UNIT 6 Digestive System Pathological Conditions APPENDICITIS
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Print This Article
International Surgery Journal Lew D et al. Int Surg J. 2021 May;8(5):1575-1578 http://www.ijsurgery.com pISSN 2349-3305 | eISSN 2349-2902 DOI: https://dx.doi.org/10.18203/2349-2902.isj20211831 Case Report Acute gangrenous appendicitis and acute gangrenous cholecystitis in a pregnant patient, a difficult diagnosis: a case report David Lew, Jane Tian*, Martine A. Louis, Darshak Shah Department of Surgery, Flushing Hospital Medical Center, Flushing, New York, USA Received: 26 February 2021 Accepted: 02 April 2021 *Correspondence: Dr. Jane Tian, E-mail: [email protected] Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited. ABSTRACT Abdominal pain is a common complaint in pregnancy, especially given the physiological and anatomical changes that occur as the pregnancy progresses. The diagnosis and treatment of common surgical pathologies can therefore be difficult and limited by the special considerations for the fetus. While uncommon in the general population, concurrent or subsequent disease processes should be considered in the pregnant patient. We present the case of a 36 year old, 13 weeks pregnant female who presented with both acute appendicitis and acute cholecystitis. Keywords: Appendicitis, Cholecystitis, Pregnancy, Pregnant INTRODUCTION population is rare.5 Here we report a case of concurrent appendicitis and cholecystitis in a pregnant woman. General surgeons are often called to evaluate patients with abdominal pain. The differential diagnosis list must CASE REPORT be expanded in pregnant woman and the approach to diagnosing and treating certain diseases must also be A 36 year old, 13 weeks pregnant female (G2P1001) adjusted to prevent harm to the fetus. -

Umbilical Hernia with Cholelithiasis and Hiatal Hernia
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Springer - Publisher Connector Yamanaka et al. Surgical Case Reports (2015) 1:65 DOI 10.1186/s40792-015-0067-8 CASE REPORT Open Access Umbilical hernia with cholelithiasis and hiatal hernia: a clinical entity similar to Saint’striad Takahiro Yamanaka*, Tatsuya Miyazaki, Yuji Kumakura, Hiroaki Honjo, Keigo Hara, Takehiko Yokobori, Makoto Sakai, Makoto Sohda and Hiroyuki Kuwano Abstract We experienced two cases involving the simultaneous presence of cholelithiasis, hiatal hernia, and umbilical hernia. Both patients were female and overweight (body mass index of 25.0–29.9 kg/m2) and had a history of pregnancy and surgical treatment of cholelithiasis. Additionally, both patients had two of the three conditions of Saint’s triad. Based on analysis of the pathogenesis of these two cases, we consider that these four diseases (Saint’s triad and umbilical hernia) are associated with one another. Obesity is a common risk factor for both umbilical hernia and Saint’s triad. Female sex, older age, and a history of pregnancy are common risk factors for umbilical hernia and two of the three conditions of Saint’s triad. Thus, umbilical hernia may readily develop with Saint’s triad. Knowledge of this coincidence is important in the clinical setting. The concomitant occurrence of Saint’s triad and umbilical hernia may be another clinical “tetralogy.” Keywords: Saint’s triad; Cholelithiasis; Hiatal hernia; Umbilical hernia Background of our knowledge, no previous reports have described the Saint’s triad is characterized by the concomitant occur- coexistence of umbilical hernia with any of the three con- rence of cholelithiasis, hiatal hernia, and colonic diverticu- ditions of Saint’s triad. -

