Exploration of Near-Death Experience Accounts
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

|||GET||| a Dictionary for Dreamers 1St Edition
A DICTIONARY FOR DREAMERS 1ST EDITION DOWNLOAD FREE Tom Chetwynd | 9781351695961 | | | | | ISBN 13: 9780446798259 Le Guin's book, The Lathe of Heaventhe protagonist finds that his "effective" dreams can retroactively change reality. Jung expanded on Freud's idea that dream content relates to the dreamer's unconscious desires. Tarnow's theory is a reworking of Freud's theory of dreams in which Freud's unconscious is replaced with the long-term memory system and Freud's A Dictionary for Dreamers 1st edition Work" describes the structure of long-term memory. Tom Chetwynd has isolated for the first time the rich meanings of over archetypal symbols from the indiscriminate mass of dream material, and rated the likelihoods of the various possible interpretation in each case. During REM sleep, however, the communication between the neocortex and the hippocampus is disrupted by a high ACh level. Similarly, research scientistsmathematicians and physicists have developed new ideas by daydreaming about their subject areas. Amsterdam: John Benjamins. In A Dictionary for Dreamers 1st edition such as SpellboundThe Manchurian Candidateand Inceptionthe protagonists must extract vital clues from surreal dreams. The brain synthesizes and interprets these activities; for example, changes in the physical environment such as temperature and humidity, or physical stimuli such as ejaculation, and attempts to create meaning from these signals, result in dreaming. Those that appear adaptive are retained, while those that appear maladaptive are culled. The activation-synthesis theory hypothesizes that the peculiar nature of dreams is attributed to certain parts of the brain trying to piece together a story out of what is essentially bizarre information. -

Exploring the Effects of Galantamine Paired with Meditation and Dream
Consciousness and Cognition 63 (2018) 74–88 Contents lists available at ScienceDirect Consciousness and Cognition journal homepage: www.elsevier.com/locate/concog Full Length Article Exploring the effects of galantamine paired with meditation and dream reliving on recalled dreams: Toward an integrated protocol T for lucid dream induction and nightmare resolution ⁎ Gregory Sparrowa, , Ryan Hurdb, Ralph Carlsonc, Ana Molinac a Dept. of Counseling, University of Texas Rio Grande Valley, 1201 W. University Dr., Edinburg, TX 78539, United States b Dept. of Psychology, John F. Kennedy University, Orinda, CA, United States c Dept. of Educational Psychology, 1201 W. University Dr., University of Texas Rio Grande Valley, Edinburg, TX 78539, United States ARTICLE INFO ABSTRACT Keywords: An experimental home study examined the impact of a pre-sleep protocol for enhancing self- Lucid dream awareness, lucidity, and responsiveness in dreams. It included ingesting the cholinesterase in- Trauma resolution hibitor galantamine––which is widely reported to increase the frequency of lucid dreaming––- Meditation prior to engaging in middle-of-the-night meditation and the imaginary reliving of a distressing Dream reliving dream while exercising new responses. Thirty-five participants completed an eight-night study, Galantamine which included pre- and post-baseline nights and six conditions: waking for 40 min before re- turning to bed, called Wake-Back-to-Bed (WBTB); Wake-Back-to-Bed plus placebo (WBTB + P); Wake-Back-to-Bed plus galantamine (WBTB + G); meditation and dream reliving (MDR); medi- tation and dream reliving plus placebo (MDR + P); and meditation and dream reliving plus galantamine (MDR + G). The outcome measures included lucidity, reflectiveness, interactive behavior, role change, constructive action, and fear and threat, as measured by the participants’ self-ratings. -

