The Lacrimation Reflex* by J
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anatomical Study of the Zygomaticotemporal Branch Inside the Orbit
Open Access Original Article DOI: 10.7759/cureus.1727 Anatomical Study of the Zygomaticotemporal Branch Inside the Orbit Joe Iwanaga 1 , Charlotte Wilson 1 , Koichi Watanabe 2 , Rod J. Oskouian 3 , R. Shane Tubbs 4 1. Seattle Science Foundation 2. Department of Anatomy, Kurume University School of Medicine 3. Neurosurgery, Complex Spine, Swedish Neuroscience Institute 4. Neurosurgery, Seattle Science Foundation Corresponding author: Charlotte Wilson, [email protected] Abstract The location of the opening of the zygomaticotemporal branch (ZTb) of the zygomatic nerve inside the orbit (ZTFIN) has significant surgical implications. This study was conducted to locate the ZTFIN and investigate the variations of the ZTb inside the orbit. A total of 20 sides from 10 fresh frozen cadaveric Caucasian heads were used in this study. The vertical distance between the inferior margin of the orbit and ZTFIN (V-ZTFIN), the horizontal distance between the lateral margin of the orbit and ZTFIN (H-ZTFIN), and the diameter of the ZTFIN (D-ZTFIN) were measured. The patterns of the ZTb inside the orbit were classified into five different groups: both ZTb and LN innervating the lacrimal gland independently (Group A), both ZTb and LN innervating the lacrimal gland with a communicating branch (Group B), ZTb joining the LN without a branch to the lacrimal gland (Group C), the ZTb going outside the orbit through ZTFIN without a branch to the lacrimal gland nor LN (Group D), and absence of the ZTb (Group E). The D-ZTFIN V-ZTFIN H-ZTFIN ranged from 0.2 to 1.1 mm, 6.6 to 21.5 mm, 2.0 to 11.3 mm, respectively. -

Oculoplastics/Orbit 2017-2019
Academy MOC Essentials® Practicing Ophthalmologists Curriculum 2017–2019 Oculoplastics and Orbit *** Oculoplastics/Orbit 2 © AAO 2017-2019 Practicing Ophthalmologists Curriculum Disclaimer and Limitation of Liability As a service to its members and American Board of Ophthalmology (ABO) diplomates, the American Academy of Ophthalmology has developed the Practicing Ophthalmologists Curriculum (POC) as a tool for members to prepare for the Maintenance of Certification (MOC) -related examinations. The Academy provides this material for educational purposes only. The POC should not be deemed inclusive of all proper methods of care or exclusive of other methods of care reasonably directed at obtaining the best results. The physician must make the ultimate judgment about the propriety of the care of a particular patient in light of all the circumstances presented by that patient. The Academy specifically disclaims any and all liability for injury or other damages of any kind, from negligence or otherwise, for any and all claims that may arise out of the use of any information contained herein. References to certain drugs, instruments, and other products in the POC are made for illustrative purposes only and are not intended to constitute an endorsement of such. Such material may include information on applications that are not considered community standard, that reflect indications not included in approved FDA labeling, or that are approved for use only in restricted research settings. The FDA has stated that it is the responsibility of the physician to determine the FDA status of each drug or device he or she wishes to use, and to use them with appropriate patient consent in compliance with applicable law. -

