Mobile Learning for HIV/AIDS Healthcare Worker
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

SAMPLE – Apple Iphone Review - Article (Copyrighted Content – Not for Re-Use)
Godot Content Services Website: content.godotmedia.com Email: [email protected] SAMPLE – Apple iPhone Review - Article (Copyrighted Content – Not for Re-use) Apple iPhone 3GS Overview The ‘S’ in Apple’s 3GS iPhone denotes better speed and performance, which comes from the higher RAM and a faster processor. The 3GS undoubtedly gives a better performance than its predecessors. It also comes with video recording, voice control, copy-paste and MMS features. Its biggest weakness however is with regard to USB transfers and it is time Apple did something about it. Design The design of the iPhone 3GS is almost identical to the 3G version, measuring 4.5 x 2.4 x 0.48 inches. It comes in black and white colors. It is slightly heavier though, at 135 grams. The 3GS has a 3.5-inch widescreen display with a 480×320 resolution. The display is brighter than the 3G phone. To reduce the effects of fingerprint smudges, it features an oleophobic glaze on the display screen. Camera iPhone 3GS comes with an improved 3 megapixel camera but still falls short of the Nokia N95’s 5 megapixel camera. It now has autofocus, a feature that adjusts the color, balance, and contrast of the subject being photographed with just a tap on the display. It also comes with better low light sensitivity. But Apple has yet again decided against flash and digital zoom, which will disappoint many users. The image quality is decent. The device comes with a new video recording feature in VGA resolution at 30fps. Another great feature is video editing, where the video is displayed in different frames and you can change the clip in several ways. -

Nokia Phones: from a Total Success to a Total Fiasco
Portland State University PDXScholar Engineering and Technology Management Faculty Publications and Presentations Engineering and Technology Management 10-8-2018 Nokia Phones: From a Total Success to a Total Fiasco Ahmed Alibage Portland State University Charles Weber Portland State University, [email protected] Follow this and additional works at: https://pdxscholar.library.pdx.edu/etm_fac Part of the Engineering Commons Let us know how access to this document benefits ou.y Citation Details A. Alibage and C. Weber, "Nokia Phones: From a Total Success to a Total Fiasco: A Study on Why Nokia Eventually Failed to Connect People, and an Analysis of What the New Home of Nokia Phones Must Do to Succeed," 2018 Portland International Conference on Management of Engineering and Technology (PICMET), Honolulu, HI, 2018, pp. 1-15. This Article is brought to you for free and open access. It has been accepted for inclusion in Engineering and Technology Management Faculty Publications and Presentations by an authorized administrator of PDXScholar. Please contact us if we can make this document more accessible: [email protected]. 2018 Proceedings of PICMET '18: Technology Management for Interconnected World Nokia Phones: From a Total Success to a Total Fiasco A Study on Why Nokia Eventually Failed to Connect People, and an Analysis of What the New Home of Nokia Phones Must Do to Succeed Ahmed Alibage, Charles Weber Dept. of Engineering and Technology Management, Portland State University, Portland, Oregon, USA Abstract—This research intensively reviews and analyzes the management made various strategic changes to take the strategic management of technology at Nokia Corporation. Using company back into its leading position, or at least into a traditional narrative literature review and secondary sources, we position that compensates or reduces the losses incurred since reviewed and analyzed the historical transformation of Nokia’s then. -