Practice Parameters for the Treatment of Patients with Dominantly Inherited Colorectal Cancer
Practice Parameters For The Treatment Of Patients With Dominantly Inherited Colorectal Cancer Diseases of the Colon & Rectum 2003;46(8):1001-1012 Prepared by: The Standards Task Force The American Society of Colon and Rectal Surgeons James Church, MD; Clifford Simmang, MD; On Behalf of the Collaborative Group of the Americas on Inherited Colorectal Cancer and the Standards Committee of the American Society of Colon and Rectal Surgeons. The American Society of Colon and Rectal Surgeons is dedicated to assuring high quality patient care by advancing the science, prevention, and management of disorders and diseases of the colon, rectum, and anus. The standards committee is composed of Society members who are chosen because they have demonstrated expertise in the specialty of colon and rectal surgery. This Committee was created in order to lead international efforts in defining quality care for conditions related to the colon, rectum, and anus. This is accompanied by developing Clinical Practice Guidelines based on the best available evidence. These guidelines are inclusive, and not prescriptive. Their purpose is to provide information on which decisions can be made, rather than dictate a specific form of treatment. These guidelines are intended for the use of all practitioners, health care workers, and patients who desire information about the management of the conditions addressed by the topics covered in these guidelines. Practice Parameters for the Treatment of Patients With Dominantly Inherited Colorectal Cancer Inherited colorectal cancer includes two main syndromes in which predisposition to the disease is based on a germline mutation that may be transmitted from parent to child. -

Diagnosis and Treatment of Perianal Crohn Disease: NASPGHAN Clinical Report and Consensus Statement
CLINICAL REPORT Diagnosis and Treatment of Perianal Crohn Disease: NASPGHAN Clinical Report and Consensus Statement ÃEdwin F. de Zoeten, zBrad A. Pasternak, §Peter Mattei, ÃRobert E. Kramer, and yHoward A. Kader ABSTRACT disease. The first description connecting regional enteritis with Inflammatory bowel disease is a chronic inflammatory disorder of the perianal disease was by Bissell et al in 1934 (2), and since that time gastrointestinal tract that includes both Crohn disease (CD) and ulcerative perianal disease has become a recognized entity and an important colitis. Abdominal pain, rectal bleeding, diarrhea, and weight loss consideration in the diagnosis and treatment of CD. Perianal characterize both CD and ulcerative colitis. The incidence of IBD in the Crohn disease (PCD) is defined as inflammation at or near the United States is 70 to 150 cases per 100,000 individuals and, as with other anus, including tags, fissures, fistulae, abscesses, or stenosis. autoimmune diseases, is on the rise. CD can affect any part of the The symptoms of PCD include pain, itching, bleeding, purulent gastrointestinal tract from the mouth to the anus and frequently will include discharge, and incontinence of stool. perianal disease. The first description connecting regional enteritis with perianal disease was by Bissell et al in 1934, and since that time perianal INCIDENCE AND NATURAL HISTORY disease has become a recognized entity and an important consideration in the Limited pediatric data describe the incidence and prevalence diagnosis and treatment of CD. Perianal Crohn disease (PCD) is defined as of PCD. The incidence of PCD in the pediatric age group has been inflammation at or near the anus, including tags, fissures, fistulae, abscesses, estimated to be between 13.6% and 62% (3). -

Utility of the Digital Rectal Examination in the Emergency Department: a Review
The Journal of Emergency Medicine, Vol. 43, No. 6, pp. 1196–1204, 2012 Published by Elsevier Inc. Printed in the USA 0736-4679/$ - see front matter http://dx.doi.org/10.1016/j.jemermed.2012.06.015 Clinical Reviews UTILITY OF THE DIGITAL RECTAL EXAMINATION IN THE EMERGENCY DEPARTMENT: A REVIEW Chad Kessler, MD, MHPE*† and Stephen J. Bauer, MD† *Department of Emergency Medicine, Jesse Brown VA Medical Center and †University of Illinois-Chicago College of Medicine, Chicago, Illinois Reprint Address: Chad Kessler, MD, MHPE, Department of Emergency Medicine, Jesse Brown Veterans Hospital, 820 S Damen Ave., M/C 111, Chicago, IL 60612 , Abstract—Background: The digital rectal examination abdominal pain and acute appendicitis. Stool obtained by (DRE) has been reflexively performed to evaluate common DRE doesn’t seem to increase the false-positive rate of chief complaints in the Emergency Department without FOBTs, and the DRE correlated moderately well with anal knowing its true utility in diagnosis. Objective: Medical lit- manometric measurements in determining anal sphincter erature databases were searched for the most relevant arti- tone. Published by Elsevier Inc. cles pertaining to: the utility of the DRE in evaluating abdominal pain and acute appendicitis, the false-positive , Keywords—digital rectal; utility; review; Emergency rate of fecal occult blood tests (FOBT) from stool obtained Department; evidence-based medicine by DRE or spontaneous passage, and the correlation be- tween DRE and anal manometry in determining anal tone. Discussion: Sixteen articles met our inclusion criteria; there INTRODUCTION were two for abdominal pain, five for appendicitis, six for anal tone, and three for fecal occult blood. -

