 pandemic, it is tempting to imagine a post-COVID future that includes some silver linings. As terrible as the situation is today, this calamity will lead to some lasting, positive changes, particularly in healthcare. Virtual Care (often referred to in common parlance as simply telemedicine, and we will use them interchangeably here) has emerged as the poster child for this line of thinking. Providers and patients have dramatically increased the use of telemedicine to ensure continued access to quality healthcare services while maintaining social distance and modulating the enormous burden on our healthcare workers and facilities. Regulators and payers are encouraging and enabling this shift by temporarily relaxing policies that have historically limited telemedicine. Adjacent areas of digital health including digital therapeutics, digital disease management, and remote monitoring have followed suit, finding similarly relaxed policies, more accessible reimbursement, and increased adoption by providers and patients alike. Many have questioned whether these changes will endure as life returns to a “new normal”, or if policies will be reverted and accelerated growth will subside. We begin by examining the potential for COVID-19 to drive lasting change for various categories of digital health technologies. Given the large scale of virtual care, in combination with its potential for lasting COVID-19 impact, we then will dive deeply into this category as a leading indicator of other areas of digital health. Because the US experience has been so widely covered (and to some degree it is still playing out in real time) we highlight key characteristics and trends across Asia Pacific (APAC) and European markets. -
Best Practices of Cybersecurity in the Healthcare Industries
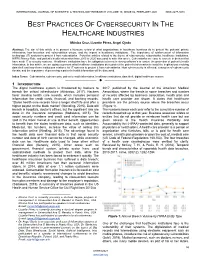
INTERNATIONAL JOURNAL OF SCIENTIFIC & TECHNOLOGY RESEARCH VO`LUME 10, ISSUE 02, FEBRUARY 2021 ISSN 2277-8616 BEST PRACTICES OF CYBERSECURITY IN THE HEALTHCARE INDUSTRIES Mónica Cruz, Lizzette Pérez, Angel Ojeda Abstract: The aim of this article is to present a literature review of what organizations in healthcare business do to protect the patients‘ private information, how breaches and vulnerabilities occurs, and the impact in healthcare institutions. The importance of reinforcement of information technology (IT) systems to protect it from cyberattacks. Forty-five articles related to the theme of cybersecurity, cyberattacks, healthcare institutions, HIPPA Privacy Rule, and patient‘s health information from 2015 to 2020 was used to write this article. Cyberattacks are easy to execute in devices that have weak IT or security systems. Healthcare institutions have the obligation to invest in strong software‘s to ensure the protection of patient‘s health information. In this article, we are going to present what healthcare institutions do to protect the patient's information to avoid the implications involving data theft and how these institutions reinforce its‘ IT systems to protect it from cyberattacks. How cybersecurity is affected, examples of cybersecurity threats, and the importance of preserving a patient‘s health information will be discussed. Index Terms: Cyberattacks, cybersecurity, patient‘s health information, healthcare institutions, data theft, digital healthcare system —————————— —————————— 1 INTRODUCTION The digital healthcare system is threatened by hackers to 2017, published by the Journal of the American Medical breach the critical infrastructure (Athinaiou, 2017). Hackers Association, where the trends in some breaches and number favor stealing health care records, which includes personal of records affected by business association, health plan and information like credit cards, financial, and banking records. -

Electronic Health Records in India
CSD Working Paper Series: Towards a New Indian Model of Information and Communications Technology-Led Growth and Development Electronic Health Records in India ICT India Working Paper #25 Manisha Wadhwa March 2020 CSD Working Paper Series: Towards a New Indian Model of Information and Communications Technology-Led Growth and Development Table of Contents Abbreviations ................................................................................................................................................ 4 Abstract ......................................................................................................................................................... 5 Introduction .................................................................................................................................................. 6 Benefits of EHR ............................................................................................................................................. 8 Initiatives by the Government of India ......................................................................................................... 8 EHR Standards ........................................................................................................................................... 8 Goals of EHR Standards ......................................................................................................................... 9 Need for EHR Standards ....................................................................................................................... -