Smartphone-Based Vehicle Telematics — a Ten-Year Anniversary Johan Wahlstrom,¨ Isaac Skog, Member, IEEE, and Peter Handel,¨ Senior Member, IEEE
Internet of Things Telematics Vehicle Telematics Smartphone-based Vehicle Telematics Smartphone-based Vehicle Telematics — A Ten-Year Anniversary Johan Wahlstrom,¨ Isaac Skog, Member, IEEE, and Peter Handel,¨ Senior Member, IEEE Abstract—Just like it has irrevocably reshaped social life, Estimated market value: the fast growth of smartphone ownership is now beginning to revolutionize the driving experience and change how we think 263 about automotive insurance, vehicle safety systems, and traffic Internet of Things research. This paper summarizes the first ten years of research in smartphone-based vehicle telematics, with a focus on user- 138 friendly implementations and the challenges that arise due to Telematics the mobility of the smartphone. Notable academic and industrial projects are reviewed, and system aspects related to sensors, Vehicle Telematics 45 energy consumption, cloud computing, vehicular ad hoc net- [Billion dollars] works, and human-machine interfaces are examined. Moreover, we highlight the differences between traditional and smartphone- Smartphone-based based automotive navigation, and survey the state-of-the-art Vehicle Telematics By 2020 By 2019 in smartphone-based transportation mode classification, driver classification, and road condition monitoring. Future advances are expected to be driven by improvements in sensor technology, evidence of the societal benefits of current implementations, and the establishment of industry standards for sensor fusion and Fig. 1. A Venn diagram illustrating the relation between the internet of things, telematics, vehicle telematics, and smartphone-based vehicle telemat- driver assessment. ics. Predicted market values are $263 billion (internet of things, by 2020) [2], Index Terms—Smartphones, internet-of-things, telematics, ve- $138 billion (telematics, by 2020) [7], and $45 billion (vehicle telematics, by hicle navigation, usage-based-insurance, driver classification. -

'Inferior' Iphone 9 January 2017, by Nigel Linge
Nokia had the world's best smartphone – then came the 'inferior' iPhone 9 January 2017, by Nigel Linge device as a phone first and a computer second. That's not too surprising given its history and evolution, starting out as a basic telephone and slowly but surely acquiring more computing features. But a new entrant can turn thinking on its head, and that's precisely what Apple did by viewing the handset as primarily a computer that just happened to include a phone capability. This was clearly reflected in its appearance, where the physical keyboard was eliminated and replaced by a single button and large touch screen. In Credit: Sami Keinänen/Flickr, CC BY-SA contrast, the Nokia N95 had a range of buttons and a slide feature that revealed a conventional phone keypad. Ten years ago, anyone who wanted the latest and Even more important were the key differences best smartphone was excited about the Nokia N95. between the software that controlled the two Launched at the Nokia Open Studio in September phones. Nokia was locked into the cumbersome 2006, it was trumpeted as the all-in-one multimedia Symbian operating system and its complex user computer and went on to achieve sales of a million interface, whereas Apple iOS was centred on the handsets within the UK in its first year. touch screen with gesture controls and had a fully functioning web browser and, of course, apps. On paper, it had everything a gadget-lover could desire, including a 2.6-inch LCD screen, a Several reviewers at the time were rather lukewarm 5-megapixel camera with Carl Zeiss optics and towards the iPhone, concerned about its technical video recorder, up to 8GB of storage, 3G and WiFi inadequacies and especially its lack of 3G. -

Iphone: Surviving the Shakeout
iPhone: Surviving The Shakeout Robin Abraham, Daniel Alvarez, Brent Goldman, and Craig Vieregg BEM 106 – Competitive Strategy, Spring Term June 4, 2008 iPhone: Surviving the Shakeout 1 Table of Contents 1 Executive Summary............................................................................................................. 3 2 History ..................................................................................................................................... 3 3 Six Forces Analysis .............................................................................................................. 4 3.1 Competition .....................................................................................................................................4 3.2 New Entrants...................................................................................................................................5 3.3 Buyer Bargaining Power ............................................................................................................5 3.4 Supplier Bargaining Power .......................................................................................................5 3.5 Substitute Products ......................................................................................................................6 3.6 Complements/Synergies............................................................................................................6 4 SWOT Analysis ..................................................................................................................... -