ACUTE Yellow Atrophy Ofthe Liver Is a Rare Disease; Ac
ACUTE YELLOW ATROPHY OF THE LIVER AS A SEQUELA TO APPENDECTOMY.' BY MAX BALLIN, M.D., OF DETROIT, MICHIGAN. ACUTE yellow atrophy of the liver is a rare disease; ac- cording to Osler about 250 cases are on record. This affection is also called Icterus gravis, Fatal icterus, Pernicious jaundice, Acute diffuse hepatitis, Hepatic insufficiency, etc. Acute yellow atrophy of the liver is characterized by a more or less sudden onset of icterus increasing to the severest form, headaches. insomnia, violent delirium, spasms, and coma. There are often cutaneous and mucous hiemorrhages. The temperature is usually high and irregular. The pulse, first normal, later rapid; urine contains bile pigments, albumen, casts, and products of incomplete metabolism of albumen, leucin, and tyrosin, the pres- ence of which is considered pathognomonic. The affection ends mostly fatally, but there are recoveries on record. The findings of the post-mortem are: liver reduced in size; cut surface mot- tled yellow, sometimes with red spots (red atrophy), the paren- chyma softened and friable; microscopically the liver shows biliary infiltration, cells in all stages of degeneration. Further, we find parenchymatous nephritis, large spleen, degeneration of muscles, haemorrhages in mucous and serous membranes. The etiology of this affection is not quite clear. We find the same changes in phosphorus poisoning; many believe it to be of toxic origin, but others consider it to be of an infectious nature; and we have even findings of specific germs (Klebs, Tomkins), of streptococci (Nepveu), staphylococci (Bourdil- lier), and also the Bacillus coli is found (Mintz) in the affected organs. The disease seems to occur always secondary to some other ailment, and is observed mostly during pregnancy (about one-third of all cases, hence the predominance in women), after Read before the Wayne County Medical Society, January 5, I903. -

Plugs for Anal Fistula Repair Original Policy Date: November 26, 2014 Effective Date: January 1, 2021 Section: 7.0 Surgery Page: Page 1 of 12
Medical Policy 7.01.123 Plugs for Anal Fistula Repair Original Policy Date: November 26, 2014 Effective Date: January 1, 2021 Section: 7.0 Surgery Page: Page 1 of 12 Policy Statement Biosynthetic fistula plugs, including plugs made of porcine small intestine submucosa or of synthetic material, are considered investigational for the repair of anal fistulas. NOTE: Refer to Appendix A to see the policy statement changes (if any) from the previous version. Policy Guidelines There is a specific CPT code for the use of these plugs in the repair of an anorectal fistula: • 46707: Repair of anorectal fistula with plug (e.g., porcine small intestine submucosa [SIS]) Description Anal fistula plugs (AFPs) are biosynthetic devices used to promote healing and prevent the recurrence of anal fistulas. They are proposed as an alternative to procedures including fistulotomy, endorectal advancement flaps, seton drain placement, and use of fibrin glue in the treatment of anal fistulas. Related Policies • N/A Benefit Application Benefit determinations should be based in all cases on the applicable contract language. To the extent there are any conflicts between these guidelines and the contract language, the contract language will control. Please refer to the member's contract benefits in effect at the time of service to determine coverage or non-coverage of these services as it applies to an individual member. Some state or federal mandates (e.g., Federal Employee Program [FEP]) prohibits plans from denying Food and Drug Administration (FDA)-approved technologies as investigational. In these instances, plans may have to consider the coverage eligibility of FDA-approved technologies on the basis of medical necessity alone. -

