Care Process Models Urinary Tract Infection in Adults
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Antibiotic Susceptibility of Bacterial Strains Causing Asymptomatic Bacteriuria in Pregnancy: a Cross- Sectional Study in Harare, Zimbabwe
MOJ Immunology Antibiotic Susceptibility of Bacterial Strains causing Asymptomatic Bacteriuria in Pregnancy: A Cross- Sectional Study in Harare, Zimbabwe Abstract Research Article Background and objective antibiotic susceptibility pattern: Effective among treatmentisolated bacterial of asymptomatic species among bacteriuria pregnant in Volume 6 Issue 1 - 2018 pregnancy requires susceptible drugs. The aim of this study was to determine womenMaterials with and asymptomatic Methods bacteriuria. : This study was conducted at 4 selected primary health 1Department of Nursing Science, University of Zimbabwe, care facilities in Harare, including pregnant women registering for antenatal Zimbabwe care at gestation between 6 and 22 weeks and without urinary tract infection 2Department of Medical Microbiology, University of Zimbabwe, symptoms. Asymptomatic bacteriuria was diagnosed by culture test of all Zimbabwe 3 midstream urine samples following screening by Griess nitrate test. Susceptibility Department of Obstetrics and Gynaecology, University of Zimbabwe, Zimbabwe test was done for all positive 24 hour old culture using the disk diffusion test. The resistant and intermediate. 4Institute of Clinical Medicine, University of Oslo, Norway minimum inhibitory concentration was measured and categorized as susceptible, Results *Corresponding author: : Tested antibiotics included gentamycin (88.2%), ceftriaxone (70.6%), Department of Nursing Science,Judith Mazoe Musona Street, Rukweza, PO Box nitrofurantoin (76.5%), ciprofloxacin (82.4%), ampicillin (67.6%) and norfloxacin University of Zimbabwe, College of Health Sciences, (61.8%). Prevalence of asymptomatic bacteriuria was 14.2% (95% CI, 10.28% to 19.22%). Coagulase negative staphylococcus was the most popular (29.4%) A198, Harare, Zimbabwe, Tel: 00263773917910; Email: bacteria followed by Escherichia coli (23.5%). Gentamycin (83.3%), ciprofloxacin Received: | Published: (75%) and ceftriaxone (70.8) overally had the highest sensitivity. -

CMS Manual System Human Services (DHHS) Pub
Department of Health & CMS Manual System Human Services (DHHS) Pub. 100-07 State Operations Centers for Medicare & Provider Certification Medicaid Services (CMS) Transmittal 8 Date: JUNE 28, 2005 NOTE: Transmittal 7, of the State Operations Manual, Pub. 100-07 dated June 27, 2005, has been rescinded and replaced with Transmittal 8, dated June 28, 2005. The word “wound” was misspelled in the Interpretive Guidance section. All other material in this instruction remains the same. SUBJECT: Revision of Appendix PP – Section 483.25(d) – Urinary Incontinence, Tags F315 and F316 I. SUMMARY OF CHANGES: Current Guidance to Surveyors is entirely replaced by the attached revision. The two tags are being combined as one, which will become F315. Tag F316 will be deleted. The regulatory text for both tags will be combined, followed by this revised guidance. NEW/REVISED MATERIAL - EFFECTIVE DATE*: June 28, 2005 IMPLEMENTATION DATE: June 28, 2005 Disclaimer for manual changes only: The revision date and transmittal number apply to the red italicized material only. Any other material was previously published and remains unchanged. However, if this revision contains a table of contents, you will receive the new/revised information only, and not the entire table of contents. II. CHANGES IN MANUAL INSTRUCTIONS: (N/A if manual not updated.) (R = REVISED, N = NEW, D = DELETED) – (Only One Per Row.) R/N/D CHAPTER/SECTION/SUBSECTION/TITLE R Appendix PP/Tag F315/Guidance to Surveyors – Urinary Incontinence D Appendix PP/Tag F316/Urinary Incontinence III. FUNDING: Medicare contractors shall implement these instructions within their current operating budgets. IV. ATTACHMENTS: Business Requirements x Manual Instruction Confidential Requirements One-Time Notification Recurring Update Notification *Unless otherwise specified, the effective date is the date of service. -