Nomina Histologica Veterinaria, First Edition
NOMINA HISTOLOGICA VETERINARIA Submitted by the International Committee on Veterinary Histological Nomenclature (ICVHN) to the World Association of Veterinary Anatomists Published on the website of the World Association of Veterinary Anatomists www.wava-amav.org 2017 CONTENTS Introduction i Principles of term construction in N.H.V. iii Cytologia – Cytology 1 Textus epithelialis – Epithelial tissue 10 Textus connectivus – Connective tissue 13 Sanguis et Lympha – Blood and Lymph 17 Textus muscularis – Muscle tissue 19 Textus nervosus – Nerve tissue 20 Splanchnologia – Viscera 23 Systema digestorium – Digestive system 24 Systema respiratorium – Respiratory system 32 Systema urinarium – Urinary system 35 Organa genitalia masculina – Male genital system 38 Organa genitalia feminina – Female genital system 42 Systema endocrinum – Endocrine system 45 Systema cardiovasculare et lymphaticum [Angiologia] – Cardiovascular and lymphatic system 47 Systema nervosum – Nervous system 52 Receptores sensorii et Organa sensuum – Sensory receptors and Sense organs 58 Integumentum – Integument 64 INTRODUCTION The preparations leading to the publication of the present first edition of the Nomina Histologica Veterinaria has a long history spanning more than 50 years. Under the auspices of the World Association of Veterinary Anatomists (W.A.V.A.), the International Committee on Veterinary Anatomical Nomenclature (I.C.V.A.N.) appointed in Giessen, 1965, a Subcommittee on Histology and Embryology which started a working relation with the Subcommittee on Histology of the former International Anatomical Nomenclature Committee. In Mexico City, 1971, this Subcommittee presented a document entitled Nomina Histologica Veterinaria: A Working Draft as a basis for the continued work of the newly-appointed Subcommittee on Histological Nomenclature. This resulted in the editing of the Nomina Histologica Veterinaria: A Working Draft II (Toulouse, 1974), followed by preparations for publication of a Nomina Histologica Veterinaria. -

Ectopic Intraocular Lacrimal Gland Tissue
Br J Ophthalmol: first published as 10.1136/bjo.56.9.690 on 1 September 1972. Downloaded from Brit. _. Ophthal. (I972) 56, 690 Ectopic intraocular lacrimal gland tissue GWYN MORGAN AND ALAN MUSHIN Departments of Pathology and Clinical Ophthalmology, Institute of Ophthalmology, University of London Ectopic lacrimal gland tissue is rarely found within the eye. The first report was that of Puech (i 887) who described an adenoma ofthe choroid in an adult female. The lesion had the appearance of lacrimal gland tissue which was adherent to the sclera and the retina. After an interval of 65 years Christensen and Anderson (I 952) described ectopic lacrimal gland tissue within the sclera, ciliary body, limbus, and iris in an infant of 2 weeks. Bruce (I 952) described a case in the iris of a 2-month-old boy who was 2 weeks premature. No other abnormalities were noted in these infants. Hunter (i 960) described a fourth case in which ectopic cystic lacrimal gland tissue was seen in the ciliary body, iris, and sclera. The fifth case was described by Dallachy (i96i) in a 2-month-old female infant; ectopic lacrimal gland tissue was seen in the ciliary body and iris. A search of the literature since I96I revealed only one other case of intraocular lacrimal gland tissue (Green and Zimmerman, I967); their patient was a s-month-old child with ectopic lacrimal gland tissue in the limbal area and a nodule ofsimilar tissue in the chamber angle, on the anterior copyright. surface of the iris, and in the ciliary body. -

Eye External Anatomy of Eye Accessory Structures
4/22/16 Eye Bio 40B Dr. Kandula External Anatomy of Eye Accessory Structures l Eyebrows l Levator Palpebrae Superioris - opens eye l Eyelashes l Ciliary glands – modified sweat glands l Small sebaceous glands l Sty is inflamed ciliary glands or small sebaceous glands 1 4/22/16 Terms: Lacrimal gland and duct Surface of eye Lacrimal puncta Lacrimal sac Nasolacrimal duct Nasal cavity Tears / Lacrimal fluid l a watery physiologic saline, with a plasma-like consistency, l contains the bactericidal enzyme lysozyme; l it moistens the conjunctiva and cornea, l provides nutrients and dissolved O2 to the cornea. Extrinsic Muscles of the Eye: Lateral/medial rectus Important to know Superior/inferior rectus actions and nerve Superior/inferior oblique supply in table 2 4/22/16 Extrinsic Eye Muscles • Eye movements controlled by six extrinsic eye muscles Four recti muscles § Superior rectus – moves eyeball superiorly supplied by Cranial Nerve III § Inferior rectus - moves eyeball inferiorly supplied by Cranial Nerve III § Lateral rectus - moves eyeball laterally supplied by Cranial Nerve VI § Medial rectus - moves eyeball medially supplied by Cranial Nerve III Extrinsic Eye Muscles Two oblique muscles rotate eyeball on its axis § Superior oblique rotates eyeball inferiorly and laterally and is supplied by Cranial Nerve IV § Inferior oblique rotates superiorly and laterally and is supplied by Cranial Nerve III Convergence of the Eyes l Binocular vision in humans has both eyes looking at the same object l As you look at an object close to your face, -