Endoscopy Rotation Coordination and Goals and Objects Department of Surgery Stanford School of Medicine (8/15/17, Jnl)
Endoscopy Rotation Coordination And Goals and Objects Department of Surgery Stanford School of Medicine (8/15/17, jnl) Rotation Director: James Lau, MD ATTENDINGS and CONTACT INFORMATION Cell Phone E-mail Address James Lau, MD (702) 306-8780 [email protected] Homero Rivas, MD MBA (972) 207-2381 [email protected] Dan Azagury, MD (650) 248-3173 [email protected] Shai Friedland, MD [email protected] Andrew Shelton, MD [email protected] Natalie Kirilcuk, MD [email protected] Cindy Kin, MD [email protected] Laren Becker, MD [email protected] Jennifer Pan, MD [email protected] Suzanne Matsui, MD [email protected] Ramsey Cheung, MD [email protected] KEYPOINT The key for this rotation is that you need to show initiative. TEXT Practical Gastrointestinal Endoscopy: The Fundamentals. Sixth Edition. By Peter B. Cotton, Christopher B. Williams, Robert H. Hawes and Brian P. Saunders. You are responsible for the material to enhance your understanding and supplement your past experiences. Lots of pictures and tips and tricks. Quick read. Copy of text available for purchase on Amazon.com or for check out from the Lane Library. Procedure Schedule Monday Tuesday Wednesday Thursday Friday Laren Becker Jennifer Pan Shelton/Kirilcuk/Kin Ramsey Suzanne (VA (VA Colonoscopy 8:00 am Cheung (VA Matsui (VA Livermore) Livermore) (Stanford Endoscopy) Livermore) Livermore) Every other Tuesday Rivas/Lau alternating Upper/Occasional Lower 1 Endoscopy 9a-1p (Stanford Endoscopy) Suzanne Matsui (VA Livermore) The Staff Drs. Becker, Cheung, Pan, and Matsui are gastroenterologists that perform 75% colonoscopies and 25% upper endoscopies at the Livermore location for the Palo Alto VA. -

The Differences Between ICD-9 and ICD-10
Preparing for the ICD-10 Code Set: Fact Sheet 2 October 1, 2015 Compliance Date Get the Facts to be Compliant Alert: The new ICD-10 compliance date is October 1, 2015. The Differences Between ICD-9 and ICD-10 This is the second fact sheet in a series and is focused on the differences between the ICD-9 and ICD-10 code sets. Collectively, the fact sheets will provide information, guidance, and checklists to assist you with understanding what you need to do to implement the ICD-10 code set. The ICD-10 code sets are not a simple update of the ICD-9 code set. The ICD-10 code sets have fundamental changes in structure and concepts that make them very different from ICD-9. Because of these differences, it is important to develop a preliminary understanding of the changes from ICD-9 to ICD-10. This basic understanding of the differences will then identify more detailed training that will be needed to appropriately use the ICD-10 code sets. In addition, seeing the differences between the code sets will raise awareness of the complexities of converting to the ICD-10 codes. Overall Comparisons of ICD-9 to ICD-10 Issues today with the ICD-9 diagnosis and procedure code sets are addressed in ICD-10. One concern today with ICD-9 is the lack of specificity of the information conveyed in the codes. For example, if a patient is seen for treatment of a burn on the right arm, the ICD-9 diagnosis code does not distinguish that the burn is on the right arm. -
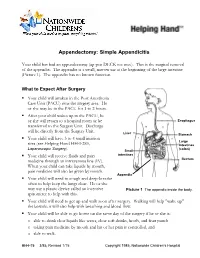
Appendectomy: Simple Appendicitis
Appendectomy: Simple Appendicitis Your child has had an appendectomy (ap pen DECK toe mee). This is the surgical removal of the appendix. The appendix is a small, narrow sac at the beginning of the large intestine (Picture 1). The appendix has no known function. What to Expect After Surgery . Your child will awaken in the Post Anesthesia Care Unit (PACU) near the surgery area. He or she may be in the PACU for 1 to 2 hours. After your child wakes up in the PACU, he or she will return to a hospital room or be Esophagus transferred to the Surgery Unit. Discharge will be directly from the Surgery Unit. Liver Stomach . Your child will have 3 to 4 small incision Large sites (see Helping Hand HH-I-283, Intestines Laparoscopic Surgery (colon) ). Small . Your child will receive fluids and pain intestines medicine through an intravenous line (IV). Rectum When your child can take liquids by mouth, pain medicine will also be given by mouth. Appendix . Your child will need to cough and deep-breathe often to help keep the lungs clear. He or she may use a plastic device called an incentive Picture 1 The appendix inside the body. spirometer to help with this. Your child will need to get up and walk soon after surgery. Walking will help "wake up" the bowels; it will also help with breathing and blood flow. Your child will be able to go home on the same day of the surgery if he or she is: o able to drink clear liquids like water, clear soft drinks, broth, and fruit punch o taking pain medicine by mouth and his or her pain is controlled, and o able to walk. -