Investigation of Urine 2015
UK Standards for Microbiology Investigations Investigation of Urine 2015 OCTOBER 5 - SEPTEMBER 7 BETWEEN ON CONSULTED WAS DOCUMENT THIS - DRAFT Issued by the Standards Unit, Microbiology Services, PHE Bacteriology | B 41 | Issue no: dl+ | Issue date: dd.mm.yy <tab+enter> | Page: 1 of 46 © Crown copyright 2015 Investigation of Urine Acknowledgments UK Standards for Microbiology Investigations (SMIs) are developed under the auspices of Public Health England (PHE) working in partnership with the National Health Service (NHS), Public Health Wales and with the professional organisations whose logos are displayed below and listed on the website https://www.gov.uk/uk- standards-for-microbiology-investigations-smi-quality-and-consistency-in-clinical- laboratories. SMIs are developed, reviewed and revised by various working groups which are overseen by a steering committee (see https://www.gov.uk/government/groups/standards-for-microbiology-investigations- steering-committee). 2015 The contributions of many individuals in clinical, specialist and reference laboratories who have provided information and comments during the development of this document are acknowledged. We are grateful to the Medical Editors for editingOCTOBER the 5 medical content. - For further information please contact us at: Standards Unit Microbiology Services Public Health England SEPTEMBER 61 Colindale Avenue 7 London NW9 5EQ E-mail: [email protected] Website: https://www.gov.uk/uk-standards-forBETWEEN-microbiology -investigations-smi-quality- and-consistency-in-clinical-laboratories -

Urinary Tract Infection (Uti) Fact Sheet
URINARY TRACT INFECTION (UTI) FACT SHEET Overview A urinary tract infection (UTI) is an infection that involves any part of the urinary tract, including the kidneys, bladder and urethra. It is usually caused by exposure of the urinary tract to a fecal organism such as Escherichia coli (E. coli) but also may be caused by other organisms. An indwelling urinary catheter is a drainage tube that is inserted into the urinary bladder through the urethra, is left in place and is connected to a closed urine collection system. Urinary tract infections in patients with an indwelling urinary catheter are called catheter-associated UTIs, or CAUTIs. Signs and Symptoms Common symptoms of UTI include: • fever; • pain or burning in the lower abdomen; • burning during urination; • an increase in the frequency of urination; and • cloudy appearing urine. Causes and Transmission A UTI occurs when germs (usually bacteria) enter the urinary tract through the meatus (the opening of the urinary tract). These germs then cause infection. The urinary tract is normally sterile, meaning it contains no germs. A CAUTI occurs when germs (usually bacteria) enter the urinary tract through the urinary catheter and cause infection. This can occur when health care worker hands are not properly cleaned before the insertion of a catheter or during the process of cleaning or emptying of the urine collection system. Risk Factors Sexually active women, people with blockages in the urinary tract, such as prostate enlargement, and women using certain types of birth control, such as diaphragms, or those who are undergoing menopause are at higher risk of UTI. -