Anatomy of the Periorbital Region Review Article Anatomia Da Região Periorbital
RevSurgicalV5N3Inglês_RevistaSurgical&CosmeticDermatol 21/01/14 17:54 Página 245 245 Anatomy of the periorbital region Review article Anatomia da região periorbital Authors: Eliandre Costa Palermo1 ABSTRACT A careful study of the anatomy of the orbit is very important for dermatologists, even for those who do not perform major surgical procedures. This is due to the high complexity of the structures involved in the dermatological procedures performed in this region. A 1 Dermatologist Physician, Lato sensu post- detailed knowledge of facial anatomy is what differentiates a qualified professional— graduate diploma in Dermatologic Surgery from the Faculdade de Medician whether in performing minimally invasive procedures (such as botulinum toxin and der- do ABC - Santo André (SP), Brazil mal fillings) or in conducting excisions of skin lesions—thereby avoiding complications and ensuring the best results, both aesthetically and correctively. The present review article focuses on the anatomy of the orbit and palpebral region and on the important structures related to the execution of dermatological procedures. Keywords: eyelids; anatomy; skin. RESU MO Um estudo cuidadoso da anatomia da órbita é muito importante para os dermatologistas, mesmo para os que não realizam grandes procedimentos cirúrgicos, devido à elevada complexidade de estruturas envolvidas nos procedimentos dermatológicos realizados nesta região. O conhecimento detalhado da anatomia facial é o que diferencia o profissional qualificado, seja na realização de procedimentos mini- mamente invasivos, como toxina botulínica e preenchimentos, seja nas exéreses de lesões dermatoló- Correspondence: Dr. Eliandre Costa Palermo gicas, evitando complicações e assegurando os melhores resultados, tanto estéticos quanto corretivos. Av. São Gualter, 615 Trataremos neste artigo da revisão da anatomia da região órbito-palpebral e das estruturas importan- Cep: 05455 000 Alto de Pinheiros—São tes correlacionadas à realização dos procedimentos dermatológicos. -

TEAR PRODUCTION and DRAINAGE the Lacrimal Gland Is Located in the Superolateral Aspect of the Eyelid Below the Eyebrow(S)
Anatomy and Physiology 9 The conjunctiva is a mucous membrane that lines the upper and lower eyelids and extends over the sclera to the corneal margin. It contains lym- phoid tissue, which provides some immunology protection. It is innervated by CN V, the trigeminal nerve. The portion of the conjunctiva that covers the sclera is termed the bulbar conjunctiva; the portion covering the inner surface of the eyelids is termed the palpebral conjunctiva. Figure 1. Eyelid Muscles TEAR PRODUCTION AND DRAINAGE The lacrimal gland is located in the superolateral aspect of the eyelid below the eyebrow(s). It secretes watery (aqueous) tears and produces about 0.2 ml of tears in 24 hours. Aqueous tears flow downward and inward toward the tear drainage system at the inner canthus. In addition to aqueous tears, several glands located in the conjunctiva and eyelid margins secrete oily and sticky (mucous) tears. The meibomian glands are located within the tarsal plate of the eyelid and secrete oily tears. The glands of Zeiss, Moll, Wolfing, and Krause secrete sticky tears. These three types of tears provide moisture and protection to the surface of the eye(s). With each blink, tears are pushed across the eye toward the puncta located at the medial junction of the upper and lower eyelids. From the puncta, tears are pushed into the canaliculi and then into the lacrimal sac. 10 Essentials of Ophthalmic Nursing They are drained from the lacrimal sac and nasolacrimal duct to the inside of the nose and down the throat (see Figure 2). Figure 2. Lacrimal System TEAR FILM The tear film has three distinct layers. -

