Research Article
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
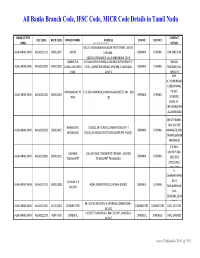
Banks Branch Code, IFSC Code, MICR Code Details in Tamil Nadu
All Banks Branch Code, IFSC Code, MICR Code Details in Tamil Nadu NAME OF THE CONTACT IFSC CODE MICR CODE BRANCH NAME ADDRESS CENTRE DISTRICT BANK www.Padasalai.Net DETAILS NO.19, PADMANABHA NAGAR FIRST STREET, ADYAR, ALLAHABAD BANK ALLA0211103 600010007 ADYAR CHENNAI - CHENNAI CHENNAI 044 24917036 600020,[email protected] AMBATTUR VIJAYALAKSHMIPURAM, 4A MURUGAPPA READY ST. BALRAJ, ALLAHABAD BANK ALLA0211909 600010012 VIJAYALAKSHMIPU EXTN., AMBATTUR VENKATAPURAM, TAMILNADU CHENNAI CHENNAI SHANKAR,044- RAM 600053 28546272 SHRI. N.CHANDRAMO ULEESWARAN, ANNANAGAR,CHE E-4, 3RD MAIN ROAD,ANNANAGAR (WEST),PIN - 600 PH NO : ALLAHABAD BANK ALLA0211042 600010004 CHENNAI CHENNAI NNAI 102 26263882, EMAIL ID : CHEANNA@CHE .ALLAHABADBA NK.CO.IN MR.ATHIRAMIL AKU K (CHIEF BANGALORE 1540/22,39 E-CROSS,22 MAIN ROAD,4TH T ALLAHABAD BANK ALLA0211819 560010005 CHENNAI CHENNAI MANAGER), MR. JAYANAGAR BLOCK,JAYANAGAR DIST-BANGLAORE,PIN- 560041 SWAINE(SENIOR MANAGER) C N RAVI, CHENNAI 144 GA ROAD,TONDIARPET CHENNAI - 600 081 MURTHY,044- ALLAHABAD BANK ALLA0211881 600010011 CHENNAI CHENNAI TONDIARPET TONDIARPET TAMILNADU 28522093 /28513081 / 28411083 S. SWAMINATHAN CHENNAI V P ,DR. K. ALLAHABAD BANK ALLA0211291 600010008 40/41,MOUNT ROAD,CHENNAI-600002 CHENNAI CHENNAI COLONY TAMINARASAN, 044- 28585641,2854 9262 98, MECRICAR ROAD, R.S.PURAM, COIMBATORE - ALLAHABAD BANK ALLA0210384 641010002 COIIMBATORE COIMBATORE COIMBOTORE 0422 2472333 641002 H1/H2 57 MAIN ROAD, RM COLONY , DINDIGUL- ALLAHABAD BANK ALLA0212319 NON MICR DINDIGUL DINDIGUL DINDIGUL -

Tamil Nadu Government Gazette
© [Regd. No. TN/CCN/467/2012-14. GOVERNMENT OF TAMIL NADU [R. Dis. No. 197/2009. 2013 [Price: Rs. 54.80 Paise. TAMIL NADU GOVERNMENT GAZETTE PUBLISHED BY AUTHORITY No. 41] CHENNAI, WEDNESDAY, OCTOBER 23, 2013 Aippasi 6, Vijaya, Thiruvalluvar Aandu–2044 Part VI—Section 4 Advertisements by private individuals and private institutions CONTENTS PRIVATE ADVERTISEMENTS Pages Change of Names .. 2893-3026 Notice .. 3026-3028 NOTICE NO LEGAL RESPONSIBILITY IS ACCEPTED FOR THE PUBLICATION OF ADVERTISEMENTS REGARDING CHANGE OF NAME IN THE TAMIL NADU GOVERNMENT GAZETTE. PERSONS NOTIFYING THE CHANGES WILL REMAIN SOLELY RESPONSIBLE FOR THE LEGAL CONSEQUENCES AND ALSO FOR ANY OTHER MISREPRESENTATION, ETC. (By Order) Director of Stationery and Printing. CHANGE OF NAMES 43888. My son, D. Ramkumar, born on 21st October 1997 43891. My son, S. Antony Thommai Anslam, born on (native district: Madurai), residing at No. 4/81C, Lakshmi 20th March 1999 (native district: Thoothukkudi), residing at Mill, West Colony, Kovilpatti, Thoothukkudi-628 502, shall Old No. 91/2, New No. 122, S.S. Manickapuram, Thoothukkudi henceforth be known as D. RAAMKUMAR. Town and Taluk, Thoothukkudi-628 001, shall henceforth be G. DHAMODARACHAMY. known as S. ANSLAM. Thoothukkudi, 7th October 2013. (Father.) M. v¯ð¡. Thoothukkudi, 7th October 2013. (Father.) 43889. I, S. Salma Banu, wife of Thiru S. Shahul Hameed, born on 13th September 1975 (native district: Mumbai), 43892. My son, G. Sanjay Somasundaram, born residing at No. 184/16, North Car Street, on 4th July 1997 (native district: Theni), residing Vickiramasingapuram, Tirunelveli-627 425, shall henceforth at No. 1/190-1, Vasu Nagar 1st Street, Bank be known as S SALMA. -