Prevalence of Urinary Tract Infection and Antibiotic Resistance Pattern in Pregnant Women, Najran Region, Saudi Arabia
Vol. 13(26), pp. 407-413, August, 2019 DOI: 10.5897/AJMR2019.9084 Article Number: E3F64FA61643 ISSN: 1996-0808 Copyright ©2019 Author(s) retain the copyright of this article African Journal of Microbiology Research http://www.academicjournals.org/AJMR Full Length Research Paper Prevalence of urinary tract infection and antibiotic resistance pattern in pregnant women, Najran region, Saudi Arabia Ali Mohamed Alshabi1*, Majed Saeed Alshahrani2, Saad Ahmed Alkahtani1 and Mohammad Shabib Akhtar1 1Department of Clinical Pharmacy, College of Pharmacy, Najran University, Najran, Saudi Arabia. 2Department of Obstetics and Gyneocology, Faculty of Medicine, Najran University, Najran, Saudi Arabia. Received 25 February, 2019; Accepted August 5, 2019 Urinary Tract Infection (UTI) is one of the commonest infectious disease in pregnancy, and in pregnancy we have very limited number of antibiotics to treat the UTI. This study was conducted on 151 patients who attended the gynecology clinic during the study period. Nineteen UTI proven cases of UTI were studied for prevalence of microorganism and sensitivity pattern against different antibiotics. Among the bacteria isolated, Escherichia coli (73.68%) and Staphylococcus aureus (10.52%) were the most prevalent Gram negative and Gram positive bacteria respectively. To know the resistance pattern of microorganism we used commercially available discs of different antibiotics. Gram negative bacteria showed more resistance as compared to Gram positive one. It is observed that the most effective antibiotic for Gram negative isolates is Ceftriaxone (87.5%), followed by Amoxicillin + Clavulanic acid (81.25%), Amikacin (75%), Cefuroxime (75%), Cefixime (68.75%) and Mezlocillin (62.5%). For the Gram positive bacteria, Ceftriaxone, Amikacin and Amoxicillin + Clavulanic acid were the most effective antimicrobials (100%). -
Breaking the Cycle Asymptomatic Bacteriuria
Breaking the Cycle Asymptomatic Bacteriuria Urinary tract infection (UTI) is the most common indication for antibiotic use in post-acute care facilities and a significant proportion of this use is inappropriate and unnecessary. Asymptomatic bacteriuria (ASB) is prevalent in residents of post-acute care facilities and is frequently misidentified as a “UTI”. www.preventHAIaz.gov For comments or question please contact: [email protected] Definitions: ASB refers to bacteria in the urine at levels often regarded as clinically significant (>100,000 colonies/ml) but with no symptoms or localizing signs suggestive of UTI. Pyuria (>10 WBC/ hpf) accompanying ASB is not an indication for antibiotic treatment. Ordering of UA/C&S: The ‘Choosing Wisely’ guideline from the American Medical Directors Association (AMDA) recommends against obtaining urine studies unless there are clear signs and symptoms that localize to the urinary tract. Multiple studies have also shown that confusion or altered mental status is not a reliable indication for urine studies. Such studies often lead to unnecessary antibiotic treatment. Urine studies are not recommended for: • Change in urine color, odor or turbidity – these are typically due to resident hydration and not indicators of infection • Catheterized residents while the catheter remains in situ. This includes both Foley and suprapubic catheters • After a patient fall Common ways ASB masquerades as an infection requiring antibiotic treatment: requiring antibiotic as an infection ASB masquerades Common ways • To document -

