A Framework for Selecting Digital Health Technology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

APPROPRIATE HEALTH TECHNOLOGY Emlrc44itech.Disc./1
WORLD HEALTH ORGANIZATION ~egional Office for the Eastern Mediterranean ORGANISATION MONDIALE DE LA SANTE Bureau regional de la Mediterranee orientale REGIONAL COMMITTEE FOR THE EMlRC44/Tech.Disc'/l EASTERN MEDITERRANEAN August 1997 Forty-fourth Session Original: Arabic Agenda item 7 TECHNICAL DISCUSSIONS APPROPRIATE HEALTH TECHNOLOGY EMlRC44ITech.Disc./1 CONTENTS page Executive Summary 1. Introduction....................................................................................................... 1 2. Definitions......................................................................................................... 1 2.1 Health technology..................................................................................... I 2.2 Appropriate technology............................................................................. I 3. Appropriate technology and future trends........................................................... 3 3. I General..................................................................................................... 3 3.2 Health care.................................................................... ............................ 3 3.3 Gene technology..... ....... ....... ............ ........................................................ 4 3.4 Laboratory medicine technologies............................................................. 4 3.5 Transfusion medicine................................................................................. 5 3.6 Diagnostic imaging................................................................................... -

Artificial Intelligence in Health Care: the Hope, the Hype, the Promise, the Peril
Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril Michael Matheny, Sonoo Thadaney Israni, Mahnoor Ahmed, and Danielle Whicher, Editors WASHINGTON, DC NAM.EDU PREPUBLICATION COPY - Uncorrected Proofs NATIONAL ACADEMY OF MEDICINE • 500 Fifth Street, NW • WASHINGTON, DC 20001 NOTICE: This publication has undergone peer review according to procedures established by the National Academy of Medicine (NAM). Publication by the NAM worthy of public attention, but does not constitute endorsement of conclusions and recommendationssignifies that it is the by productthe NAM. of The a carefully views presented considered in processthis publication and is a contributionare those of individual contributors and do not represent formal consensus positions of the authors’ organizations; the NAM; or the National Academies of Sciences, Engineering, and Medicine. Library of Congress Cataloging-in-Publication Data to Come Copyright 2019 by the National Academy of Sciences. All rights reserved. Printed in the United States of America. Suggested citation: Matheny, M., S. Thadaney Israni, M. Ahmed, and D. Whicher, Editors. 2019. Artificial Intelligence in Health Care: The Hope, the Hype, the Promise, the Peril. NAM Special Publication. Washington, DC: National Academy of Medicine. PREPUBLICATION COPY - Uncorrected Proofs “Knowing is not enough; we must apply. Willing is not enough; we must do.” --GOETHE PREPUBLICATION COPY - Uncorrected Proofs ABOUT THE NATIONAL ACADEMY OF MEDICINE The National Academy of Medicine is one of three Academies constituting the Nation- al Academies of Sciences, Engineering, and Medicine (the National Academies). The Na- tional Academies provide independent, objective analysis and advice to the nation and conduct other activities to solve complex problems and inform public policy decisions. -

Digital Health in a Broadband Land: the Role of Digital Health Literacy Within Rural Environments Wuyou Sui1*, Danica Facca2
Health Science Inquiry Volume 11 | 2020 Digital health in a broadband land: The role of digital health literacy within rural environments Wuyou Sui1*, Danica Facca2 1Department of Kinesiology, Western University, London, ON, Canada 2Faculty of Information and Media Sciences, Western University, London, ON, Canada *Author for correspondence ([email protected]) Abstract: The rapid rise and widespread integration of digital technologies (e.g., smartphones, personal computers) into the fabric of our society has birthed a modern means of delivering healthcare, known as digital health. Through leveraging the accessibility and ubiquity of digital technologies, digital health represents an unprecedented level of reach, impact, and scalability for health- care interventions, known as digital behaviour change interventions (DBCIs). The potential benefits associated with employing DBCIs are of particular interest for populations that are disadvantaged to receiving traditional healthcare, such as rural popu- lations. However, several factors should be considered before implementing a DBCI into a rural environment, notably, digital health literacy. Digital health literacy describes the skills necessary to successful navigate and utilize a digital health solution (e.g., DBCI). Given their limited access to high-speed internet, higher cost associated for similar services, and poorer development of information and communication technologies (ICTs), most rural populations likely report lower digital health literacy – specif- ically, computer literacy, the ability to utilize and leverage digital technologies to solve problems. Hence, DBCIs should address this ‘digital divide’ between urban and rural populations before implementation. Practical solutions could include evaluating rural communities’ access to ICTs, needs assessments with rural community members, as well as integrating rural community stakeholders into the design of digital literacy education and interventions. -