Lacrimal Gland Pathologies from an Anatomical Perspective
Review Article Acta Medica Anatolia Volume 3 Issue 3 2015 Lacrimal Gland Pathologies from an Anatomical Perspective Mahmut Sinan Abit Bingol State Hospital, Bingol, Turkey. Abstract Most of the patients in our daily practice have one or more ocular surface disorders including conjunctivitis, keratitis, dry eye disease, meibomian gland dysfunction, contact lens related symptoms, refractive errors, computer vision syndrome. Lacrimal gland has an important role in all above mentioned pathologies due to its major secretory product. An anatomical and physi- ological knowledge about lacrimal gland is a must in understanding basic and common ophthalmological cases. İn this paper it is aimed to explain the lacrimal gland diseases from an anatomical perspective. Keywords: lacrimal gland, anatomy Received: 07.08.2015 Accepted: 30.09.2015 doi: 10.15824/actamedica.96512 Introduction Lacrimal gland is pinkish-gray, lobulated serous can also be seen as a component of some syndromes gland. The aqueous component of tear film is mainly such as triple A syndrome in which achalasia and provided by lacrimal gland (1). In the first trimester addison disease accompanies alacrima. Besides dry eye, of pregnancy and at 19-21 mm stage of embryologic mental retardation, autonomic dysfunction, deafness development, it appears as epithelial buddings from and hyperkeratosis on palms of hands and soles of feet superolateral conjunctival fornix ectoderm. The are additional symptoms of this syndrome (5). mesenchymal condensations around these clusters Lacrimal gland is situated in the superotemporal orbit. than turn in to secretory components. These early It measures about 20 mm long, by 12 mm wide and epithelial buds with secretory components form the by 5 mm thick (6). -

Parasympathetic Nucleus of Facial Nerve
Neurology of Lacrimation Michael Davidson Professor, Ophthalmology Diplomate, American College of Veterinary Ophthalmologists Department of Clinical Sciences College of Veterinary Medicine North Carolina State University Raleigh, North Carolina, USA Trigeminal Nerve and Lacrimation Sensory afferent from lacrimal gland, adnexa, eye – through ophthalmic division and first branch of maxillary division (zygomatic n.) maxillary branch To trigeminal ganglion ophthalmic branch – adjacent to petrous temporal bone lateral to mandibular branch cavernous sinus near middle ear trigeminal ganglion Terminal branches of trigeminal n. trigeminal nerve distributes sympathetic and parasympathetic efferent to lacrimal gland and face Trigeminal-Lacrimal Reflex Afferent arm = CN V, ophthalmic division ⇒trigeminal ganglion ⇒ principle CN V nuclei Efferent arm = parasympathetic efferent to lacrimal gland(s) Elicits reflex tearing Parasympathetic efferent also supplies basal stimuli for lacrimation www.slideplayer.com Parasympathetic Efferent to Lacrimal Gland CN VII parasympathetic nuclei ⇒ greater petrosal nerve (petrous temporal bone) ⇒ nerve of pterygoid canal (with post ganglionic sympathetics) ⇒ synapse in pterygopalatine ganglion (ventral periorbital region, near apex of orbit) ⇒ zygomatic nerve (CN V, maxillary division)* ⇒ zygomaticotemporal nerve ⇒ acinar cells of lacrimal gland** *some texts state postganglionic parasympathetic fibers also in lacrimal nerve (ophthalmic division CNV) **postganglionic parasympathetic innervation to nictitans -
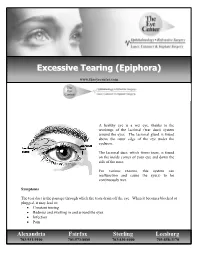
Excessive Tearing (Epiphora ))
EExxcceessssiivvee TTeeaarriinngg ((EEppiipphhoorraa)) www.theeyecenter.com A healthy eye is a wet eye, thanks to the workings of the lacrimal (tear duct) system around the eyes. The lacrimal gland is found above the outer edge of the eye under the eyebrow. The lacrimal duct, which forms tears, is found on the inside corner of your eye and down the side of the nose. For various reasons, this system can malfunction and cause the eye(s) to be continuously wet. Symptoms The tear duct is the passage through which the tears drain off the eye. When it becomes blocked or plugged, it may lead to: • Constant tearing • Redness and swelling in and around the eyes • Infection • Pain Alexandria Fairfax Sterling Leesburg 703-931-9100 703-573-8080 703-430-4400 703-858-3170 The blockage may be due to: • Mucous buildup in the lacrimal duct at birth and in infancy • Ingrown eyelashes • Thick or hardened discharge from an eye infection such as conjunctivitis (pink eye) • Continued exposure to allergens that irritate the eyes • Obstruction due to airborne irritants especially in the work environment (i.e. dust, chemicals, smoke or pollution) • Other eye conditions, such as a stye, that cause the eye to have an unusual discharge that can harden and plug the lacrimal duct. Treatment The ophthalmologist will examine the eye and may probe the tear duct to determine if a blockage exists. Initially, antibiotic drops may be prescribed to treat the infection, and possibly corticosteroid drops to treat any swelling. The blockage can often be worked loose by massaging the tear duct along the side of the eye and down the nose. -

