Urinary Tract Infection in Patients Undergoing TURP
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CMS Manual System Human Services (DHHS) Pub
Department of Health & CMS Manual System Human Services (DHHS) Pub. 100-07 State Operations Centers for Medicare & Provider Certification Medicaid Services (CMS) Transmittal 8 Date: JUNE 28, 2005 NOTE: Transmittal 7, of the State Operations Manual, Pub. 100-07 dated June 27, 2005, has been rescinded and replaced with Transmittal 8, dated June 28, 2005. The word “wound” was misspelled in the Interpretive Guidance section. All other material in this instruction remains the same. SUBJECT: Revision of Appendix PP – Section 483.25(d) – Urinary Incontinence, Tags F315 and F316 I. SUMMARY OF CHANGES: Current Guidance to Surveyors is entirely replaced by the attached revision. The two tags are being combined as one, which will become F315. Tag F316 will be deleted. The regulatory text for both tags will be combined, followed by this revised guidance. NEW/REVISED MATERIAL - EFFECTIVE DATE*: June 28, 2005 IMPLEMENTATION DATE: June 28, 2005 Disclaimer for manual changes only: The revision date and transmittal number apply to the red italicized material only. Any other material was previously published and remains unchanged. However, if this revision contains a table of contents, you will receive the new/revised information only, and not the entire table of contents. II. CHANGES IN MANUAL INSTRUCTIONS: (N/A if manual not updated.) (R = REVISED, N = NEW, D = DELETED) – (Only One Per Row.) R/N/D CHAPTER/SECTION/SUBSECTION/TITLE R Appendix PP/Tag F315/Guidance to Surveyors – Urinary Incontinence D Appendix PP/Tag F316/Urinary Incontinence III. FUNDING: Medicare contractors shall implement these instructions within their current operating budgets. IV. ATTACHMENTS: Business Requirements x Manual Instruction Confidential Requirements One-Time Notification Recurring Update Notification *Unless otherwise specified, the effective date is the date of service. -

Urinary Tract Infection (Uti) Fact Sheet
URINARY TRACT INFECTION (UTI) FACT SHEET Overview A urinary tract infection (UTI) is an infection that involves any part of the urinary tract, including the kidneys, bladder and urethra. It is usually caused by exposure of the urinary tract to a fecal organism such as Escherichia coli (E. coli) but also may be caused by other organisms. An indwelling urinary catheter is a drainage tube that is inserted into the urinary bladder through the urethra, is left in place and is connected to a closed urine collection system. Urinary tract infections in patients with an indwelling urinary catheter are called catheter-associated UTIs, or CAUTIs. Signs and Symptoms Common symptoms of UTI include: • fever; • pain or burning in the lower abdomen; • burning during urination; • an increase in the frequency of urination; and • cloudy appearing urine. Causes and Transmission A UTI occurs when germs (usually bacteria) enter the urinary tract through the meatus (the opening of the urinary tract). These germs then cause infection. The urinary tract is normally sterile, meaning it contains no germs. A CAUTI occurs when germs (usually bacteria) enter the urinary tract through the urinary catheter and cause infection. This can occur when health care worker hands are not properly cleaned before the insertion of a catheter or during the process of cleaning or emptying of the urine collection system. Risk Factors Sexually active women, people with blockages in the urinary tract, such as prostate enlargement, and women using certain types of birth control, such as diaphragms, or those who are undergoing menopause are at higher risk of UTI. -

