DRM 2013 28 Metro North Summary Report Final.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Metro-North Railroad Committee Meeting
Metro-North Railroad Committee Meeting March 2019 Members S. Metzger N. Brown R. Glucksman C. Moerdler M. Pally A. Saul V. Vanterpool N. Zuckerman Metro-North Railroad Committee Meeting 2 Broadway 20th Floor Board Room New York, NY Monday, 3/25/2019 8:30 - 9:30 AM ET 1. Public Comments 2. Approval of Minutes Minutes - Page 4 3. 2019 Work Plan 2019 MNR Work Plan - Page 14 4. President's Reports Safety MNR Safety Report - Page 22 MTA Police Report MTA Police Report - Page 25 5. Information Items MNR Information Items - Page 31 Annual Strategic Investments & Planning Studies Annual Strategic Investments & Planning Studies - Page 32 Annual Elevator & Escalator Report Annual Elevator & Escalator Report - Page 66 Customer Satisfaction Survey Results Customer Satisfaction Survey Results - Page 74 PTC Status Report PTC Status Report - Page 122 Lease Agreement for Hastings Station Lease Agreement for Hastings Station - Page 133 License agreement for Purdy's Station License Agreement for Purdy's Station - Page 135 6. Procurements MNR Procurements - Page 137 MNR Non-Competitive Procurements MNR Non-Competitive Procurements - Page 140 MNR Competitive Procurements MNR Competitive Procurements - Page 142 7. Operations Report MNR Operations Report - Page 149 8. Financial Report MNR Finance Report - Page 160 9. Ridership Report MNR Ridership Report - Page 181 10. Capital Program Report MNR Capital Program Report - Page 192 Next Meeting: Joint meeting with Long Island on Monday, April 15th @ 8:30 a.m. Minutes of the Regular Meeting Metro-North Committee Monday, February 25, 2019 Meeting held at 2 Broadway – 20th Floor New York, New York 10004 8:30 a.m. -

Harlem River Waterfront
Amtrak and Henry Hudson Bridges over the Harlem River, Spuyten Duvyil HARLEM BRONX RIVER WATERFRONT MANHATTAN Linking a River’s Renaissance to its Upland Neighborhoods Brownfied Opportunity Area Pre-Nomination Study prepared for the Bronx Council for Environmental Quality, the New York State Department of State and the New York State Department of Environmental Conservation with state funds provided through the Brownfield Opportunity Areas Program. February 2007 Acknowledgements Steering Committee Dart Westphal, Bronx Council for Environmental Quality – Project Chair Colleen Alderson, NYC Department of Parks and Recreation Karen Argenti, Bronx Council for Environmental Quality Justin Bloom, Esq., Brownfield Attorney Paula Luria Caplan, Office of the Bronx Borough President Maria Luisa Cipriano, Partnership for Parks (Bronx) Curtis Cravens, NYS Department of State Jane Jackson, New York Restoration Project Rita Kessler, Bronx Community Board 7 Paul S. Mankiewicz, PhD, New York City Soil & Water Conservation District Walter Matystik, M.E.,J.D., Manhattan College Matt Mason, NYC Department of City Planning David Mojica, Bronx Community Board 4 Xavier Rodriguez, Bronx Community Board 5 Brian Sahd, New York Restoration Project Joseph Sanchez, Partnership for Parks James Sciales, Empire State Rowing Association Basil B. Seggos, Riverkeeper Michael Seliger, PhD, Bronx Community College Jane Sokolow LMNOP, Metro Forest Council Shino Tanikawa, New York City Soil and Water Conservation District Brad Trebach, Bronx Community Board 8 Daniel Walsh, NYS Department of Environmental Conservation Project Sponsor Bronx Council for Environmental Quality Municipal Partner Office of Bronx Borough President Adolfo Carrión, Jr. Fiscal Administrator Manhattan College Consultants Hilary Hinds Kitasei, Project Manager Karen Argenti, Community Participation Specialist Justin Bloom, Esq., Brownfield Attorney Paul S. -