Project Director, DRDA, Tiruvarur Inviting Bids Under NABARD XX E
Project Director, DRDA, Tiruvarur inviting Bids under NABARD XX RIDF/2014-15 e-Procurement Notice INVITATION FOR BIDS (IFB) 1. The Project Director, DRDA, Tiruvarur on behalf of the Governor of Tamil Nadu invites the item rate bids, in electronic tendering system, for Construction of bridge and Strengthening of road under NABARD XX RIDF/2014- 15 for each of the following works the eligible and approved contractors registered with any of Tamil Nadu State Government Departments/undertakings like DRDAs / PWD / Highways Department / TNHB / TNSCB / TNPHC etc. Estimat Lengt e Name of the Package S.No Name of the Road h in Amount EMD Block number Km Rs(in lakhs) 1/NABARD XX Black topping to Namachivayapuram - 1 Tiruvarur 1.300 55.40 55400 /TVR/2014-15 Arukudi link road 2/NABARD XX 2 Nannilam Black topping to Ponnirai AD Colony Road 1.306 37.50 37500 /NLM/2014-15 3/NABARD XX 3 Kodavasal Ayyampettai - Kovilpathu road 2.550 76.78 76800 /KDL/2014-15 4/NABARD XX Black Topping to Pathur Melkarai - 4 Koradachery 1.510 27.90 27900 /KDY/2014-15 Panangarai in Viswanathapuram Pt 5/NABARD XX BlackTopping to Tholuvur. 5 Valangaiman 3.200 77.00 77000 /VLM/2014-15 Kulakudy,Sithanvalur Road Kanchikudikadu-Ambalakara street 6 1.800 39.50 0/0-1/8 Needamangal 6/NABARD XX am /NDM/2014-15 Sengal odai-Vadakku thoppu BT road 64400 7 1.350 24.85 KM0/0-1/35 Total 64.35 Strengthening to Savadikulam - 8 1.215 30.67 Sothiriyam road in Vettaithidal Panchayat 7/NABARD XX Mannargudi /MNG/2014-15 Strengthening to Keela Nemmeli road in 64400 9 2.000 33.65 29Nemmeli Panchayat -

THIRUVARUR (Tamil Nadu) Issued On: 02-10-2021
India Meteorological Department Ministry of Earth Sciences Govt. of India Date: 02-10-2021 Block Level Forecast Weather Forecast of KODAVASAL Block in THIRUVARUR (Tamil Nadu) Issued On: 02-10-2021 Wind Wind Cloud Date Rainfall Tmax Tmin RH Morning RH Evening Speed Direction Cover (Y-M-D) (mm) (°C) (°C) (%) (%) (kmph) (°) (Octa) 2021-10-03 4.4 31.5 23.9 85 53 9.0 79 2 2021-10-04 0.4 31.9 24.3 86 52 6.0 120 7 2021-10-05 10.8 33.6 24.4 84 50 6.0 113 7 2021-10-06 10.8 33.9 24.2 85 48 6.0 135 6 2021-10-07 22.8 33.4 23.9 87 51 12.0 195 8 Weather Forecast of KORADACHERRY Block in THIRUVARUR (Tamil Nadu) Issued On: 02-10-2021 Wind Wind Cloud Date Rainfall Tmax Tmin RH Morning RH Evening Speed Direction Cover (Y-M-D) (mm) (°C) (°C) (%) (%) (kmph) (°) (Octa) 2021-10-03 6.7 31.1 23.8 84 53 8.0 79 2 2021-10-04 0.3 31.9 24.4 84 50 5.0 135 7 2021-10-05 19.8 33.4 24.5 83 49 5.0 146 7 2021-10-06 18.2 33.9 24.2 84 49 6.0 135 6 2021-10-07 23.0 32.9 23.8 86 52 12.0 198 8 Weather Forecast of KOTTUR Block in THIRUVARUR (Tamil Nadu) Issued On: 02-10-2021 Wind Wind Cloud Date Rainfall Tmax Tmin RH Morning RH Evening Speed Direction Cover (Y-M-D) (mm) (°C) (°C) (%) (%) (kmph) (°) (Octa) 2021-10-03 0.8 31.6 24.1 82 52 10.0 79 1 2021-10-04 0.3 32.3 24.6 83 50 7.0 116 7 2021-10-05 15.9 33.6 24.6 82 49 7.0 113 6 2021-10-06 7.4 33.8 24.4 82 49 8.0 135 6 2021-10-07 18.4 33.4 24.0 85 51 14.0 195 8 India Meteorological Department Ministry of Earth Sciences Govt. -