Cybersecurity and the Digital-Health: the Challenge of This Millennium
healthcare Editorial Cybersecurity and the Digital-Health: The Challenge of This Millennium Daniele Giansanti Centre Tisp, Istituto Superiore di Sanità, Via Regina Elena 299, 00161 Roma, Italy; [email protected]; Tel.: +39-06-4990-2701 1. Cybersecurity The problem of computer security is as old as computers themselves and dates back decades. The transition from: (a) a single-user to multi-user assignment to the resource and (b) access to the computer resource of the standalone type to one of the types distributed through a network made it necessary to start talking about computer security. All network architectures, from peer to peer to client-server type, are subject to IT security problems. The term Cybersecurity has recently been introduced to indicate the set of procedures and methodologies used to defend computers, servers, mobile devices, electronic systems, networks and data from malicious attacks. Cybersecurity [1–3] is therefore applied to various contexts, from the economic one to that relating to mobile technologies and includes various actions: • Network security: the procedures for using the network safely; • Application Security: the procedures and solutions for using applications safely; • Information security: the management of information in a secure way and in a privacy- sensitive manner in accordance with pre-established regulations; • Operational security: the security in IT operations, such as, for example, in bank- type transactions; • Disaster recovery and operational continuity: the procedures for restarting after problems Citation: Giansanti, D. Cybersecurity that have affected the regular/routine operation of a system and to ensure operational and the Digital-Health: The Challenge continuity. For example, using informatic solutions such as an efficient disk mirroring of This Millennium. -

Digital Health and the Global Pandemic | 1
Introduction As the world grapples with the tragic COVID-19 pandemic, it is tempting to imagine a post-COVID future that includes some silver linings. As terrible as the situation is today, this calamity will lead to some lasting, positive changes, particularly in healthcare. Virtual Care (often referred to in common parlance as simply telemedicine, and we will use them interchangeably here) has emerged as the poster child for this line of thinking. Providers and patients have dramatically increased the use of telemedicine to ensure continued access to quality healthcare services while maintaining social distance and modulating the enormous burden on our healthcare workers and facilities. Regulators and payers are encouraging and enabling this shift by temporarily relaxing policies that have historically limited telemedicine. Adjacent areas of digital health including digital therapeutics, digital disease management, and remote monitoring have followed suit, finding similarly relaxed policies, more accessible reimbursement, and increased adoption by providers and patients alike. Many have questioned whether these changes will endure as life returns to a “new normal”, or if policies will be reverted and accelerated growth will subside. We begin by examining the potential for COVID-19 to drive lasting change for various categories of digital health technologies. Given the large scale of virtual care, in combination with its potential for lasting COVID-19 impact, we then will dive deeply into this category as a leading indicator of other areas of digital health. Because the US experience has been so widely covered (and to some degree it is still playing out in real time) we highlight key characteristics and trends across Asia Pacific (APAC) and European markets. -

Strengthening Care Management with Health Information Technology a Learning Guide
Strengthening Care Management with Health Information Technology A Learning Guide Presenting lessons learned by the 17 Beacon Community Awardees of the Office of the National Coordinator for Health Information Technology in the U.S. Department of Health and Human Services July 2013 i The Beacon Community Cooperative Agreement Program demonstrates how health IT investments and Meaningful Use of electronic health records (EHR) advance the vision of patient-centered care, while achieving the three-part aim of better health, better care at lower cost. The Department of Health and Human Services, Office of the National Coordinator for Health IT (ONC) is providing $250 million over three years to 17 selected communities throughout the United States that have already made inroads in the development of secure, private, and accurate systems of EHR adoption and health information exchange. Each of the 17 communities—with its unique population and regional context—is actively pursuing the following areas of focus: • Building and strengthening the health IT infrastructure and exchange capabilities within communities, positioning each community to pursue a new level of sustainable health care quality and efficiency over the coming years; • Translating investments in health IT to measureable improvements in cost, quality and population health; and • Developing innovative approaches to performance measurement, technology and care delivery to accelerate evidence generation for new approaches. For more information about the Beacon Community Program visit www.healthit.gov. This Learning Guide is part of the Beacon Nation project and is funded by the Hawai’i Island Beacon Community, an awardee of ONC Beacon Community Program. The Learning Guide was produced by Booz Allen Hamilton, under a contract with the Hawai’i Island Beacon Community. -