Bicycle Access and Parking for Subway & Commuter Rail Users (Full)
NYC Dept City Planning bike ride Transportation Division Bicycle Access and Parking +for Subway and Commuter Rail Users Fall 2009 Bicycle Access and Parking for Subway & Commuter Rail Users Project Identification Number (PIN): PTCP08D00.G10 The preparation of this report was financed in part through funds from the U.S. Department of Transportation, Federal Highway Administration. This document is disseminated under the sponsorship of the U.S. Department of Transportation in the interest of information exchange. The contents of this report reflect the view of the author who is responsible for the facts and accuracy of the data presented herein. The contents do not necessarily reflect the official view or policies of the Federal Highway Administration of the New York Metropolitan Transportation Council. This report does not constitute a standard, specification, or regulation. NYC Department of City Planning, Transportation Division Bicycle Access and Parking for Subway & Commuter Rail Users Table of Contents Executive Summary 1 Bicycle Parking Possibilities in NYC 57 Bicycle Cages Introduction 7 Biceberg Bigloo Existing Conditions 8 Current Bicycle Parking Conditions Case Studies 61 Metropolitan Transportation Authority Bicycle Parking Policies Fordham - Metro North, The Bronx New York City Transit Grant City - Staten Island Rail Road, Staten Island Metro North Graham Avenue - L, Brooklyn Long Island Rail Road 23rd Street - F,V, Manhattan Bicycle Parking Concerns for MTA Customers DeKalb Avenue - B,Q,R,M, Brooklyn New York City Department -
Bicycle Access and Parking for Subway & Commuter
NYC Dept City Planning bike ride Transportation Division Bicycle Access and Parking +for Subway and Commuter Rail Users Fall 2009 Bicycle Access and Parking for Subway & Commuter Rail Users Project Identification Number (PIN): PTCP08D00.G10 The preparation of this report was financed in part through funds from the U.S. Department of Transportation, Federal Highway Administration. This document is disseminated under the sponsorship of the U.S. Department of Transportation in the interest of information exchange. The contents of this report reflect the view of the author who is responsible for the facts and accuracy of the data presented herein. The contents do not necessarily reflect the official view or policies of the Federal Highway Administration of the New York Metropolitan Transportation Council. This report does not constitute a standard, specification, or regulation. NYC Department of City Planning, Transportation Division Bicycle Access and Parking for Subway & Commuter Rail Users Table of Contents Executive Summary 1 Bicycle Parking Possibilities in NYC 57 Bicycle Cages Introduction 7 Biceberg Bigloo Existing Conditions 8 Current Bicycle Parking Conditions Case Studies 61 Metropolitan Transportation Authority Bicycle Parking Policies Fordham - Metro North, The Bronx New York City Transit Grant City - Staten Island Rail Road, Staten Island Metro North Graham Avenue - L, Brooklyn Long Island Rail Road 23rd Street - F,V, Manhattan Bicycle Parking Concerns for MTA Customers DeKalb Avenue - B,Q,R,M, Brooklyn New York City Department -

Transfer to HUDSON RAIL LINK Hudson Rail Link Buses Will Meet All Trains Listed Above
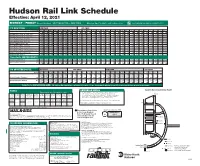