233 the Use of Absorbent Pads Increases the Risk For
233 Omli R1, Skotnes L H1, Romild U1, Kuhry E1 1. Namsos Hospital THE USE OF ABSORBENT PADS INCREASES THE RISK FOR LOWER URINARY TRACT INFECTIONS IN NURSING HOMES RESIDENTS. Hypothesis / aims of study Urinary incontinence is a common medical problem in the nursing home population. The aim of this study was to determine whether use of absorbent pads is a risk factor for the development of lower urinary tract infections in nursing home residents. Introduction Lower urinary tract infections (UTIs) are a common medical problem in the elderly. Different kinds of absorbent products, such as diapers, pad and pant combinations, are used in incontinence care. In some cases, indwelling catheters, external condom catheters or in-and-out catheterisation are options for managing bladder dysfunction. About 23% of the residents in nursing homes don’t need toilet assistance. That means that the majority of residents is dependent on help from nursing staff for toileting and help to change soiled absorbent pads. Transmission of bacteria during incontinence care is associated with UTIs in elderly. In the vulnerable nursing home population, UTIs are a frequent problem and can lead to increased morbidity and even mortality. The prevalence of UTIs in nursing home residents is approximately 30%. Improving hand hygiene among staffing in nursing homes is one of the most important and effective methods to reduce hand born transmission of pathological microbes. Studies in long-term-care facilities document a lack of hand hygiene in connection to staff-resident interactions. This study studies the association between the use of absorbent pads and symptomatic UTIs in the nursing home population. -
Module 3: Benign Prostatic Hypertrophy
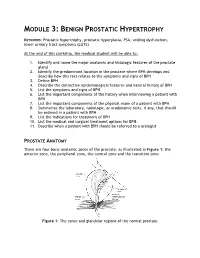
MODULE 3: BENIGN PROSTATIC HYPERTROPHY KEYWORDS: Prostatic hypertrophy, prostatic hyperplasia, PSA, voiding dysfunction, lower urinary tract symptoms (LUTS) At the end of this clerkship, the medical student will be able to: 1. Identify and name the major anatomic and histologic features of the prostate gland 2. Identify the predominant location in the prostate where BPH develops and describe how this fact relates to the symptoms and signs of BPH 3. Define BPH 4. Describe the distinctive epidemiological features and natural history of BPH 5. List the symptoms and signs of BPH 6. List the important components of the history when interviewing a patient with BPH 7. List the important components of the physical exam of a patient with BPH 8. Summarize the laboratory, radiologic, or urodynamic tests, if any, that should be ordered in a patient with BPH 9. List the indications for treatment of BPH 10. List the medical and surgical treatment options for BPH. 11. Describe when a patient with BPH should be referred to a urologist PROSTATE ANATOMY There are four basic anatomic zones of the prostate, as illustrated in Figure 1: the anterior zone, the peripheral zone, the central zone and the transition zone. Figure 1: The zones and glandular regions of the normal prostate. The anterior zone is entirely fibromuscular and non-glandular, and it appears to have little significance in prostatic function or pathology. This area comprises approximately 20% of the bulk of prostatic tissue. The peripheral zone is composed entirely of acinar tissue. It comprises the posterior surface of the prostate, including the apical, lateral, posterolateral and anterolateral portions of the prostate. -

Urinary Incontinence ! ! !What Is Urinary Incontinence? Leakage of Urine Is Called Urinary Incontinence
! ! ! Urinary Incontinence ! ! !What is urinary incontinence? Leakage of urine is called urinary incontinence. Some women leak small amounts of !urine. At other times, leakage of urine is frequent or severe. !Are there different types of urinary incontinence? !There are several types of urinary incontinence: • Stress urinary incontinence is loss of urine when a woman coughs, laughs, or sneezes. Leaks also can happen when a woman walks, runs, or exercises. It is caused by a weakening of the tissues that support the bladder or the muscles of the ! urethra. • Urge incontinence is leakage of urine caused by overactive bladder muscles that ! contract too often or problems with the nerves that send signals to the bladder !• Mixed incontinence is a combination of both stress and urge incontinence symptoms • Overflow incontinence is a steady loss of small amounts of urine when the bladder does not empty all the way during voiding. It can be caused by an underactive bladder ! muscle or blockage of the urethra. !What are the symptoms of urinary incontinence? !In addition to leaking urine, a woman with incontinence also may have other symptoms: • Urgency— A strong urge to urinate whether or not the bladder is full, often with pelvic ! pressure !• Frequency— Voiding more often than she considers usual !• Nocturia — The need to void during hours of sleep !• Dysuria — Painful voiding !• Enuresis— Bed-wetting or leaking while sleeping ! What causes urinary incontinence? ! Urinary incontience can have short-term causes and long-term causes. Short-term !causes are easier to treat and include the following: • Urinary tract infection— Loss of bladder control may be caused by an infection of the urinary tract. -