How to Leverage Health Technology to Improve Patient Flow
How to Leverage Health Technology to Improve Patient Flow 3/31/2017 A growing population has led to an increased demand for healthcare services. Concurrently, healthcare reforms and reimbursement requirements necessitate improvements in quality care and patient satisfaction. Healthcare facilities have begun searching for ways in which to handle the influx of patients without sacrificing either quality or the patient experience. How can your facility achieve increased volume and profits while maintaining quality and improving patient satisfaction? This whitepaper addresses how RTLS (Real Time Locating System) technology can be implemented to solve critical issues such as: · Increased capacity · Decreased waiting times · Patient and staff satisfaction · Increased healthcare staff productivity Increased Capacity The aging population in the United States is requiring more healthcare services. As the Baby Boomer population ages, almost twenty percent of the current population living in the United States will reach age 65 or older. This increase in the aging population leads to a significant growth in the number of individuals with chronic conditions. According to the American Hospital Association, the number of Boomers with multiple chronic conditions is continuing to grow and will reach about 37 million adults by 2030.i The prevalence of chronic conditions is also increasing in the United States population as a whole and calls for increased medical services and innovative approaches on how to properly deliver care to this population. Many healthcare delivery systems are utilizing RTLS technology to meet the increased population challenge. The Nor-Lea Medical Clinic in Lovington, New Mexico implemented an RTLS system to handle their growing influx of patients. -
Best Practices of Cybersecurity in the Healthcare Industries
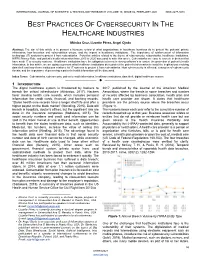
INTERNATIONAL JOURNAL OF SCIENTIFIC & TECHNOLOGY RESEARCH VO`LUME 10, ISSUE 02, FEBRUARY 2021 ISSN 2277-8616 BEST PRACTICES OF CYBERSECURITY IN THE HEALTHCARE INDUSTRIES Mónica Cruz, Lizzette Pérez, Angel Ojeda Abstract: The aim of this article is to present a literature review of what organizations in healthcare business do to protect the patients‘ private information, how breaches and vulnerabilities occurs, and the impact in healthcare institutions. The importance of reinforcement of information technology (IT) systems to protect it from cyberattacks. Forty-five articles related to the theme of cybersecurity, cyberattacks, healthcare institutions, HIPPA Privacy Rule, and patient‘s health information from 2015 to 2020 was used to write this article. Cyberattacks are easy to execute in devices that have weak IT or security systems. Healthcare institutions have the obligation to invest in strong software‘s to ensure the protection of patient‘s health information. In this article, we are going to present what healthcare institutions do to protect the patient's information to avoid the implications involving data theft and how these institutions reinforce its‘ IT systems to protect it from cyberattacks. How cybersecurity is affected, examples of cybersecurity threats, and the importance of preserving a patient‘s health information will be discussed. Index Terms: Cyberattacks, cybersecurity, patient‘s health information, healthcare institutions, data theft, digital healthcare system —————————— —————————— 1 INTRODUCTION The digital healthcare system is threatened by hackers to 2017, published by the Journal of the American Medical breach the critical infrastructure (Athinaiou, 2017). Hackers Association, where the trends in some breaches and number favor stealing health care records, which includes personal of records affected by business association, health plan and information like credit cards, financial, and banking records. -