Digital Health & AI
The Digital Health and AI Program The creation of large volumes of complex healthcare data means that artificial intelligence (AI) will increasingly be applied within every aspect of the field. AI algorithms are already being utilized by a number of healthcare organizations for diagnosis and treatment recommendations, patient engagement and adherence, and administrative activities. Our vision at the Ottawa DOM-NFP is to build AI healthcare applications to accelerate the prevention, diagnosis and treatment of diseases, and provide universal access to medical expertise and care. To achieve this vision, we have assembled a multidisciplinary team of experts from diverse fields and we are building strategic partnerships with world-leading AI organizations. As part of our effort to build world class partnerships with leading organizations in the field of AI, we reached out to Microsoft to explore opportunities to work together. Microsoft has shown great interest in our work and have agreed to build long-term collaboration to support our Digital Health and AI Program. Additionally, Microsoft offered the Ottawa DOM-NFP an Azure grant. We are in discussion with other world leading organizations and will continue building such strategic collaborations in the future. Our goal is to provide medical researchers with a springboard to accelerate knowledge implementation by helping them translate their research into AI powered healthcare applications. We are creating in-house resources for technology development, market research, knowledge translation and business strategy, and building strategic partnerships with external organizations, healthcare investors and public sector funders. We envision that the digital health applications developed through such multi- functional collaborations will empower physicians, patients and other care professionals to make informed decisions quicker and more accurately than ever before. -
A Framework for Selecting Digital Health Technology
INNOVATION REPORT A Framework for Selecting Digital Health Technology AN IHI RESOURCE 20 University Road, Cambridge, MA 02138 • ihi.org How to Cite This Paper: Ostrovsky A, Deen N, Simon A, Mate K. A Framework for Selecting Digital Health Technology. IHI Innovation Report. Cambridge, MA: Institute for Healthcare Improvement; June 2014. (Available at www.ihi.org). AUTHORS: Andrey Ostrovsky, MD: Pediatric Resident, Children’s Hospital Boston and Boston Medical Center; and Co-founder and CEO, Care at Hand Nigel Deen: Research Assistant, IHI Adam Simon, PhD: President and CEO, Cerora, Inc. Kedar Mate, MD: Senior Vice President, IHI This IHI Innovation Project was conducted in Summer 2013. The Institute for Healthcare Improvement (IHI) is a leading innovator in health and health care improvement worldwide. IHI’s approach to innovation is built on two major concepts: 1) innovation is needed when people, organizations, or systems, seek to move beyond incremental improvement to achieve new levels of performance; and 2) innovation is the bridge between invention and implementation. Innovation, for us, is the key to getting promising inventions executed and adopted across all settings. IHI’s innovation process seeks to research innovative ideas, assess their potential for advancing quality improvement, and bring them to action. The process includes time-bound learning cycles (30, 60, or 90 days) to scan for innovative practices, test theories and new models, and synthesize the findings (in the form of the summary Innovation Report). Learn more about IHI’s innovation process on our website. Copyright © 2014 Institute for Healthcare Improvement All rights reserved. Individuals may photocopy these materials for educational, not-for-profit uses, provided that the contents are not altered in any way and that proper attribution is given to IHI as the source of the content. -
Digital Health Ecosystem for African Countries File Type
Digital Health Ecosystem for African countries A Guide for Public and Private Actors for establishing holistic Digital Health Ecosystems in Africa LIST OF ABBREVIATIONS ACBF African Capacity Building Foundation ICD International Statisticall Classification of Diseases and Related Health Problems API Application Programming Interface ICT Information and Communications BMZ Federal Ministry for Economic Cooperation Technology and Development IHE Healthcare Enterprise CDA Clinical Document Architecture IVD Ischemic Vascular Disease CDA Common Document Architecture KPI Key Performance Indicators CDR Clinical Data Repository mHealth Mobile Health Applications CDW Clinical Data Warehouse MPI Master Patient Index CODL Centre for Open and Distance Learning MRS Medical Record System DATIM Data for Accountability Transparency Impact Monitoring NGO Non-Governmental Organization EAIDSNet East African Integrated Disease NHSSP II National Heath Sector Strategic Plan II Surveillance Network openEHR Open Electronic Health Record ECS Emergency Care Summary PaaS Platform as a Servcie eHR Electronic Health Record PEPFAR President's Emergency Plan for AIDS Relief eID Electronic Identification PHCIS Primary Health Care Information System eIDSR Electronic Integrated Disease Surveillance REC Regional Economic Communities and Response RRI eHealth Regulation Readiness Index EMR Electronic Medical Record System SaaS Software as a Service ePS Electronic Patient Summary SACIDS Southern Africa Centre for Infectious Disease ESA European Space Agency Surveillance ESB -