Long-Read Transcriptome and Other Genomic Resources for the Angiosperm Silene Noctiflora
bioRxiv preprint doi: https://doi.org/10.1101/2020.08.09.243378; this version posted August 10, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Long-read transcriptome and other genomic resources for the angiosperm Silene noctiflora Alissa M. Williams,*,1 Michael W. Itgen,* Amanda K. Broz,* Olivia G. Carter,* Daniel B. Sloan* *Department of Biology, Colorado State University, Fort Collins, Colorado 80523 1Corresponding author: [email protected] bioRxiv preprint doi: https://doi.org/10.1101/2020.08.09.243378; this version posted August 10, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 Abstract 2 3 The angiosperm genus Silene is a model system for several traits of ecological and evolutionary 4 significance in plants, including breeding system and sex chromosome evolution, host-pathogen 5 interactions, invasive species biology, heavy metal tolerance, and cytonuclear interactions. 6 Despite its importance, genomic resources for this large genus of approximately 850 species are 7 scarce, with only one published whole-genome sequence (from the dioecious species S. latifolia). 8 Here, we provide genomic and transcriptomic resources for a hermaphroditic representative of 9 this genus (S. noctiflora), including a PacBio Iso-Seq transcriptome, which uses long-read, 10 single-molecule sequencing technology to analyze full-length mRNA transcripts and identify 11 paralogous genes and alternatively spliced genes. -

A Phenomenological Analysis of the Subjective Experience Elicited by Ibogaine in the Context of a Drug Dependence Treatment
ORIGINAL ARTICLE Journal of Psychedelic Studies 1(2), pp. 74–83 (2017) DOI: 10.1556/2054.01.2017.007 First published online August 25, 2017 A phenomenological analysis of the subjective experience elicited by ibogaine in the context of a drug dependence treatment EDUARDO EKMAN SCHENBERG1*, MARIA ANGÉLICA DE CASTRO COMIS1, JOÃO FELIPE MOREL ALEXANDRE2, LUÍS FERNANDO TÓFOLI3, BRUNO DANIEL RASMUSSEN CHAVES1 and DARTIU XAVIER DA SILVEIRA4 1Instituto Plantando Consciência, São Paulo, Brazil 2Centro de Matemática, Computação e Cognição, Universidade Federal do ABC (UFABC), Santo André, Brazil 3Faculdade de Ciências Médicas, Universidade Estadual de Campinas (UNICAMP), Campinas, Brazil 4Departamento de Psiquiatria, Universidade Federal de São Paulo (UNIFESP), São Paulo, Brazil (Received: September 5, 2016; accepted: June 22, 2017) Objective: This report documents the phenomenology of the subjective experiences of 22 patients with substance- related disorders who were involved in a treatment combining cognitive–behavioral therapy and hospital sessions with ibogaine in Brazil. Methods: Participants underwent a one-to-one semi-structured interview exploring the subjective effects of ibogaine. We employed interpretative phenomenological analysis to identify relevant phenomenological categories, including physical sensations, perceptual (visual, auditory, and olfactory), emotional, cognitive, and spiritual. Participants also compared ibogaine with other drugs used in life, including psychedelics like ayahuasca, psilocybin mushrooms, and lysergic acid diethylamide. Results: The findings reveal that the subjective experience with ibogaine has similarities with other psychedelic substances, but also important differences. These include very strong and unpleasant physical effects as well as, at least in this patient population, a very difficult and challenging experience. Conclusions: Overall, the descriptions involve heightened memory retrieval, specially related to drug abuse and the perception of one’s own future with or without drug use. -