233 the Use of Absorbent Pads Increases the Risk For
233 Omli R1, Skotnes L H1, Romild U1, Kuhry E1 1. Namsos Hospital THE USE OF ABSORBENT PADS INCREASES THE RISK FOR LOWER URINARY TRACT INFECTIONS IN NURSING HOMES RESIDENTS. Hypothesis / aims of study Urinary incontinence is a common medical problem in the nursing home population. The aim of this study was to determine whether use of absorbent pads is a risk factor for the development of lower urinary tract infections in nursing home residents. Introduction Lower urinary tract infections (UTIs) are a common medical problem in the elderly. Different kinds of absorbent products, such as diapers, pad and pant combinations, are used in incontinence care. In some cases, indwelling catheters, external condom catheters or in-and-out catheterisation are options for managing bladder dysfunction. About 23% of the residents in nursing homes don’t need toilet assistance. That means that the majority of residents is dependent on help from nursing staff for toileting and help to change soiled absorbent pads. Transmission of bacteria during incontinence care is associated with UTIs in elderly. In the vulnerable nursing home population, UTIs are a frequent problem and can lead to increased morbidity and even mortality. The prevalence of UTIs in nursing home residents is approximately 30%. Improving hand hygiene among staffing in nursing homes is one of the most important and effective methods to reduce hand born transmission of pathological microbes. Studies in long-term-care facilities document a lack of hand hygiene in connection to staff-resident interactions. This study studies the association between the use of absorbent pads and symptomatic UTIs in the nursing home population. -
Module 3: Benign Prostatic Hypertrophy
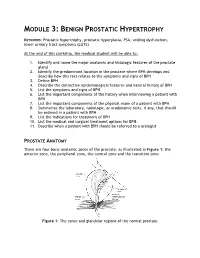
MODULE 3: BENIGN PROSTATIC HYPERTROPHY KEYWORDS: Prostatic hypertrophy, prostatic hyperplasia, PSA, voiding dysfunction, lower urinary tract symptoms (LUTS) At the end of this clerkship, the medical student will be able to: 1. Identify and name the major anatomic and histologic features of the prostate gland 2. Identify the predominant location in the prostate where BPH develops and describe how this fact relates to the symptoms and signs of BPH 3. Define BPH 4. Describe the distinctive epidemiological features and natural history of BPH 5. List the symptoms and signs of BPH 6. List the important components of the history when interviewing a patient with BPH 7. List the important components of the physical exam of a patient with BPH 8. Summarize the laboratory, radiologic, or urodynamic tests, if any, that should be ordered in a patient with BPH 9. List the indications for treatment of BPH 10. List the medical and surgical treatment options for BPH. 11. Describe when a patient with BPH should be referred to a urologist PROSTATE ANATOMY There are four basic anatomic zones of the prostate, as illustrated in Figure 1: the anterior zone, the peripheral zone, the central zone and the transition zone. Figure 1: The zones and glandular regions of the normal prostate. The anterior zone is entirely fibromuscular and non-glandular, and it appears to have little significance in prostatic function or pathology. This area comprises approximately 20% of the bulk of prostatic tissue. The peripheral zone is composed entirely of acinar tissue. It comprises the posterior surface of the prostate, including the apical, lateral, posterolateral and anterolateral portions of the prostate. -

Urinary Incontinence ! ! !What Is Urinary Incontinence? Leakage of Urine Is Called Urinary Incontinence
! ! ! Urinary Incontinence ! ! !What is urinary incontinence? Leakage of urine is called urinary incontinence. Some women leak small amounts of !urine. At other times, leakage of urine is frequent or severe. !Are there different types of urinary incontinence? !There are several types of urinary incontinence: • Stress urinary incontinence is loss of urine when a woman coughs, laughs, or sneezes. Leaks also can happen when a woman walks, runs, or exercises. It is caused by a weakening of the tissues that support the bladder or the muscles of the ! urethra. • Urge incontinence is leakage of urine caused by overactive bladder muscles that ! contract too often or problems with the nerves that send signals to the bladder !• Mixed incontinence is a combination of both stress and urge incontinence symptoms • Overflow incontinence is a steady loss of small amounts of urine when the bladder does not empty all the way during voiding. It can be caused by an underactive bladder ! muscle or blockage of the urethra. !What are the symptoms of urinary incontinence? !In addition to leaking urine, a woman with incontinence also may have other symptoms: • Urgency— A strong urge to urinate whether or not the bladder is full, often with pelvic ! pressure !• Frequency— Voiding more often than she considers usual !• Nocturia — The need to void during hours of sleep !• Dysuria — Painful voiding !• Enuresis— Bed-wetting or leaking while sleeping ! What causes urinary incontinence? ! Urinary incontience can have short-term causes and long-term causes. Short-term !causes are easier to treat and include the following: • Urinary tract infection— Loss of bladder control may be caused by an infection of the urinary tract. -

Frequently Asked Questions About Overactive Bladder
ABOUT OAB Frequently Asked Questions about Overactive Bladder What is Overactive Bladder (OAB)? If you live with OAB, you may also: Overactive Bladder (OAB) isn’t a disease. It’s the u Leak urine (incontinence): Sometimes people name of a group of urinary symptoms. The most with OAB also have “urgency incontinence.” common symptom of OAB is a sudden urge to This means that urine leaks when you feel urinate that you can’t control. Some people will the sudden urge to go. This isn’t the same as leak urine when they feel this urge. Having to “stress urinary incontinence” or “SUI.” People urinate many times during the day and night is with SUI leak urine while sneezing, laughing or another symptom of OAB. doing other physical activities. (You can learn more about SUI at UrologyHealth.org/SUI.) How common is OAB? u Urinate frequently: You may also need to go OAB is common. It affects millions of Americans. to the bathroom many times during the day. As many as 30 percent of men and 40 percent The number of times someone urinates varies of women in the United States live with OAB from person to person. But many experts symptoms. agree that going to the bathroom more than eight times in 24 hours is “frequent urination.” Who is at risk for OAB? u Wake up at night to urinate: Waking from As you grow older, you’re at higher risk for sleep to go to the bathroom more than once a OAB. But no matter what your age, there are night is another symptom of OAB. -