7. 3G/3.5G Mobile Phone/PDA Support
7. 3G/3.5G Mobile Phone/PDA Support To streaming from 3/3.5G mobile phone or PDA, you have to open the mobile port of DVR, the default setting is 7050, which may be changed, please refer to 5.5.5 PPPoE/DDNS(Net- Second Page] or IE 6.5 Device Parameters Settings ServerÆNetwork setting, video system For limited upload bandwidth of internet that DVRs connect, or limited streaming capability of some mobile phone/PDA, you have to adjust bandwidth of DVR to internet, please refer to 5.3.8 Dual Streaming for Network(Record- Advanced Setting) or 6.5 Device Parameters Settings - ChannelÆ Camera setting, Sub Bitstream, Subcode (from IE) for more details You may find the Windows Mobile 5.0/6.0/6.1 PDA(amplayersetup.CAB) and Symbian S60 3rd (P2P_S60_3rd_0113.sis) and S60 5th(P2P_S60_5Th_20090112.sis) softwares from the CD inside the DVR package or visit your DVR website to download by IE – http://xxx.xxxx.xxxx/download.html Note: User’s mobile phone must apply internet connection service at first, such as 3G or 3.5G service. Please contact mobile company for detail. 7. 1 Windows Mobile PDA Open accessory CD and find the “amplayersetup.CAB” for the surveillance software. Please refer to PDA user manual, copy *.cab into windows mobile pda Double click on *.cab can start install software into PDA. After install completed, user can find QQEYE in the application list. Execute QQEYE program and click to setup IP address of remote DVR. - 60 - Input user name 〖Admin〗and password. IP address of DVR and port:7050 for streaming data. -

Nokia N95 8GB Data Sheet
Nokia N95 8GB Planned Market Introduction Data Sheet Q4 2007 Category Multimedia Computer Key Features Stunning Screen, Massive Memory Luminous 2.8” QVGA display – watch video, view vibrant images, web pages and maps. Store your media and files on 8GB of built- in memory: carry up to 20 hours of video, or up to 6000 songs. Search or Explore: Nokia Maps Built-in GPS with Assisted GPS (A-GPS) support and maps data for over 150 countries and navigation support for over 30 countries. Higher Speed – Less Waiting – More Fun Fast ways to connect people with their passions and with people Nokia Nseries Experiences who share them, through WLAN or HSDPA (3.5G) with up to 10 times faster download than with 3G. Slide and Play MEDIA Unique 2-way slide for fast transition from a powerful multimedia computer to a multimedia player Crystal clear 2.8” QVGA (240 x 320) display with up to 16M colors Shoot and Share Stream media files from compatible media portals 5 megapixel camera with Carl Zeiss optics and auto focus. DVD-like The real web with Nokia Web Browser with Mini Map video quality with stabilization feature, VGA resolution and up to Visual Radio support 30 fps. MUSIC Digital music player supports MP3/AAC/eAAC/eAAC+/M4A/WMA Technical Profile with playlists System: WCDMA2100 (HSDPA), EGSM900, Up to 10 hours playback GSM850/1800/1900 MHz (EGPRS) Dedicated music keys User Interface: S60 3rd Edition, Feature Pack 3.1 Stereo FM radio (87.5-108MHz) Dimensions: 99 x 53 x 21mm (L x W x H), (96 cc) Integrated stereo hands free speaker Weight: -