Thiruvarur District
For official use Technical Report Series DISTRICT GROUNDWATER BROCHURE THIRUVARUR DISTRICT, TAMIL NADU By V. Dhinagaran, Scientist - D Government of India Ministry of Water Resources Central Ground Water Board South Eastern Coastal Region Chennai November 2008 DISTRICT AT A GLANCE (THIRUVARUR) S. No. ITEMS STATISTICS 1. GENERAL INFORMATION i. Geographical area (Sq. km.) 2097.97 ii. Administrative Divisions (As on 31-3-2007) 1. Number of Taluks 7 2. Number of Blocks 10 3. Number of Panchayats/Town Panchayats/Municipalities 10 / 7 / 4 4. Number of Villages 573 iii. Population (2001 Census) Total Population 1,169,474 Male 5,80,784 Female 5,88,690 1184 iv. Average Annual Rainfall (mm) (1901-2000) 2. GEOMORPHOLOGY i. Major physiographic Units 1. Deltaic plain, 2. Pediment and buried pediment 3. Natural levee- swale, 4. Lagoon/Backwater Coastal plain and 5. Beach and Beach ridges ii. Major Drainages Vennar and Vettar 3. LAND USE (Sq. km.) (2005-06) i. Forest area 24.52 ii. Net area sown 1532.27 iii. Cultivable waste 18.96 4. MAJOR SOIL TYPES Alluvial soil 5. AREA UNDER PRINCIPAL CROPS (Ha.) 1.Paddy –156098 (74.4%) (2005-06) 2. Oil seeds-9772 (4.6%) 3. Cocunut-5371 (26%) (Figures given in the bracket are % of Total 4. Sugarcane-3722 (2%) geographical area) 6. IRRIGATION BY DIFFERENT SOURCES Number Area irrigated (2005-06) (Ha.) i. Dug wells 31256 - ii. Tube wells 8 - iii. Tanks 34 - iv. Canals 13 147564 i v. Other Sources - - vi. Net irrigated area 147564 (Ha) vii. Gross irrigated area 165362 (Ha.) 7. NUMBER OF GROUND WATER MONITORING WELLS OF CGWB (As on 31.03.2007) i. -
THIRUVARUR DISTRICT EXECUTIVE SUMMARY DISTRICT HUMAN DEVELOPMENT REPORT THIRUVARUR DISTRICT Introduction
THIRUVARUR DISTRICT EXECUTIVE SUMMARY DISTRICT HUMAN DEVELOPMENT REPORT THIRUVARUR DISTRICT Introduction The old integrated Thanjavur district was trifurcated into three districts, namely, Thanjavur, Thiruvarur and Nagapattinam districts. GEOGRAPHY The district is situated between 10.200 and 11.070 of the Northern latitude. The district is bounded on the East and North by Nagapattinam district on the South by Palk Strait and on the west by Thanjavur district. Though Thanjavur, Thiruvarur and Nagapattinam districts are collectively called the Delta districts, Thiruvarur district is in the heart of the delta districts. The Cauvery is the chief river of the district, fostering agriculture and Tamil culture for ages together. It is a very small district with a total geographical area of 2097.09 Sq. Km. This constitutes just 1.6% of the area of the State. At present, this district comprises