UTI) Using Urinary Nitrite and Significant Bacteriuria (SBU
Available online at www.ijmrhs.com International Journal of Medical Research & ISSN No: 2319-5886 Health Sciences, 2016, 5, 4:6-15 Comparative diagnosis of urinary tract infection (UTI) using urinary nitrite and significant bacteriuria (SBU) 1John Anuli S., 2Mboto Clement I. and *2Agbo Bassey E. 1Department of General Studies, College of Health Technology, Calabar, Nigeria 2Department of Microbiology, Faculty of Biological Sciences, University of Calabar,P.M.B. 1115, Calabar, Nigeria *Corresponding Authors E-mail: [email protected] _____________________________________________________________________________________________ ABSTRACT The clinical laboratory diagnosis of urinary tract infection was compared in two hundred (200) midstream urine samples using bacteria culture and urinary nitrite detection technique. The comparative susceptibility of the isolates to common antibiotics was evaluated using completely randomized design (CRD). The minimum inhibitory concentration (MIC) and minimum bactericidal concentration (MBC) for each antibiotics test was evaluated using standard laboratory procedures. Approximately fifty one percent (101/200) of urine samples that were culture yielded significant bacteriuria (SBU) as compared to (32.59%, 65/200) which had positive nitrite detection. Also eighteen percent (18%, 35/200) of the negative nitrite detection test showed evidence of significant bacteriuria. Significant bacteriuria was significantly associated at p <0.05 with culture isolation technique. A total of nine (9) different bacterial isolates were detected in this study. The isolates and their frequency of occurrence were Escherichia coli 30(29.7%), Pseudomonas aeruginosa 15(14.9%), Klebsiella pneumonia 13(12.8%), Enterococcus faecalis and Citrobacterfreundii 10(9.9), Proteus mirabilis 9(8.9), Staphylococcus aureus 8(7.7%), Serretiamarcesens and Streptococcus specie 3(3.0%).The mean total viable count ranged from 31.50±3.15x10 7cfuml -1 to 262.5±1.09x10 8cfuml -1. -

Method for the Detection of Significant Bacteriuria in Large Groups of Patients
J Clin Pathol: first published as 10.1136/jcp.17.5.498 on 1 September 1964. Downloaded from J. clin. Path. (1964), 17, 498 Method for the detection of significant bacteriuria in large groups of patients D. A. LEIGH AND J. D. WILLIAMS From the Department of Pathology, Edgware General Hospital SYNOPSIS A measured area of blotting paper was used as a vehicle for transferring a constant aliquot of urine on to the surface of a culture medium. The number of bacterial colonies growing in the inoculum area of the medium corresponded to the number of organisms in the urine. One thousand, two hundred and seventy-five urines from women attending an ante-natal clinic were tested by this method, and the results compared with the results of quantitative bacterial counting and of triphenyl tetrazolium chloride (T.T.C.) tests. The method was found to be a simple, cheap, and reliable way of screening urine specimens for significant bacteriuria. The increased incidence of urinary tract infection, METHODS often persisting asymptomatically, which has been found in certain sections of the population, notably THE PAPER STRIP A Postlip Mill 633 fibre-free, fluffless pregnant women (Kaitz and Hodder, 1961; Monzon, paper supplied to the laboratory for use as blotting paper was used for the paper strips. Strips were cut 3 in. long Armstrong, Pion, Deigh, and Hewitt, 1963), has led by i in. wide and a fold was made across the strip i copyright. in. to a search for screening tests which are simple to from one end (Fig. 1). The X in.