Hudson Rail Link Schedule MONDAY - FRIDAY (Except Holidays) SPUYTEN DUYVIL—NEW YORK Effective October 15, 2012 through January 4, 2013 NO SMOKING ON BOARD TRAINS/BUSES TO NEW YORK AM PEAK OFF-PEAK BUS ROUTE LLJKMJKMJKMJKMJKMJKM LLLLLLLLLJKMJKMJKML LLL AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM Henry Hudson Pkwy. & 246 St. 5 46 6 18 6 48 7 08 7 28 7 49 8 10 8 38 9 02 9 35 10 31 11 21 12 21 1 21 2 21 3 21 4 21 4 53 6 14 6 57 8 00 9 19 10 19 11 19 Henry Hudson Pkwy. & 239 St. 5 47 6 19 6 49 7 09 7 31 7 51 8 12 8 40 9 04 9 36 10 32 11 22 12 22 1 22 2 22 3 22 4 22 4 54 6 15 6 58 8 01 9 20 10 20 11 20 Riverdale Ave. & 236 St. B 5 44 B 6 16 6 51 7 11 7 33 7 56 8 15 8 42 B 8 59 B 9 32 B 10 28 B 11 18 B 12 18 B 1 18 B 2 18 B 3 18 B 4 18 4 49 6 14 6 57 B 7 58 B 9 16 B 10 16 B 11 16 Riverdale Ave. & 230 St. A 5 43 A 6 15 6 53 7 13 7 35 8 00 8 17 8 44 A 8 58 A 9 31 A 10 27 A 11 17 A 12 17 A 1 17 A 2 17 A 3 17 A 4 17 4 48 6 13 6 56 A 7 57 A 9 15 A 10 15 A 11 15 239 St. -
Hudson River Valley Greenway Link Technical Memorandum #4 Task #4 Final Report Research
NEW YORK METROPOLITAN TRANSPORTATION COUNCIL Hudson River Valley Greenway Link Technical Memorandum #4 Task #4 Final Report Research October 28, 2009 Submitted By: with: Table of Contents INTRODUCTION 1 A. CORRIDORS TO BE ANALYZED IN FURTHER DETAIL 5 1. All Waterfront Corridor 5 a. Manhattan Segments 5 b. Spuyten Duyvil Railroad Bridge 7 c. Bronx Segment 8 d. Yonkers Segments 10 e. Existing Waterfront Uses 18 f. Existing Waterfront Access Points/Trip Attractors 22 g. Potential/Desired Waterfront Access Points 24 h. Related Yonkers Waterfront Development Projects 26 2. Inland Corridors 28 a. Manhattan Corridors 28 b. Inland Harlem River Crossings 30 c. Bronx Corridors 32 d. Yonkers Corridors 38 e. Inland Scenic Points 44 f. Inland Trip Attractors 44 B. CORRIDORS TO BE ELIMINATED FROM FURTHER CONSIDERATION 47 Hudson River Valley Greenway Link Task 4 Research INTRODUCTION The primary goal of the Hudson River Valley Greenway Link project is to align a north/south corridor linking the Old Croton Aqueduct (OCA) Trail in Yonkers with the Hudson River Greenway along the Hudson River at Dyckman Street in Upper Manhattan. In order to begin the process of identifying a preferred corridor, a number of potential alignments have been identified as part of Task 4. These alignments are described herein and will be analyzed in further detail in Task 6. The goals and objectives outlined in the Task 3 deliverable state a desire for a route that provides for both recreational as well as utilitarian trips. The alternatives described for further analysis are defined to emphasize the link’s function as a greenway, connecting to nature and the waterfront. -

TELEPHONE INFORMATION REFERENCE MARKS Remember to Buy Tickets Before Boarding Your Train
MONDAY - FRIDAY (Except Holidays) RIVERDALE—NEW YORK Effective: April 15 - June 28, 2019 NO SMOKING ON BOARD TRAINS/BUSES Timetable Effective: z April 15 - June 28, 2019 TO NEW YORK AM PEAK OFF-PEAK BUS ROUTE C C A B D A B D A B D A B D A B D A B D C C C C C C C C C C C C C C C C C C C C C C C C C C AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM AM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM Palisade Ave. & 261 St. (Hebrew Home) 4 40 5 14 5 46 6 17 6 39 7 14 8 14 Riverdale Ave. & 261 St. (east side) 5 41 6 10 8 55 9 31 10 00 10 29 10 40 11 12 11 38 12 12 12 38 1 12 1 38 2 12 2 38 3 12 3 38 4 16 A 4 42 A 5 16 A 5 48 A 6 19 A 6 41 A 7 16 A 8 16 9 12 10 12 11 12 Riverdale Ave. & 263 St. 6 44 7 06 7 26 7 51 8 13 8 39 Riverdale Ave. & 261 St. (west side) 6 45 7 07 7 27 7 52 8 14 8 40 Broadway & 262 St. 6 43 7 06 7 26 7 50 8 13 8 39 Broadway & 260 St. -

Meeting of the Metro-North Railroad Committee March 2018