Frequently Asked Questions About Overactive Bladder
ABOUT OAB Frequently Asked Questions about Overactive Bladder What is Overactive Bladder (OAB)? If you live with OAB, you may also: Overactive Bladder (OAB) isn’t a disease. It’s the u Leak urine (incontinence): Sometimes people name of a group of urinary symptoms. The most with OAB also have “urgency incontinence.” common symptom of OAB is a sudden urge to This means that urine leaks when you feel urinate that you can’t control. Some people will the sudden urge to go. This isn’t the same as leak urine when they feel this urge. Having to “stress urinary incontinence” or “SUI.” People urinate many times during the day and night is with SUI leak urine while sneezing, laughing or another symptom of OAB. doing other physical activities. (You can learn more about SUI at UrologyHealth.org/SUI.) How common is OAB? u Urinate frequently: You may also need to go OAB is common. It affects millions of Americans. to the bathroom many times during the day. As many as 30 percent of men and 40 percent The number of times someone urinates varies of women in the United States live with OAB from person to person. But many experts symptoms. agree that going to the bathroom more than eight times in 24 hours is “frequent urination.” Who is at risk for OAB? u Wake up at night to urinate: Waking from As you grow older, you’re at higher risk for sleep to go to the bathroom more than once a OAB. But no matter what your age, there are night is another symptom of OAB. -

Diagnosis and Treatment of Overactive Bladder (Non-Neurogenic) in Adults: AUA/SUFU Guideline
Diagnosis and Treatment of Overactive Bladder (Non-Neurogenic) in Adults: AUA/SUFU Guideline E. Ann Gormley, Deborah J. Lightner, Kathryn L. Burgio, Toby C. Chai, J. Quentin Clemens, Daniel J. Culkin, Anurag Kumar Das, Harris Emilio Foster, Jr., Harriette Miles Scarpero, Christopher D. Tessier, Sandip Prasan Vasavada From the American Urological Association Education and Research, Inc., Linthicum, Maryland, and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction Purpose: The purpose of this guideline is to provide a clinical framework for the Abbreviations diagnosis and treatment of non-neurogenic overactive bladder (OAB). and Acronyms Materials and Methods: The primary source of evidence for this guideline is the AE ϭ adverse event systematic review and data extraction conducted as part of the Agency for ER ϭ extended release Healthcare Research and Quality (AHRQ) Evidence Report/Technology Assess- ϭ ment Number 187 titled Treatment of Overactive Bladder in Women (2009). That FDA Food and Drug report searched PubMed, MEDLINE®, EMBASE and CINAHL for English- Administration language studies published from January 1966 to October 2008. The AUA IR ϭ immediate release conducted additional literature searches to capture treatments not covered in OAB ϭ overactive bladder detail by the AHRQ report and relevant articles published between October PTNS ϭ peripheral tibial nerve 2008 and December 2011. The review yielded an evidence base of 151 treat- stimulation ment articles after application of inclusion/exclusion criteria. When sufficient PVR ϭ post-void residual evidence existed, the body of evidence for a particular treatment was assigned QoL ϭ quality of life a strength rating of A (high), B (moderate) or C (low). -