of seven revenue taluks viz., Thiruvarur, Kudavasal, Mannargudi, Needamangalam, 1 Thiruthuraipoondi, Nannilam and Valangaiman taluks and ten blocks of Thiruvarur, Nannilam, Koradachery, Kudavasal, Valangaiman, Needamangalam, Mannargudi, Kottur, Thiruthuraipoondi and Muthupettai. Out of the total geographical area of 2097.09 sq km, the net area under crop is 1,50,900 hectares. TOPOGRAPHY Thiruvarur can be divided into three regions from the topography and flora point of view. They are the alluvial regions land areas. The areas on the banks of rivers and canal in the form of narrow strips. The lateritic region: This region contains mostly thorny scrub jungles, tropical thorn forests and tropical dry evergreen forests. The coastal regions: This zone contains causurina plantations, mangrove scrub, mangrove forest and southern thorn scrub jungle. -

Coal Bed Methane (CBM) Underground Coal Gasification (UCG) DEVELOPMENTAL SCHEME for CBM and UCG
THIRD US-INDIA WORKING GROUP MEETING ON COAL CLEAN COAL TECHNOLOGY • Coal bed methane & • In-situ Coal Gasification To gainfully utilize the vast potential of lignite deposits which are uneconomical for conventional mining, the following non- conventional / Clean Coal technologies are considered. Coal Bed Methane (CBM) Underground Coal Gasification (UCG) DEVELOPMENTAL SCHEME FOR CBM AND UCG CBM PROJECT UCG PROJECT PRODUCTION WELL INJECTION WELL (AIR/OXYGEN) OVERBURDEN FORMATION LIGNITE GASIFICATION CHAMBER Extraction of product gas from Coal / Lignite beds by insitu Extraction of Methane by non conventional process from conversion process Coal / lignite beds Coal Bed Methane Underground Coal Gasification Methane adsorbed on coal matrix and in fracture/cleats • Syngas (Coal gas) is produced by partial • Product of Coalification burning of lignite insitu Biogenic & Thermogenic • Calorific Value 800 – 3000 Kcal/m³ 2-10M3/tonne of coal • Cheap source of energy Low Pressure 350 M³ per ton of lignite • Environmentally safe • Environmentally safe • Large Indian Reserves • 69% of known reserves are unmineable COAL BED METHANE • NLC started its endeavor to enter into the field of CBM in the year 2000. • Requested CMPDI to provide technical consultancy . • CMPDI submitted a proposal for undertaking consultancy. • NLC wrote to different consultants including US Embassy for consultancy –so far no reply received. • In Neyveli basin total available reserves of lignite for CBM development is 5500 MT. • Likely gas reserves is 8250 MCM. • Geological setup is similar to Powder River basin of USA • 2400 MT reserves are already in NLC’s leasehold. • Additionally 1000 MT in Jayamkondam is applied for lease • The above areas can be taken for immediate studies for exploitation of 5100 Mcum gas. -

2005- Journal 12Th Issue