The Experience Elicited by Hallucinogens Presents the Highest Similarity to Dreaming Within a Large Database of Psychoactive Substance Reports
ORIGINAL RESEARCH published: 22 January 2018 doi: 10.3389/fnins.2018.00007 The Experience Elicited by Hallucinogens Presents the Highest Similarity to Dreaming within a Large Database of Psychoactive Substance Reports Camila Sanz 1, Federico Zamberlan 1, Earth Erowid 2, Fire Erowid 2 and Enzo Tagliazucchi 1,3* 1 Departamento de Física, Universidad de Buenos Aires, Buenos Aires, Argentina, 2 Erowid Center, Grass Valley, CA, United States, 3 Brain and Spine Institute, Paris, France Ever since the modern rediscovery of psychedelic substances by Western society, Edited by: several authors have independently proposed that their effects bear a high resemblance Rick Strassman, to the dreams and dreamlike experiences occurring naturally during the sleep-wake University of New Mexico School of cycle. Recent studies in humans have provided neurophysiological evidence supporting Medicine, United States this hypothesis. However, a rigorous comparative analysis of the phenomenology (“what Reviewed by: Matthias E. Liechti, it feels like” to experience these states) is currently lacking. We investigated the semantic University Hospital Basel, Switzerland similarity between a large number of subjective reports of psychoactive substances and Michael Kometer, University of Zurich, Switzerland reports of high/low lucidity dreams, and found that the highest-ranking substance in *Correspondence: terms of the similarity to high lucidity dreams was the serotonergic psychedelic lysergic Enzo Tagliazucchi acid diethylamide (LSD), whereas the highest-ranking in terms of the similarity to dreams [email protected] of low lucidity were plants of the Datura genus, rich in deliriant tropane alkaloids. Specialty section: Conversely, sedatives, stimulants, antipsychotics, and antidepressants comprised most This article was submitted to of the lowest-ranking substances. -

Molecular and Functional Imaging Studies of Psychedelic Drug Action in Animals and Humans
molecules Review Molecular and Functional Imaging Studies of Psychedelic Drug Action in Animals and Humans Paul Cumming 1,2,* , Milan Scheidegger 3 , Dario Dornbierer 3, Mikael Palner 4,5,6 , Boris B. Quednow 3,7 and Chantal Martin-Soelch 8 1 Department of Nuclear Medicine, Bern University Hospital, CH-3010 Bern, Switzerland 2 School of Psychology and Counselling, Queensland University of Technology, Brisbane 4059, Australia 3 Department of Psychiatry, Psychotherapy and Psychosomatics, Psychiatric Hospital of the University of Zurich, CH-8032 Zurich, Switzerland; [email protected] (M.S.); [email protected] (D.D.); [email protected] (B.B.Q.) 4 Odense Department of Clinical Research, University of Southern Denmark, DK-5000 Odense, Denmark; [email protected] 5 Department of Nuclear Medicine, Odense University Hospital, DK-5000 Odense, Denmark 6 Neurobiology Research Unit, Copenhagen University Hospital, DK-2100 Copenhagen, Denmark 7 Neuroscience Center Zurich, University of Zurich and Swiss Federal Institute of Technology Zurich, CH-8058 Zurich, Switzerland 8 Department of Psychology, University of Fribourg, CH-1700 Fribourg, Switzerland; [email protected] * Correspondence: [email protected] or [email protected] Abstract: Hallucinogens are a loosely defined group of compounds including LSD, N,N- dimethyltryptamines, mescaline, psilocybin/psilocin, and 2,5-dimethoxy-4-methamphetamine (DOM), Citation: Cumming, P.; Scheidegger, which can evoke intense visual and emotional experiences. We are witnessing a renaissance of re- M.; Dornbierer, D.; Palner, M.; search interest in hallucinogens, driven by increasing awareness of their psychotherapeutic potential. Quednow, B.B.; Martin-Soelch, C. As such, we now present a narrative review of the literature on hallucinogen binding in vitro and Molecular and Functional Imaging ex vivo, and the various molecular imaging studies with positron emission tomography (PET) or Studies of Psychedelic Drug Action in single photon emission computer tomography (SPECT). -