Bluetooth Firmware Version 1.70 Bluetooth Firmware Version 1.70
Bluetooth firmware Version 1.70 yes = Feature is supported and confirmed. no = Feature is not supported by the Kenwood Bluetooth Module. n/a = Feature is not supported by the Phone. Bluetooth firmware Version 1.70 Phone connection Phonebook Phonebook Phonebook Phonebook Enable to use Market Network Pairing from Pick-up and Phonebook Display Display Enable to use Enable to Notify about Brand Model ROM Version Dial number Redial automatic transfer - transfer - transfer- AVRCP Target Area Operator From Phone KENWOOD Hang-up a call transfer battery level network level A2DP profile send SMS new SMS synchronisation one by one selection all profile Bluetooth Model Apple iPhone (AT&T) 2.1 (5F136) - - yes yes yes yes yes yes - - - n/a yes yes n/a n/a n/a n/a Apple iPhone 3G (AT&T) 2.1 (5F136) - - yes yes yes yes yes yes - - - n/a yes yes n/a n/a n/a n/a AU W54S - - - yes yes yes yes yes n/a - - - yes yes yes no no n/a n/a Blackberry 8100 Pearl (AT&T) 4.2.1.96 - - yes yes yes yes yes yes - - - yes yes yes n/a n/a n/a n/a Blackberry 8100 Pearl (T-Mobile) 4.2.0.42 - - yes yes yes yes yes yes - - - yes yes yes n/a n/a n/a n/a Blackberry 8120 4.3.0.79 - - yes yes yes yes yes yes - - - n/a yes yes yes yes n/a n/a Blackberry 8130 Pearl (Verizon) 4.3.0.60 - - yes yes yes yes yes no - - - no yes yes yes yes n/a n/a Blackberry 8300 Curve (AT&T) 4.2.2.89 - - yes yes yes yes yes yes - - - yes n/a n/a n/a n/a n/a n/a Blackberry 8310 (AT&T) 4.2.2.181 - - yes yes yes yes yes yes - - - n/a yes yes yes yes n/a n/a Blackberry 8320 4.2.2.184 - - yes yes yes yes yes -

Skype Nu Tilgængelig for Nokia Smartphones På Ovi Marked
2010-03-03 13:39 CET Skype nu tilgængelig for Nokia smartphones på Ovi Marked Nu har over 200 millioner smartphone-brugere verden over adgang til Skype. Nokia og Skype offentliggjorde i dag, at Skype nu er tilgængelig for telefoner med styresystemet Symbian. Skype til Symbian giver Nokia smartphone- brugere verden over mulighed for at bruge Skype mens de er på farten. Skype kan downloades gratis fra Ovi Marked, og er tilgængelig for alle Nokiamobiler, der har den seneste version af Symbian. For mere information vedrørende Skype for Symbian sehttp://www.skype.com/go/symbian. Nedenfor findes den engelske pressemeddelelse samt kontaktinformation: Skype now available for Nokia smartphones in Ovi Store More than 200 million smartphone users worldwide now have Skype at their fingertips Luxembourg and Espoo, Finland - Skype and Nokia today jointly announced the release of Skype for Symbian, a Skype client for Nokia smartphones based on the Symbian platform, the world's most popular smartphone platform. Skype for Symbian will allow Nokia smartphone users worldwide to use Skype on the move, over either a WiFi or mobile data connection (GPRS, EDGE, 3G). It is now downloadable for free from the Ovi Store, Nokia's one- stop shop for mobile content. Skype for Symbian enables Nokia smartphone users to: - Make free Skype-to-Skype calls to other Skype users anywhere in the world* - Save money on calls and texts (SMS) to phones abroad - Send and receive instant messages to and from individuals or groups - Share pictures, videos and other files - Receive calls to their existing online number - See when Skype contacts are online and available to call or IM - Easily import names and numbers from the phone's address book Skype for Symbian will run on any Nokia smartphone using Symbian ^1, the latest version of the Symbian platform. -