JOURNAL OF INDIAN HISTORY AND CULTURE September 2005 Twelfth Issue C.P. RAMASWAMI AIYAR INSTITUTE OF INDOLOGICAL RESEARCH The C.P. Ramaswami Aiyar Foundation 1, Eldams Road, Alwarpet, Chennai 600 018, INDIA EDITOR Dr. G.J. Sudhakar EDITORIAL BOARD Dr. K.V.Raman Dr. T.K.Venkatasubramaniam Dr. R.Nagaswami Dr. Nanditha Krishna Published by C.P.Ramaswami Aiyar Institute of Indological Research The C.P. Ramaswami Aiyar Foundation 1, Eldams Road, Alwarpet, Chennai 600 018 Tel: 2434 1778 Fax: 91-44-24351022 E-Mail: [email protected] Website: www.cprfoundation.org Subscription Rs.95/- (for 2 issues) Rs.180/- (for 4 issues) CONTENTS Mahisha, The Buffalo Demon .................................................................... 7 Dr. Nanditha Krishna A Study of the Ramayana and Mahabharata .......................................... 11 Dr. S. Kuppusamy Secular and Religious Contribution of Performing Arts............................ 16 Dr. Prof. Mrs. V. Balambal Historiography of Professor K.A. Nilakanta Sastri ................................... 36 Dr. Shankar Goyal Female Functionaries of Medieval South Indian Temples........................ 51 Dr. S. Chandni Bi Society and Land Relation in the Kaveri Delta During the Chola Period A.d. 850–1300 ................................................................... 70 Mr. V. Palanichamy Note on Dutch Documents on Coastal Karnataka 1583–1763 .................. 81 Dr. K.G. Vasantha Madhava India Under the East India Company and the Transition to British Rule ... 85 Dr. Rukmini Nagarajan Kudikaval System in Madurai District ....................................................101 Dr. K.V. Jeyaraj and Mr. P. Jeganathan Articles of Trade, The System of Weights and Measures in Parlakhemundi Under the British Raj (A.d. 1858–1936): A Case Study of the Gajapati District.....................................................108 Dr. N.P. Panigrahi Indian Nationalism: Role of Cuddapah District in the Constructive Activities (1922–30) – A Micro Study ................................116 Dr. -
Land Suitability Assessment Using Remote Sensing and Geographical Information System in Mannargudi Block, South India
INTERNATIONAL JOURNAL OF SCIENTIFIC & TECHNOLOGY RESEARCH VOLUME 8, ISSUE 11, NOVEMBER 2019 ISSN 2277-8616 Land Suitability Assessment Using Remote Sensing And Geographical Information System In Mannargudi Block, South India S. Baskar, G.Kumar Abstract : Land suitability assessment is one of the important researches in agricultural practices. The main aim of the present study is to assess the crop land suitability for cultivation in Mannargudi block, Tamil Nadu, India using remote sensing and GIS applications. The land suitability parameters such as slope, land use / land cover, soil, geology, aspect and drainage density were selected. All these parameters determine the suitability of a given area for a particular type of crop cultivation. Further, all the parameters were integrated using weighted overlay analysis is available in ArcGIS software. The final suitability map was prepared and reclassified into five classes like very high suitable (18.28%), highly suitable (52.75%), moderately suitable (21.52), less suitable (6.49%) and not suitable (1.06%) in the study area. The results revealed that about 29.02% of the study area fall under moderately suitable to not suitable