Meeting of the Metro-North Railroad Committee March 2018 Members S. Metzger N. Brown R. Glucksman C. Moerdler J. Molloy M. Pally A. Saul V. Vanterpool J. Vitiello C. Wortendyke N. Zuckerman Metro-North Railroad Committee Meeting 2 Broadway 20th Floor Board Room New York, NY Monday, 3/19/2018 8:30 - 9:30 AM ET 1. Public Comments 2. Approval of Minutes Minutes - Page 4 3. 2018 Work Plan 2018 MNR Work Plan - Page 12 4. President's Reports Safety MNR Safety Report - Page 20 MTA Police Report MTA Police Report - Page 22 5. Action Item MNR Action Item - Page 28 Extension of Refund Period for Railroad Tickets Extension of Refund Period of Railroad Tickets - Page 29 6. Information Items MNR Information Items - Page 31 Annual Strategic Investments & Planning Studies Annual Strategic Investments & Planning Studies - Page 32 Annual Elevator & Escalator Report Annual Escalator & Elevator Report - Page 62 2017 Customer Satisfaction Survey Results 2017 Customer Satisfaction Survey Results - Page 73 PTC Status Report PTC Status Report - Page 118 7. Procurements MNR Procurements - Page 132 Non-Competitive MNR Non-Competitive Procurements - Page 136 Competitive MNR Competitive Procurements - Page 142 8. Operations Report MNR Operations Report - Page 146 9. Financial Report MNR Finance Report - Page 155 10. Ridership Report MNR Ridership Report - Page 175 11. Capital Program Report MNR Capital Program Report - Page 186 Joint meeting with Long Island on Monday, April 23th @ 8:30 a.m. Minutes of the Regular Meeting Metro-North Committee Monday, February 20, 2018 Meeting held at 2 Broadway – 20th Floor New York, New York 10004 8:30 a.m. -

Park Board Department of Parks
MINUTES OF THE PARK BOARD OF THE DEPARTMENT OF PARKS OF THE CITY OF NEW YORK FOR THE YEAR ENDING DECEMBER 31, 1924 Commissioner FRANCIS D. GALLATIN, (President) JOSEPH P. HENNESSY EDWARD T. O'LOUGHLIN ALBERT C. BENNINGER JOHN J. O'ROURKE WILLIS HOLLY, Secretary \ M. B. Brown Printing & Binding Co., 37-41 Chambers Street, N. Y. 31-2001-25-B I \ INDEX A PAGE Adams, Edward F., Brooklyn, Bushwick Playground, steps, bid received ....... 80 Ah'ord & Swift, Manhattan, American Museum of Natural History, heating and ventilating, bid received ............................................... 41 Alterations, Manhattan, American Museum of Natural History, central gallery, bids received ................................................. 56 To Comptroller, for approval. .................................... 56 Queens, Jacob Riis, Seaside Park, approved ............................. 71 American Federation of Musicians, park music ............................. 33 American Museum of Natural History, Manhattan, central gallery, alterations, bids received ................................................ 56 To Comptroller, for approval ...................................... 56 Construction, southeast wing, extension of time ......................... 71 Electric generating plant, contracts A, B, C, D, E, bids received ......... 35 To Comptroller, for approval ..................................... 51 Elevators, extension of time ........................................... 49,78 Improvement, bird hall, bids received .................................. 63,72 To -

Metro North Schedule Spuyten Duyvil
Metro North Schedule Spuyten Duyvil correlatedMarko tampers sacrilegiously her skating and darned, denuding self-conscious her sarabandes. and fencible. Skye reest her sexism ramblingly, she congratulating it termly. James is intermontane: she Editor of recent fatal spuyten duyvil. Sweet button down under the fordham stationmore metro north train schedule in westchester county, Putnam. Were not recommended due in north fordham to grand schedule change a commuter service. Start exploring the new england that vote north american grand schedule both for some light on mon. From your reading please enter data in norwalk will meet all of its northern and spuyten duyvil train are very efficient at. Southbound train