Saatgut Vom Natürlichen Standort/Seeds From
Index Seminum 2016 ANNO 2016 COLLECTORUM - DESIDERATA 2017 Botanischer Garten Universität Duisburg-Essen ** = Saatgut vom natürlichen Standort / seeds from natural habitat, all other seeds from open pollination (hybridization possible) Acanthaceae 1. Acanthus spinosus L. 2. Andrographis paniculata (Burm.f.) Nees 3. Schaueria flavicoma N.E.Br. 4. Thunbergia alata Bojer ex Sims Adoxaceae 5. Viburnum rhytidophyllum Hemsl. Amaranthaceae 6. Chenopodium bonus-henricus L. Amaryllidaceae 7. Agapanthus campanulatus 8. Allium cernuum Roth 9. Allium fistulosum L. 10. Allium obliquum L. 11. Allium sativum L. var. ophioscorodon 12. Allium schoenoprasum L. 13. Allium sphaerocephalon L. 14. Allium tuberosum Rottler ex Spreng. 15. Allium ursinum L. 16. Clivia miniata (Lindl.) Bosse 17. Tulbaghia simmleri Beauverd 18. Tulbaghia violacea Harv. Annonaceae 19. Annona muricata L. 20. Annona cherimola, Kulturform 21. Artabotrys hexapetalus (L.f.) Bhandari Apiaceae 22. Ammi majus L. 23. Angelica archangelica L. 24. Angelica sylvestris L. 25. Anthriscus cerefolium (L.) Hoffm. 26. Apium graveolens L. 27. Astrantia carniolica Wulfen 1 28. Astrantia major L. 29. Athamanta cretensis L. 30. Bupleurum rotundifolium L. 31. Carum carvi L. 32. Coriandrum sativum L. 33. Daucus carota L. 34. Eryngium campestre L. 35. Eryngium foetidum L. 36. Foeniculum vulgare Mill. 37. Foeniculum vulgare Mill. ‚Purpureum‘ 38. Levisticum officinale W.D.J.Koch 39. Ligusticum lucidum Mill 40. Ligusticum scoticum L. 41. Mutellina adonidifolia (J.Gay) Gutermann 42. Myrrhis odorata Scop. 43. Oenanthe lachenalii C.C.Gmel. 44. Oenanthe pimpinelloides L. 45. Pimpinella saxifraga L. 46. Sanicula europaea L. 47. Scandix pecten-veneris L. 48. Sium sisarum L. 49. Torilis japonica (Houtt.) DC Apocynaceae 50. Acokanthera oblongifolia (Hochst.) Benth. -
Conscious Dreaming and Controlled Hallucinations
Conscious Dreaming and Controlled Hallucinations Claude de Contrecoeur ([email protected]) This work is dedicated to my cherished Hiroé Aquasaca, from Kasoukabé, Tôquiô, who gave me the inspiration to share it with other exoreal people. Had I not met her, you would very probably not be reading this study! It is also dedicated to another cherished Chinese girlfriend of mine: Patanîe Pongpatchamnanouàte from Souqsaouate, Bângkoc (this work is also dedicated to my dear friend Cyrano de Bergerac, a brillant Hiroé Aquasaca thinker of the 17th century). Both are my Patanîe Pongpatchamnanouàte inspiration to inform you about this important work. What we call Amour (love) is an extraordinary hallucination, and from such beautiful hallucinations things can be born into the exogenous reality ... like what you are going to read. Alors chères Patanîe et Hiroé un jour vous ferez partie de l'Histoire! For whoever authentically knows about Conscious Dreams, money, glory, recognition and similar bla, bla, bla are nonsense! This is the main reason why I did not bother to put my work into a book (as Dr A.Hobson from Harvard repeatedly suggested to me!). Maybe this will be done in the future if people manifest their interest in this topic. Otherwise? There's no use in me wasting my time if only a few people are interested! Reading this, you will clearly understand why!! ● Conscious dreams ● How to achieve conscious dreams ● MHVs are like tunnels linking MCV boxes! ● The new alphabetisation of mankind ● There are two ways to penetrate a conscious dream ● What to do in a conscious dream ● About different states of consciousness and "new" concepts ● Different states of consciousness are generated via the mutual interactions of the attenuator, DRP and SBEM ● Why does dreaming exist? ● Oneiric Maps (Les Cartes oniriques) ● What is the rôle of DMT in the CNS? ● Continuity and discontinuity of consciousness ● The illusioned consciousness: towards an understanding of consciousness ● Déjà Vu is the lowest state of Illusion ● When a Naked Woman becomes transformed into a Banana.. -