How to Value Digital Health Interventions? a Systematic Literature Review
International Journal of Environmental Research and Public Health Review How to Value Digital Health Interventions? A Systematic Literature Review Katarzyna Kolasa * and Grzegorz Kozinski Division of Health Economics and Health Care Management, Kozminski University, 03-301 Warsaw, Poland; [email protected] * Correspondence: [email protected] Received: 27 January 2020; Accepted: 13 March 2020; Published: 23 March 2020 Abstract: In Europe, there were almost twice as many patents granted for medical technology (13,795) compared to pharmaceuticals (7441) in 2018. It is important to ask how to integrate such an amount of innovations into routine clinical practice and how to measure the value it brings to the healthcare system. Given the novelty of digital health interventions (DHI), one can even question whether the quality-adjusted life years (QALY) approach developed for pharmaceuticals can be used or whether we need to develop a new DHI’s value assessment framework. We conducted a systematic literature review of published DHIs’ assessment guidelines. Each publication was analyzed with a 12-items checklist based on a EUnetHTA core model enriched with additional criteria such as usability, interoperability, and data security. In total, 11 value assessment guidelines were identified. The review revealed that safety, clinical effectiveness, usability, economic aspects, and interoperability were most often discussed (seven out of 11). More than half of the guidelines addressed organizational impact, data security, choice of comparator, and technical considerations (six out of 11). The unmet medical needs (three out of 11), along with the ethical (two out of 11) and legal aspects (one out of 11), were given the least attention. -

Draft Global Strategy on Digital Health 2020–2024
Draft global strategy on digital health 2020–2024 GLOBAL STRATEGY ON DIGITAL HEALTH Draft 12 December 2019 _______________________________________________________________________________________________ Table of Contents digital technologies: shaping the future of global health ..................................................................... 3 PURPOSE ............................................................................................................................................ 5 GUIDING PRINCIPLES .......................................................................................................................... 6 I. ACKNOWLEDGE THAT institutionalization of digital health in the national health system requires a decision and commitment by countries ........................................................................................................ 6 II. recognize THAT SUCCESSFUL DIGITAL HEALTH INITIATIVEs REQUIRE AN INTEGRATED STRATEGY ............ 6 III. PROMOTE THE APPROPRIATE USE OF DIGITAL TECHNOLOGIES FOR HEALTH ....................................... 6 IV. RECOGNIZES the URGENT NEED TO ADDRESS THE MAJOR IMPEDIMENTS FACED BY least-developed COUNTRIES IMPLEMENTING DIGITAL HEALTH TECHNOLOGIEs ....................................................................... 7 THE VISION AND STRATEGIC OBJECTIVES ............................................................................................. 7 VISION ........................................................................................................................................................ -

Digital Health Report
Q1 2020 DIGITAL HEALTH REPORT During this unprecedented time, digital health is disrupting our healthcare Machine Learning Legal Issues delivery system for the better. Digital health companies are working hard to for Digital Health Companies in provide innovative telehealth, digital screening, and testing services. They Commercial Transactions are leveraging AI to assess symptoms, model outcomes, and identify possible treatments for COVID-19. Digital health companies are providing physicians and other frontline responders with new tools to fight this pandemic. The Wilson Sonsini digital health team is here to support you during this time. Providing a cross-functional team approach for our digital health clients, we can help you: • understand the latest regulatory changes; • draft and enter into contracts; • protect your ground-breaking intellectual property (IP); and • obtain financing for your next round of innovation. Please feel free to reach out to your By Rob Parr and Scott McKinney for digital health companies, and Wilson Sonsini team member or a traditional contract approaches may not member of the digital health practice With its potential to revolutionize properly address intellectual property, industries and products of all types, group for assistance. risk allocation, data use, and other “machine learning” (ML) is a hot important issues that are unique to ML topic. ML, a sub-category of artificial or artificial intelligence more generally. intelligence, refers to software In This Issue This article is intended to highlight for algorithms that are programmed to digital health companies that wish to analyze data, learn from that analysis, Machine Learning Legal commercialize ML-enabled technologies and improve themselves.