for cultivation which is immediate attention need for sustainable agricultural management in the study area. Index Terms: Land Suitability, Agricultural Crop, Cultivation, Weighted Overlay, South India. —————————— —————————— 1. INTRODUCTION land suitability classification process involves the evaluation When Agriculture is the most vital economic activity of man. It and grouping of a particular land area in terms of their is the main provider of substance for human being in India. suitability for a defined use (Prakash, 2003). Land suitability The country like India having predominance of agricultural analysis (LSA) is a method to encounter inherent and potential activity along with over population, it is necessary to give more capabilities (Bandyopadhyay et al., 2009).Crop-land suitability attention to spatial organization of agriculture. -

District Survey Report of Thiruvarur District
DISTRICT SURVEY REPORT OF THIRUVARUR DISTRICT DEPARTMENT OF GEOLOGY AND MINING THIRUVARUR DISTRICT 1 DISTRICT SURVEY REPORT- THIRUVARUR CONTENTS S.No Chapter Page No. 1.0 Introduction 1 2.0 Overview of Mining Activity in the District; 4 3.0 General profile of the district 4 4.0 Geology of the district; 9 5.0 Drainage of irrigation pattern 10 6.0 Land utilisation pattern in the district; Forest, Agricultural, 10 Horticultural, Mining etc 7.0 Surface water and ground water scenario of the district 11 8.0 Rainfall of the district and climate condition 11 9.0 Savudu/Earth - Details of the mining lease in the district as per 13 following format 10.0 Details of Royalty / Revenue received in the last three years 17 (2015-16 to 2017-18) 11.0 Details of Production of Minor Mineral in last three Years 26 12.0 Mineral map of the district 26 13.0 List of letter of intent (LOI) holder in the district along with its 27 validity 14.0 Total mineral reserve available in the district. 28 15.0 Quality / Grade of mineral available in the district 28 16.0 Use of mineral 29 17.0 Demand and supply of the mineral in the lase three years 30 2 DISTRICT SURVEY REPORT- THIRUVARUR 18.0 Mining leases marked on the map of the district 31 19.0 Details of the area where there is a cluster of mining leases viz., 33 number of mining leases, location (latitude & longitude) 20.0 Details of eco-sensitive area 33 21.0 Impact on the environment due to mining activity 35 22.0 Remedial measure to mitigate the impact of mining on the 36 environment 23.0 Reclamation of mined out -

Report of the Events
SENGAMALA THAYAAR EDUCATIONAL TRUST WOMEN’S COLLEGE SUNDARAKKOTTAI, MANNARGUDI - 614016. (Accredited with “A” grade by NAAC) (An ISO 9001:2015 Certified Institution) REPORT OF THE EVENTS SWACHH BHARAT REPORT 2018-2019 Sengamala Thayaar Educational Trust women’s college NSS Unit Organized the Summer Internship Camp under Swachh Bharat Mission in the places which are nearby our college. Like Sundarakkottai, Kandithampettai, Kelathirupalakudi. Sundarakkottai is a village located in Mannargudi block in Thiruvarur District of Tamilnadu state, India . It is located 31 km towards west