Urinary Tract Infection (UTI)
Patient Factsheet Hospital: Urinary Tract Infection (UTI) What is a UTI? Urethritis – inflammation of the urethra. A Urinary tract infection (UTI) is an infection Urethritis causes pain on urination and the of the urinary system – the bladder, kidneys, sensation of wanting to pass urine all the or even the ureters or urethra. They are more time. Often, you will pass frequent, small common in women, people with diabetes, mounts of urine. and more likely to affect the very young or the Cystitis – inflammation of the bladder. very old. Also men with prostate problems, and people with catheters or urinary tract Cystitis causes similar symptoms as abnormalities are at increased risk of urethritis, as well as pain in the lower developing a UTI. abdomen. Pyelonephritis – inflammation of the kidney. What causes a UTI? Infections involving the kidney are more UTIs are usually caused by bacteria. The serious. Most patients with pyelonephritis feel bacteria usually enters the urinary tract from quite unwell. You may experience: the bowel or back passage (anus), via the urethra (the tube from which urine exits the Fever and chills bladder). Pain in the loins and/or back UTIs can also be caused by sexually Nausea and loss of appetite. transmitted infections, such as Chlamydia. Blood in the urine is a common symptom of These can affect both men and women. If UTI, and can occur with any type of UTI. one person is diagnosed, their partner(s) will also require testing and treating to avoid Tests re-infection and potentially serious complications. A mid stream urine (MSU) specimen will be requested. -
Urinary Tract Infections
Urinary Tract Infections www.kidney.org Did you know that... n Urinary tract infections (UTIs) are responsible for nearly 10 million doctor visits each year. n One in five women will have at least one UTI in her lifetime. Nearly 20 percent of women who have a UTI will have another, and 30 percent of those will have yet another. Of this last group, 80 percent will have recurrences. n About 80 to 90 percent of UTIs are caused by a single type of bacteria. 2 NATIONAL KIDNEY FOUNDATION n UTIs can be treated effectively with medications called antibiotics. n People who get repeated UTIs may need additional tests to check for other health problems. n UTIs also may be called cystitis or a bladder infection. This brochure answers the questions most often asked about UTIs. If you have more questions, speak to your doctor. What is a urinary tract infection? A urinary tract infection is what happens when bacteria (germs) get into the urinary tract (the bladder) and multiply. The result is redness, swelling and pain in the urinary tract (see diagram). WWW.KIDNEY.ORG 3 Most UTIs stay in the bladder, the pouch-shaped organ where urine is stored before it passes out of the body. If a UTI is not treated promptly, the bacteria can travel up to the kidneys and cause a more serious type of infection, called pyelonephritis (pronounced pie-low-nef-right- iss). Pyelonephritis is an actual infection of the kidney, where urine is produced. This may result in fever and back pain. What causes a UTI? About 80 to 90 percent of UTIs are caused by a type of bacteria, called E. -

Neurogenic Bladder Jordache Mcleod, Jamie Milligan, Joe Lee, Matthew Smith
MOBILITY CLINIC CASE-BASED LEARNING MODULE Neurogenic Bladder Jordache McLeod, Jamie Milligan, Joe Lee, Matthew Smith INTRODUCTION Many patients with spinal cord injury (SCI) will have problems with emptying the bladder and/or storing urine; some of these issues are obvious, some are not. It is critical for primary care providers to work with patients to develop an effective voiding routine to avoid both acute and long-term complications of inadequate bladder management. This module will enable clinicians to: Become familiar with various methods of bladder voiding in neurogenic bladder Prescribe medications to assist in the storage of urine Identify and manage common complications of neurogenic bladder Determine appropriate follow-up and screening for patients CASE PAUL, AGE 24 Paul is a 24-year-old male who presents to the office with vague abdominal discomfort and a general sense of “feeling unwell”. He has an incomplete T4 spinal cord injury sustained within the last year. He is otherwise healthy. His vital signs are stable, with a heart rate of 65 and a blood pressure of 100/70. He is afebrile. What further information would you like to know on history? Has he ever had symptoms like this before and if so what was the cause? What is his current bladder management routine? Be specific! How does he empty his bladder and how often? Any constipation? Has he ever had autonomic dysreflexia (AD)? AD can occur in patients with SCI at level T6 or above, and bladder problems are the most frequent cause of AD. Has he had other symptoms suggestive of a UTI e.g., any change in urine colour, fever, sudden change in urinary symptoms, increased spasticity, or change in his ability to hold or void urine? Paul self-catheterizes every eight hours. -