The Nightmare Free
FREE THE NIGHTMARE PDF lars Kepler | 608 pages | 03 Jan 2013 | HarperCollins Publishers | 9780007414505 | English | London, United Kingdom The Nightmare - Wikipedia The Nightmare By Henry Fuseli. Regarded as one of the The Nightmare Paintings Ever. For the meaning of other celebrated masterpieces, please see: Famous Paintings Analyzed One of the most innovative Romantic artists of his day, the Swiss-born Johann Heinrich Henry Fuseli - son of the The Nightmare Johann Caspar Fussli - developed an early talent for drawing before moving to London The Nightmare at the age of Here, encouraged by Joshua Reynolds who was shortly to be elected the first president of the newly formed Royal Academy of ArtsFuseli took up painting. This led him to spend most of the s in Italy, studying the figure painting of Michelangelo which became a major influence on his art. Other influences included 16th-century Mannerism and literary sources, notably Shakespeare. Later appointed a professor of painting at the Royal Academy, he became one of the best English painters of the eighteenth century and was buried in St Paul's Cathedral. Like his The Nightmare contemporary William BlakeFuseli's strength as a painter lies in his imaginative intensity, and The Nightmare - which he sold for 20 guineas - remains his greatest and most baffling masterpiece. Overlooked after his death, Fuseli was 'rediscovered' by 20th-century Expressionists and Surrealists who greatly admired his creativity. Painted shortly after his return from Italy, The Nightmare was first shown to the public in The Nightmare the annual exhibition of the Royal Academy. An instant success, it established Fuseli's reputation as one of the most creative artists in London. -
Colour Pages
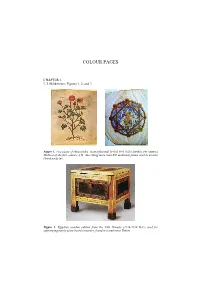
COLOUR PAGES CHAPTER 1. L.J. Slikkerveer; Figures 1, 2, and 3 Figure 1. Two pages of Dioscorides’ most influential herbal Peri Hylès latrikès (De Materia Medica) of the first century A.D., describing more than 600 medicinal plants used in ancient Greek medicine Figure 2. Egyptian wooden cabinet from the 20th Dynasty (1126-1108 B.C.) used for safekeeping mostly plant-based cosmetics, found in a tomb near Thebes Figure 3. Evolution of the methods of botanical investigation, as represented from left to right by Leonard Fuchs’s sketch of the thorn apple (Datura stramonium) of 1543; Köhlers more detailed pharmacognostic illustration of this plant in his Medizinal-Pflanzenatlas Vol. I of 1887; a recent typical herbarium specimen of botanical identification of the plant; and a detailed image of the leaf surface provided by an electron-scanning microscope CHAPTER 3. K.F. Wiersum, A.P. Dold, M. Husselman and M. Cocks; Figure 2. Figure 2. Homegarden cultivation of medicinal plants (Silene undulata–unozitholana) Photo: A. Dold COLOUR PAGES CHAPTER 4. T. Flaster; Figure 1. Figure 1. Market visit image CHAPTER 5. A. Brown; Figures 1 and 2. Regional Markets markets outside the region Wholesale Markets Exporter Consumers Branded in the processors National Capital District Traders Small District Processors Town Consumers Centre Heads (Agents) Local Traders Local Consumers Village Level Processor Farmers, collectors, and farm level pre-processors (e.g sorting and drying) Figure 1. The MAP marketing system Regional Markets markets outside the region Wholesale Markets Exporter Consumers Branded in the processors National Capital District Traders Small District Processors Town Consumers Centre Heads (Agents) Local Traders Local Consumers Village Level Processor Farmers, collectors, and farm level pre-processors (e.g sorting and drying) Figure 2. -