Descriptive Study Regarding the Etiological Factors Responsible for Secondary Bacterial Peritonitis in Patients Admitted in a Te
International Journal of Health Sciences and Research Vol.10; Issue: 7; July 2020 Website: www.ijhsr.org Original Research Article ISSN: 2249-9571 Descriptive Study Regarding the Etiological Factors Responsible for Secondary Bacterial Peritonitis in Patients Admitted in a Tertiary Care Hospital in Trans Himalayan Region Raj Kumar1, Rahul Gupta2, Anjali Sharma3, Rajesh Chaudhary4 1MS General Surgery, Civil Hospital Baijnath, Himachal Pradesh 2MD Community Medicine, District Programme Officer, Health and Family Welfare, Himachal Pradesh 3Resident Doctor, Department of Microbiology, DRPGMC Kangra at Tanda, Himachal Pradesh 4MS General Surgery, Civil Hospital Nagrota Bagwan, Himachal Pradesh Corresponding Author: Rahul Gupta ABSTRACT Peritonitis is an inflammation of the peritoneum. Primary peritonitis which is spontaneous bacterial peritonitis, Secondary peritonitis due to infection from intraabdominal source or spillage of its contents and Tertiary peritonitis which is recurrent or reactivation of secondary peritonitis. The present study was aimed to determine the etiology of generalized secondary peritonitis among the patients admitted in Department of General Surgery, Dr RPGMC Kangra at Tanda. This descriptive observational study was conducted in the department of surgery Dr. Rajendra Prasad Government Medical College Kangra at Tanda consisting of patients having acute generalised secondary peritonitis presented in emergency department or Surgery outdoor patient department over a period of one year from December 2016 through November 2017. The most common etiology of generalized secondary peritonitis in our patients was peptic ulcer disease (77.13%) followed by perforated appendicitis (9.8%). Etiological factors of secondary generalised peritonitis have a different pattern in different geographical regions. Peptic ulcer disease remains the commonest etiology of secondary peritonitis in India followed by enteric perforation which is in contrast to the western studies where appendicular and colon perforations are more common. -

Surgery for Colon and Rectal Cancer
Colon and Rectal Surgery Mohammed Bayasi, MD Department of Surgery Colon and Rectal Surgery What is a Colon and Rectal Surgeon? • Fully trained General Surgeon. • Has done additional training in the diseases of colon and rectum. Why Colon and Rectal Surgery? • Surgical and non surgical therapy for multiple diseases. • Chance to help cancer patients by removing tumor, potentially curing them. • Variety of cases, ages and patient populations. • Specialized area. Colorectal Diseases • Colon • Rectum/Anus – Cancer – Hemorrhoids – Diverticulitis – Anal fistula and – Inflammatory Bowel abscess Disease (Crohn, UC) – Anal fissure – Polyps – Prolapse Symptoms/Signs • Pain • Itching • Discharge • Bleeding • Lump Anatomy Lesson Colon • Extracts water and nutrients. • Helps to form and excrete waste. • Stores important bacteria flora. • Length: 1.5 meters long = 4.9 feet = 59 inches Colon Rectum/Anus • The final portion of the colon. • Area contains muscles important in controlling defecation and flatulence. Rectum/Anus When to see a Colon and Rectal Surgeon • Referral from another physician (Gastroenterology, PCP). • Treatment of anorectal diseases. • Blood with stool, abdominal pain, rectal pain. Hemorrhoids • Internal and external. • Cushions of blood vessels. • When enlarged, they cause bleeding and pain. Treatment • Treatment of symptomatic hemorrhoids is directed by the symptoms themselves. It can broadly be categorized into four groups: − Medical therapy − Office-based procedure − Operative therapies − Emergent interventions Anorectal Abscess • It is a collection of pus in the perianal area. Normal • Causes pain and rectal gland drainage, and if it progresses, fever and systemic Abscess infection. • Treated with incision and drainage. Anorectal Fistula • A tunnel between the inside of the anus and the skin. • Causes discharge, pain, and formation of abscess.