Urinary Tract Infections (Utis) Brown Health Services Patient Education Series
Urinary Tract Infections (UTIs) Brown Health Services Patient Education Series ● In people with penises, urethritis can What is a UTI? sometimes cause a penile discharge A UTI is an infection involving any part of the Infection of the kidneys (pyelonephritis) can urinary tract which includes the urethra, urinary include all of the above as well as: bladder, ureters and kidneys. The urethra goes between the bladder and the outside. The ureters ● Lower back pain run between the kidneys and the bladder. Most ● High fever infections involve the lower tract– the urethra ● Shaking chills (urethritis) and/or urinary bladder (cystitis). These ● Nausea and Vomiting can be painful and annoying. ● Fatigue How common are they? What causes urinary tract infections? They are more common in people who have vulvas. The most common cause of UTIs is bacteria from One in 5 people with vulvas will likely develop a UTI the bowel such as E. coli that is present on the skin during their lifetime; many will experience more near the rectum or in the vagina. Once bacteria than one. A more serious kidney infection enter the urethra they travel upward causing (pyelonephritis) may occur if the infection spreads infection in the bladder and sometimes other parts from the lower tract into the kidneys. of the urinary tract. Sexual intercourse is commonly associated with UTIs in women. During intercourse, What are the signs and symptoms of a bacteria in the vaginal area are sometimes urinary tract infection? transferred into the urethra by the motion of the penis. Sexual intercourse may also irritate the Although some UTIs can be asymptomatic, common urethra allowing bacteria to more easily travel symptoms and signs include: through the urethra into the bladder. -

Painful Bladder Syndrome/Interstitial Cystitis Successful Treatment with Montelukast: a Case Report and Literature Review
Open Access Case Report DOI: 10.7759/cureus.2876 Painful Bladder Syndrome/Interstitial Cystitis Successful Treatment with Montelukast: A Case Report and Literature Review Muhammad Wajih Ullah 1 , Sunita Lakhani 2 , Sunder Sham 3 , Afshan Rehman 4 , Wardah Siddiq 5 , Tariq Siddiqui 6 1. Cardiology, Mayo Clinic, Rochester, USA 2. Internal Medicine, Liaquat University of Medical and Health Sciences Hospital, Jamshoro, PAK 3. Internal Medicine, Ghulam Muhammad Mahar Medical College, Sukkur, PAK 4. Internal Medicine, Baylor Saint Luke's Medical Center, Houston, USA 5. Internal Medicine, Beth Israel Deaconess Medical Center/Harvard Medical College, Boston, USA 6. Internal Medicine, Maharashtra Institute of Medical Education & Research, Talegaon, IND Corresponding author: Muhammad Wajih Ullah, [email protected] Abstract Painful bladder syndrome/interstitial cystitis (PBS/IC) is a chronic condition characterized by pelvic pain, urinary frequency, and urgency for more than six months in the absence of urinary tract infections. The etiology of PBS/IC is still an enigma. PBS/IC is challenging for doctors to diagnose because its symptoms overlap with other diseases such as urinary tract infection, overactive bladder, or endometriosis. Hence, it is diagnosed after excluding those diseases. The prognosis of PBS/IC may vary because of multiple treatment options. In this study, we are documenting a 26-year-old female patient who was successfully treated with montelukast after diagnosed with PBS/IC. Categories: Internal Medicine, Urology, Pulmonology Keywords: bladder pain syndrome, montelukast, asthma Introduction Painful bladder syndrome/interstitial cystitis (PBS/IC) is a disease of unknown etiology. The male-to-female ratio is 1:9 in the US population survey [1].