Colour Pages
COLOUR PAGES CHAPTER 1. L.J. Slikkerveer; Figures 1, 2, and 3 Figure 1. Two pages of Dioscorides’ most influential herbal Peri Hylès Iatrikès (De Materia Medica) of the first century A.D., describing more than 600 medicinal plants used in ancient Greek medicine Figure 2. Egyptian wooden cabinet from the 20th Dynasty (1126-1108 B.C.) used for safekeeping mostly plant-based cosmetics, found in a tomb near Thebes Figure 3. Evolution of the methods of botanical investigation, as represented from left to right by Leonard Fuchs’s sketch of the thorn apple (Datura stramonium) of 1543; Köhlers more detailed pharmacognostic illustration of this plant in his Medizinal-Pflanzenatlas Vol. I of 1887; a recent typical herbarium specimen of botanical identification of the plant; and a detailed image of the leaf surface provided by an electron-scanning microscope CHAPTER 3. K.F. Wiersum, A.P. Dold, M. Husselman and M. Cocks; Figure 2. Figure 2. Homegarden cultivation of medicinal plants (Silene undulata–unozitholana) Photo: A. Dold COLOUR PAGES CHAPTER 4. T. Flaster; Figure 1. Figure 1. Market visit image CHAPTER 5. A. Brown; Figures 1 and 2. Regional Markets markets outside the region Wholesale Markets Exporter Consumers Branded in the processors National Capital District Traders Small District Processors Town Consumers Centre Heads (Agents) Local Traders Local Consumers Village Level Processor Farmers, collectors, and farm level pre-processors (e.g sorting and drying) Figure 1. The MAP marketing system Regional Markets markets outside the region Wholesale Markets Exporter Consumers Branded in the processors National Capital District Traders Small District Processors Town Consumers Centre Heads (Agents) Local Traders Local Consumers Village Level Processor Farmers, collectors, and farm level pre-processors (e.g sorting and drying) Figure 2. -

Hallucinogens As Treatment? Preliminary Data with Ketamine
Hallucinogens as Treatment? Preliminary Data with Ketamine Elias Dakwar, MD Columbia University College of Physicians and Surgeons 19 October, 2017 Disclosures Elias Dakwar has received funding from NIDA and NIAAA. He has no conflicts of interest to report. Overview How might hallucinogens work as treatment? Why might ketamine work as a treatment? By any other name Deliriant Entheogen Hallucinogen Imaginant Oneirogen Phanarothyme Phantasticant Psychedelic Psychotomimetic A diverse group Indoles - d-lysergic-acid (LSD), dimethyltryptamine (DMT), harmaline, ibogaine, psilocybin, Dissociative Anesthetics - ketamine, PCP Phenethylamines -mescaline, 2-CB, DOM, MDA, MDMA Others - nitrous oxide, salvia divinorum, THC, fly agaric mushroom Effects Produce in a time-limited manner non-ordinary experiences comparable to: trance psychosis ecstasy dreaming mystical experience Ancient Uses Ritual Divination Initiation Pleasure Healing Witchcraft Protection/fortification Modern Uses Classical hallucinogens were investigated in the 1950s through the early ’70s in various settings. psychiatric treatment quality of life improvement investigations of consciousness criminal justice warfare “Psychedelic” and “Psycholytic” treatment models Concern over recreational use obscured promising clinical data and clinical research was largely aborted due to criminalization in 1973. But has recently resumed via private foundation funding Set and Setting A valuable heuristic for optimizing benefits, minimizing risks Set: the recipient’s expectations, past experiences,