Biomedical Engineering (BMD ENG) 1
Biomedical Engineering (BMD_ENG) 1 Through the course, students will learn how to apply these experimental BIOMEDICAL ENGINEERING and computational genomics technologies to study gene expression regulation underlying various biological processes, such as oncogenesis. (BMD_ENG) Students will also apply computational and statistical skills, using linux and R/Matlab/Python. BMD_ENG 101-0 Introduction to Biomedical Engineering (0 Unit) BMD_ENG 317-0 Biochemical Sensors (1 Unit) Information to 1) help students determine if BME is the right major Theory, design, and applications of chemical sensors used in medical for them and 2) learn how to make the most of their undergraduate diagnosis and patient monitoring. Electrochemical and optical sensors. experience. The field of biomedical engineering, career and research Prerequisites: BIOL_SCI 215-0; BIOL_SCI 219-0; CHEM 210-1; opportunities, ethics. PHYSICS 135-2; PHYSICS 135-3. BMD_ENG 207-0 BME Lab: Experimental Design (0.5 Unit) A laboratory BMD_ENG 323-0 Visual Engineering Science (1 Unit) course focusing on quantitative physiological measurements Mammalian visual system. Physiological optics. Visual image and analyses, instrument characterization, statistical design of representation and interpretation. Visual adaptation. Motion. Color vision. experiments, and training in preparation and organization of laboratory Prerequisite: PHYSICS 135-2. notes and reports. Prerequisite: BMD_ENG 220-0 or IEMS 303-0 or MECH_ENG 359-0. BMD_ENG 325-0 Introduction to Medical Imaging (1 Unit) Diagnostic X-rays; X-ray film and radiographic image; computed BMD_ENG 220-0 Introduction to Biomedical Statistics (1 Unit) Basic tomography; ultrasound. statistical concepts presented with emphasis on their relevance to Prerequisite: PHYSICS 135-3 or equivalent. biological and medical investigations. -

Executive Brief: Top 10 Health Technology Hazards for 2017
EXECUTIVE BRIEF Top 10 Health Technology Hazards for 2017 A Report from Health Devices November 2016 EXECUTIVE BRIEF Top 10 Health Technology Hazards for 2017 A Report from Health Devices November 2016 Top 10 Health Technology Hazards for 2017 Executive Brief ECRI Institute is providing this abridged version of its 2017 Top 10 list of health technology hazards as a free public service to inform healthcare facilities about important safety issues involving the use of medical devices and systems. The full report— including detailed problem descriptions and ECRI Institute’s step-by-step recommendations for addressing the hazards—is available to members of certain ECRI Institute programs through their membership web pages. The List for 2017 1. Infusion Errors Can Be Deadly If Simple Safety Steps Are Overlooked 2. Inadequate Cleaning of Complex Reusable Instruments Can Lead to Infections 3. Missed Ventilator Alarms Can Lead to Patient Harm 4. Undetected Opioid-Induced Respiratory Depression 5. Infection Risks with Heater-Cooler Devices Used in Cardiothoracic Surgery 6. Software Management Gaps Put Patients, and Patient Data, at Risk 7. Occupational Radiation Hazards in Hybrid ORs 8. Automated Dispensing Cabinet Setup and Use Errors May Cause Medication Mishaps 9. Surgical Stapler Misuse and Malfunctions 10. Device Failures Caused by Cleaning Products and Practices The Purpose of the List The safe use of health technology—from basic infusion pumps to large, complex imaging systems—requires identifying possible sources of danger or difficulty with those technologies and taking steps to minimize the likelihood that adverse events will occur. This list will help healthcare facilities do that. -

Be He@Lthy, Be Mobile – 2018 Annual Report
BE HE@LTHY, BE MOBILE Annual Report 2018 Be He@lthy, Be Mobile Annual Report 2018 ISBN: 978-92-4-151625-9 WHO ISBN: 978-92-61-29451-9 ITU ISBN: 978-92-61-29461-8 ITU (PDF) Some rights reserved. This work is available under the Creative Commons Attribution- NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons. org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO or ITU endorses any specific organization, products or services. The unauthorized use of the WHO or ITU names or logos is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO) or the International Telecommunication Union (ITU). Neither WHO nor ITU are responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization (http://www.wipo.int/ amc/en/mediation/rules). Suggested citation. Be He@lthy, Be Mobile Annual Report 2018. Geneva: World Health Organization and International Telecommunication Union, 2019. -

Electronic Health Records in India
CSD Working Paper Series: Towards a New Indian Model of Information and Communications Technology-Led Growth and Development Electronic Health Records in India ICT India Working Paper #25 Manisha Wadhwa March 2020 CSD Working Paper Series: Towards a New Indian Model of Information and Communications Technology-Led Growth and Development Table of Contents Abbreviations ................................................................................................................................................ 4 Abstract ......................................................................................................................................................... 5 Introduction .................................................................................................................................................. 6 Benefits of EHR ............................................................................................................................................. 8 Initiatives by the Government of India ......................................................................................................... 8 EHR Standards ........................................................................................................................................... 8 Goals of EHR Standards ......................................................................................................................... 9 Need for EHR Standards .......................................................................................................................