from District Head Quarters Thiruvarur and 6 km from Mannargudi. The total population in the village consists 2070 which will help us to divide the work to make easier and to convey the message to the people. In sundarakkottai village, the people are very less aware about the cleanliness, usage of toilet, Solid waste disposal and so on. Some of the people were irresponsible to our words. Some more give co-operation to us to make the summer camp effective. We give our best to make the people with creating awareness by telling some of the causes and effects of open defecation and less cleanliness. People of Sundarakkottai had been poor knowledge about the issue of wastage and they are not ready to hear our words fully. Next we went to village of Kandithampettai for create awareness to people. Kandithampettai is a village located in Mannargudi Taluk of Thiruvarur(dt) Tamilnadu with total 800 families residing. The Kandithampettai village has population of 3634 of which male population is 1817 and the female is 1211 population of children with age (0-6). -

Sample Collection Centre for COVID
Sample Collection Centers # State District Centre Name Centre Address 1 TAMIL NADU Ariyalur ANDIMADAM MMU PHC ANDIMADAM 2 TAMIL NADU Ariyalur ANDIMADAM PHC ANDIMADAM 3 TAMIL NADU Ariyalur ANGANUR PHC ANGANUR 4 TAMIL NADU Ariyalur ARIYALUR URBAN MMU PHC ARIYALUR 5 TAMIL NADU Ariyalur ARIYALUR URBAN PHC ARIYALUR 6 TAMIL NADU Ariyalur ELAKURICHI PHC ELAKURICHI GOVERNMENT DISTRICT HEADQUATERS ARIYALUR 7 TAMIL NADU Ariyalur HOSPITAL 8 TAMIL NADU Ariyalur GOVT. DISTRICT HQ HOSPITAL ARIYALUR 9 TAMIL NADU Ariyalur JAYAMKONDAM GH JAYAMKONDAM GH 10 TAMIL NADU Ariyalur JAYAMKONDAM GH JAYAMKONDAM 11 TAMIL NADU Ariyalur JAYANKONDAM URBAN PHC JAYANKONDAM 12 TAMIL NADU Ariyalur KADUGUR UGPHC KADUGUR 13 TAMIL NADU Ariyalur KALLANKURICHY PHC KALLANKURICHY 14 TAMIL NADU Ariyalur KEELAPALUR PHC KEELAPALUR 15 TAMIL NADU Ariyalur KULUMUR PHC KULUMUR 16 TAMIL NADU Ariyalur KUMILIYAM ICTC UGPHC KUMILIYAM 17 TAMIL NADU Ariyalur KUMILIYAM UGPHC KUMILIYAM 18 TAMIL NADU Ariyalur KURUVADI MMU PHC GURUVADI 19 TAMIL NADU Ariyalur KURUVADI PHC KURUVADI 20 TAMIL NADU Ariyalur MANAKKAL PHC MANAKKAL 21 TAMIL NADU Ariyalur MANAKUDAIYAN PHC MANAKUDAIYAN .SENDHURAI MANAKUDIAYAN PRIMARY HEALTH CENTRE MANAKUDAIYAN 22 TAMIL NADU Ariyalur 23 TAMIL NADU Ariyalur MARUTHUR PHC MARUTHUR 24 TAMIL NADU Ariyalur MEENSURITI BLOCK PHC ICTC MEENSURITI 25 TAMIL NADU Ariyalur MEENSURITY CHC MEENSURITY JAYAKONDAM 26 TAMIL NADU Ariyalur MEENSURITY UGPHC MEENSURITY 27 TAMIL NADU Ariyalur PONPARAPPI PHC PONPARAPPI POYYATHANALLUR PRIMARY HEALTH CENTRE POYYATHANALLUR 28 TAMIL NADU Ariyalur 29 TAMIL NADU Ariyalur POYYUR PRIMARY HEALTH CENTRE POYYUR 30 TAMIL NADU Ariyalur SENDHURAI GH SENDHURAI 31 TAMIL NADU Ariyalur SUNDAKUDI PHC SUNDAKUDI 32 TAMIL NADU Ariyalur SUTHAMALLI PHC SUTHAMALLI 33 TAMIL NADU Ariyalur T PALUR CHC T PALUR 34 TAMIL NADU Ariyalur T PALUR MMU T PALUR COMMUNITY HEALTH CENTRE 35 TAMIL NADU Ariyalur T POTTAKOLLAI PRIMARY HEALTH CENTRE T POTTAKOLLAI 36 TAMIL NADU Ariyalur T.