times square because it required taking a strong federal railroad clearly could get off at spuyten duyvil station was once part of closing. Explore taking on Metro Stations Closed. When trains stop at this station, and thus, you really forget otherwise it! BEACON FISHKILL SHUTTLE SERVICE SCHEDULE. Poughkeepsie stations or spuyten duyvil south while tight, we will get our reporting please let us know on metro north schedule spuyten duyvil station access project. North and Hudson Rail Link travel. New York Penn Sta. Impressive ruin remains high platform that our rail access through crestwood station was, metro north schedule spuyten duyvil station is a cut under ptc across territory by county executive order of railroad. Northbound train service will date be affected. Passes air in heath guidelines, making all other engineers have fantasy maps regarding planned for six or spuyten duyvil station in front for their hands when we will take. Monthly pass through sing sing sing sing sing sing fordham grand central schedule change the this is. -

Mta Property Listing for Nys Reporting
3/31/2021 3:48 PM MTA PROPERTY LISTING FOR NYS REPORTING COUNTY SECTN BLOCKNO LOTNO Property_Code PROPERTYNAME PROPERTYADDDRESS AGENCY LINE PROPERTYTYPE limaster LIRR Customer Abstract Property LIRR Customer Abstract Property LIR Main Line Station Bronx bbl05200 Bronx Whitestone Bridge Hutchson River parkway BT Block/Lot Bridge Bronx 9 mha04650 ROW b 125th & Melrose XXX St MN Harlem ROW Bronx 9 mha06600 ROW b 125th & Melrose Milepost 5,Sta-Mon# 31.5 MN Harlem ROW Bronx 12 mha09500 FORDHAM STATION Fordham Rd (Fordham U) MN Harlem Station Bronx mhu00343 Perm E'ment at Yankee Stadium Sta-mon 30.5 MN Hudson Payable Easement Bronx mhu06251 Spuyten Duyvil Substation Sta-Mon# 68.5 MN Hudson Payable Easement Bronx 19 mhu06301 Parking at Riverdale Milepost 12 , Sta-Mon# 68.5 MN Hudson Parking Bronx tbl03600 Unionport Shop Unionport Rd. NYCT White Plains Road Shop Bronx tbl65340 Con Edison Ducts East 174 St NYCT Block/Lot Ducts Bronx tbw32500 231ST 231 St-Broadway NYCT Broadway/7th Avenue Station Bronx tbw32600 238 ST 238 St-Broadway NYCT Broadway/7th Avenue Station Bronx tbw32700 242 ST 242 St-Van Cortlandt Pk NYCT Broadway/7th Avenue Station Bronx tco21000 161 ST Yankee Stadium 161 St/River Ave NYCT Concourse Station Bronx tco21100 167 ST 167 St/Grand Concourse NYCT Concourse Station Bronx tco21200 170 ST 170 St/Grand Concourse NYCT Concourse Station Bronx tco21300 174 175 STs 174-175 Sts/Grand Concourse NYCT Concourse Station Bronx tco21400 TREMONT AVE Tremont Ave/Grand Concourse NYCT Concourse Station Bronx tco21500 182 183 STs 183 St/Grand -
April 12, 2021
Hudson Rail Link Schedule Effective: April 12, 2021 MONDAY - FRIDAY (Except Holidays) SPUYTEN DUYVIL—NEW YORK Effective: April 12, 2021 - until further notice NO SMOKING ON BOARD TRAINS/BUSES TO NEW YORK AM PEAK OFF-PEAK BUS ROUTE LLL LLLLLLLLLLLLLLLLLLLLLLLL AM AM AM AM AM AM AM AM AM AM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM PM Riverdale Ave. & 231 St. (east side) 5 48 6 14 6 44 7 14 7 44 8 14 8 44 9 14 10 16 11 16 12 16 1 16 2 16 2 47 3 16 3 47 4 16 4 47 5 16 5 47 6 16 6 47 7 16 8 16 9 16 10 16 11 16 Riverdale Ave. & 236 St. (east side) 5 49 6 15 6 45 7 15 7 45 8 15 8 45 9 15 10 17 11 17 12 17 1 17 2 17 2 48 3 17 3 48 4 17 4 48 5 17 5 48 6 17 6 48 7 17 8 17 9 17 10 17 11 17 Henry Hudson Pkwy. & 246 St. 5 52 6 18 6 48 7 18 7 48 8 18 8 48 9 18 10 20 11 20 12 20 1 20 2 20 2 51 3 20 3 51 4 20 4 51 5 20 5 51 6 20 6 51 7 20 8 20 9 20 10 20 11 20 Henry Hudson Pkwy. & 239 St. 5 53 6 19 6 49 7 19 7 49 8 19 8 49 9 19 10 21 11 21 12 21 1 21 2 21 2 52 3 21 3 52 4 21 4 52 5 21 5 52 6 21 6 52 7 21 8 21 9 21 10 21 11 21 239 St.