Lecture 7 Anatomy the PTERYGOPALATINE FOSSA
د.احمد فاضل القيسي Lecture 7 Anatomy THE PTERYGOPALATINE FOSSA The pterygopalatine fossa lies beneath the posterior surface of the maxilla and the pterygoid process of the sphenoid bone. The pterygopalatine fossa contains the maxillary nerve, the maxillary artery (third part) and the pterygopalatine parasympathetic ganglion. Boundaries Anteriorly: posterior surface of maxilla. Posteriorly: anterior margin of pterygoid process below and greater wing of sphenoid above. Medially: perpendicular plate of palatine bone. Superiorly: greater wing of sphenoid. Laterally: communicates with infratemporal fossa through pterygomaxillary fissure Communications and openings: 1. The pterygomaxillary fissure: transmits the maxillary artery from the infratemporal fossa, the posterior superior alveolar branches of the maxillary division of the trigeminal nerve and the sphenopalatine veins. 2. The inferior orbital fissure: transmits the infraorbital and zygomatic branches of the maxillary nerve, the orbital branches of the pterygopalatine ganglion and the infraorbital vessels. 3. The foramen rotundum from the middle cranial fossa, occupying the greater wing of the sphenoid bone and transmit the maxillary division of the trigeminal nerve 4. The pterygoid canal from the region of the foramen lacerum at the base of the skull. The pterygoid canal transmits the greater petrosal and deep petrosal nerves (which combine to form the nerve of the pterygoid canal) and an accompanying artery derived from the maxillary artery. 5. The sphenopalatine foramen lying high up on the medial wall of the fossa.This foramen communicates with the lateral wall of the nasal cavity. It transmits the nasopalatine and posterior superior nasal nerves (from the pterygopalatine ganglion) and the sphenopalatine vessels. 6. The opening of a palatine canal found at the base of the fossa. -

The Lacrimal System Terms
The Lacrimal System Lynn E. Lawrence, CPOT, ABOC, COA, OSC Terms • Etiology – the cause of a disease or abnormal condition • Dacryocystitis – inflammation of the lacrimal sac • Epiphora – watering of eyes due to excess secretion of tears or obstruction of the lacrimal passage Tear Film Layers oil aqueous snot What functions does each layer of the tear perform? Lacrimal System: Tear Film Layers LIPID DEFICIENCY ‐ evaporates TEAR DEFICIENCY – fails to hydrate properly oil aqueous snot What functions does each layer of the tear perform? What are functions of tears? Tear Components • Lipid Layer – prevents evaporation • Aqueous Layer ‐ hydration • Mucus Layer – sticks tear to the eye • Other components Lacrimal Apparatus • Sometimes a person cannot produce natural tears they might need punctal plugs to prevent the tears from draining off the eye. • Faucet • Action • Drain Obstructive – vs‐ non‐obstructive Tear Production – Secretory • Lacrimal gland – Reflex tearing – Too much tearing…epiphora • Gland of Krause – Superior fornix • Gland of Wolfring – Superior tarsal plate Two Primary Forms of Dry Eye 800 nm 8,000 nm 100 nm The two primary forms of dry eye are Evaporative Dry Eye, also known as Meibomian Gland Dysfunction or MGD and Aqueous Dry Eye. The majority of dry eye sufferers have MGD. Oil & Water Remember science class? Oil floats. Oil does not mix with water, but rather sits on top of water. Oil is what keeps water from evaporating. Need three volunteers TEST TIME http://optometrytimes.modernmedicine.com/optometrytimes/news/treating‐dry‐eye‐ lipid‐based‐eye‐drops Lipid Secretion: Meibomian Glands Left: Transillumination of eyelid showing meibomian glands Right: Secretion of lipid at lid margin • The lipid layer restricts evaporation to 5‐10% of tear flow – Also helps lubricate Mucin Secretion: Goblet Cells Superficial layer of bulbar conjunctiva.