Apple Iphone's Business Model
Sapienza – University of Rome Faculty of Engineering Master in Computer Engineering Course of “Business Models for Information Technology” Apple iPhone’s Business Model Enrico Angelini December 17th, 2009 Academic years 2009/2010 Table of Contents 1. iPhone ............................................................................................................................... 3 2. Business Model .............................................................................................................. 4 2.1 Business Model 2G (1st Generation) ............................................................................. 5 2.2 Business Model 3G (2nd Generation) ............................................................................ 8 3. App Store ....................................................................................................................... 10 3.1 A business under threat .................................................................................................. 14 3.2 Adoption Dynamics .......................................................................................................... 17 Bibliography ..................................................................................................................... 19 2 1. iPhone On Friday, June 29th, 2007, the iPhone went on sale and was sold in the US through Apple’s retail and online stores and AT&T retail stores. Apple closed its stores at 2:00 PM local time to prepare for the 6:00 PM iPhone launch, while hundreds of customers lined -
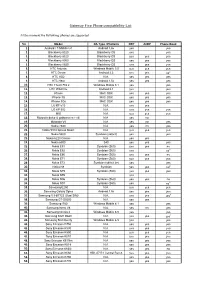
Gateway Five Phone Compatibility List
Gateway Five Phone compatibility List At the moment the following phones are supported No. Model OS Type / Platform HFP A2DP Phone Book 1. Android / T-Mobile G1 Android 1.6v yes yes 2. Blackberry 8320 Blackberry OS yes yes 3. Blackberry 8520 Blackberry OS yes yes yes 4. Blackberry 8900 Blackberry OS yes yes yes 5. Blackberry 8920 Blackberry OS yes yes yes 6. HTC Artemis Windows Mobile 5.0 yes yes yes 7. HTC Desire Android 2.2 yes yes no 2 8. HTC HD2 N.A. yes yes yes 9. HTC Hero Android 1.5v yes yes yes 10. HTC Touch Pro 2 Windows Mobile 6.1 yes yes 11. HTC Wild Fire Android 2.1 yes yes 12. iPhone MAC OSX yes yes yes 13. iPhone 3G MAC OSX yes yes yes 14. iPhone 3Gs MAC OSX yes yes yes 15. LG KF 510 N.A. yes yes 16. LG KP 502 N.A. yes yes yes 17. MIO N.A. yes yes yes 18. Motorola dolce & gabbana razr v3i N.A. yes no 19. Motorola V8 N.A. yes no yes 20. Nokia 2630 N.A. yes no yes 21. Nokia 5310 Xpress Music N.A. yes yes yes 22. Nokia 5800 Symbian (s60v3) yes yes 23. Nokia 6220 Classic N.A. yes yes 24. Nokia 6300 S40 yes yes yes 25. Nokia E51 Symbian (S60) yes yes no 26. Nokia E52 Symbian (S60) yes no 2 27. Nokia E66 Symbian (S60) yes yes no 28. Nokia E71 Symbian (S60) yes yes yes 29. Nokia E72 Symbian (s60v3 2e) yes yes 30. -
Design of a Miniaturized Imaging System for As-Built Performance
Rose-Hulman Institute of Technology Rose-Hulman Scholar Graduate Theses - Physics and Optical Engineering Physics and Optical Engineering Fall 11-23-2020 Design of a Miniaturized Imaging System for As-built Performance Jake Joo Follow this and additional works at: https://scholar.rose-hulman.edu/dept_optics Design of a Miniaturized Imaging System for As-built Performance A Thesis Submitted to the Faculty of Rose-Hulman Institute of Technology by Jake Joo In Partial Fulfillment of the Requirements for the Degree of Master of Science in Optical Engineering November 2020 © 2020 Jake Joo ROSE-HULMAN INSTITUTE OF TECHNOLOGY Final Examination Report Joonha Joo Optical Engineering Name Graduate Major Thesis Title ____________________________________________________Design of a Miniaturized Imaging System for As-Built Performance ______________________________________________________________ DATE OF EXAM: November 23, 2020 EXAMINATION COMMITTEE: Thesis Advisory Committee Thesis Advisor: Hossein Alisafaee PHOE Azad Siahmakoun PHOE Jay McCormack ME X PASSED ___________ FAILED ___________ ABSTRACT Jake Joo M.S.O.E. Rose-Hulman Institute of Technology November 2020 Design of a Miniaturized Imaging System for As-Built Performance Thesis Advisor: Dr. Hossein Alisafaee During the past two decades, many advancements in the field of optical design have occurred. Some of the more recent topics and concepts regarding optical system design are complex and require a comprehensive understanding of aberration theory, in-depth knowledge and experience with optical design software, and extensive lens design experience. This thesis focuses on the development and application of simpler methods for successful lens design for standard and miniaturized imaging systems. The impact of manufacturing tolerances of an optical system is considered, analyzed, and tested.