Pediatric Mental Health Guidelines
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Formulary and Prescribing Guidelines
Formulary and Prescribing Guidelines SECTION 1: TREATMENT OF DEPRESSION Section 1. Treatment of depression 1.1 Introduction This guidance should be considered as part of a stepped care approach in the management of depressive disorders. Antidepressants are not routinely recommended for persistent sub-threshold depressive symptoms or mild depression but can be considered in these categories where there is a past history of moderate or severe depression, initial presentation of sub-threshold depressive symptoms for at least 2 years, and persistence of either mild or sub-threshold depression after other interventions1 have failed. The most current NICE guidance should be consulted wherever possible to obtain the most up to date information. For individuals with moderate or severe depression, a combination of antidepressant medication and a high intensity psychological intervention (CBT or IPT) is recommended. When depression is accompanied by symptoms of anxiety, usually treat the depression first. If the person has an anxiety disorder and co-morbid depression or depressive symptoms, consider treating the anxiety first. Also consider offering advice on sleep hygiene, by way of establishing regular sleep and wake times; avoiding excess eating, avoiding smoking and drinking alcohol before sleep; and taking regular physical exercise if possible. Detailed information on the treatment of depression in children and adolescents can be found in section 12. Further guidance on prescribing for older adults and for antenatal/postnatal service users can be found in section 11 and section 20, respectively. 1.2 Approved Drugs for the treatment of Depression in Adults For licensing indications, see Annex 1 Drug5 Formulation5 Comments2,3,4 Caps 20mg, 60mg Selective serotonin reuptake inhibitor (SSRI) Fluoxetine Liquid 20mg/5ml 1st line SSRI (based on acquisition cost) Tabs 10mg, 25mg, 50mg Amitriptyline Tricyclic (TCA). -

Switching from Clonidine Immediate-Release to Guanfacine Extended-Release
/ DE L’ACADÉMIE CANADIENNE DE PSYCHIATRIE DE L’ENFANT ET DE L’ADOLESCENT PSYCHOPHARMACOLOGY Switching from Clonidine Immediate-Release to Guanfacine Extended-Release Dean Elbe PharmD, BCPP1,2,3 s a clinical pharmacy specialist in child and adolescent (Canada) Ltd, 2012b). Clonidine has been used off-label Amental health, I am frequently asked how to switch in children for many years for treatment of insomnia, patients from clonidine immediate-release (IR) to guanfa- ADHD, and disruptive behaviour disorders (Hunt, Capper cine extended-release (XR). This therapeutic switch may be & O’Connell, 1990; Rubinstein; Jaselskis, Cook, Fletcher required when poor adherence to a clonidine IR regimen & Leventhal, 1992; Silver & Licamele, 1994; Palumbo et (typically requiring 3–4 doses daily) is identified, when al., 2008; Efron, Lycett & Sciberras, 2014). A clonidine XR clonidine dose-optimization is limited by sedation, brady- formulation is not available in Canada, but is available in cardia or hypotension, or when coverage situations change. the United States for treatment of ADHD (Concordia Phar- The latter may occur if, for example, new eligibility for a maceuticals, Inc. 2015). government program or a third party-payer occurs. Weight-based dosing guidelines exist for clonidine IR Guanfacine XR, a selective alpha2A agonist, was first mar- (0.003–0.008 mg/kg/day) and guanfacine XR (0.05–0.08 keted in Canada in late 2013 for the treatment of attention mg/kg/day) (Shire Pharma Canada ULC, 2019; Elbe et deficit hyperactivity disorder (ADHD) in children and ado- al., 2018). Based on these guidelines and other literature, lescents (Shire Pharma Canada ULC, 2019). -
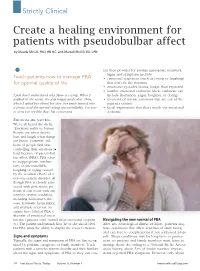
Create a Healing Environment for Patients with Pseudobulbar Affect by Maude Mcgill, Phd, RN-BC, and Marzell Mcgill, BA, LPN
Strictly Clinical Create a healing environment for patients with pseudobulbar affect By Maude McGill, PhD, RN-BC, and Marzell McGill, BA, LPN tact their provider for prompt appropriate treatment. • Signs and symptoms include: Teach patients how to manage PBA • emotional responses (such as crying or laughing) for optimal quality of life. that don’t fit the situation • emotional episodes lasting longer than expected • sudden emotional outbursts (these outbursts can I just don’t understand why Mom is crying. When I include frustration, anger, laughter, or crying) walked in the room, she was happy and calm. Then, • moments of intense emotions that are out of the when I asked her about her day, her smile turned into patient’s control a frown and she started crying uncontrollably. I’ve nev - • facial expressions that don’t match the emotional er seen her cry like that. I’m concerned. response. EMOTIONS ARE NATURAL . We’ve all heard the cliché, “Emotions make us human.” People cry when they’re hurt and laugh when things are funny. However, mil - lions of people find that controlling their emotions is hard because of pseudobul - bar affect (PBA). PBA refers to inappropriate, involun - tary, or uncontrollable laughing or crying caused by the residual effects of a nervous system disorder. Al - though PBA is closely asso - ciated with post-stroke pa - tients, it can occur with any nervous system condition, including Alzheimer’s dis - ease, traumatic brain injury, and multiple sclerosis. Sci - entists have labeled PBA a disorder of emotional incon - tinence (patients can’t control their emotional respons - Navigating the new normal of PBA es). -

ADHD Parents Medication Guide Revised July 2013
ADHD Parents Medication Guide Revised July 2013 Attention-Deficit/Hyperactivity Disorder Prepared by: American Academy of Child & Adolescent Psychiatry and American Psychiatric Association Supported by the Elaine Schlosser Lewis Fund Physician: ___________________________________________________ Address: ___________________________________________________ ___________________________________________________ ___________________________________________________ Phone: ___________________________________________________ Email: ___________________________________________________ ADHD Parents Medication Guide – July 2013 2 Introduction Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterized by difficulty paying attention, excessive activity, and impulsivity (acting before you think). ADHD is usually identified when children are in grade school but can be diagnosed at any time from preschool to adulthood. Recent studies indicate that almost 10 percent of children between the ages of 4 to 17 are reported by their parents as being diagnosed with ADHD. So in a classroom of 30 children, two to three children may have ADHD.1,2,3,4,5 Short attention spans and high levels of activity are a normal part of childhood. For children with ADHD, these behaviors are excessive, inappropriate for their age, and interfere with daily functioning at home, school, and with peers. Some children with ADHD only have problems with attention; other children only have issues with hyperactivity and impulsivity; most children with ADHD have problems with all three. As they grow into adolescence and young adulthood, children with ADHD may become less hyperactive yet continue to have significant problems with distraction, disorganization, and poor impulse control. ADHD can interfere with a child’s ability to perform in school, do homework, follow rules, and develop and maintain peer relationships. When children become adolescents, ADHD can increase their risk of dropping out of school or having disciplinary problems. -
Reveiw Week 3 Final with Questions
REVIEW 3 SOMATIZATION AND RELATED DISORDERS SOMATIZATION AND RELATED DISORDERS SOMATIZATION ▸ Psychological problems or concerns that are converted into and communicated as physical distress ▸ Anxiety is either Conscious or Unconscious ▸ Physical Illness is Real SOMATIZATION AND RELATED DISORDERS - SSD SOMATIC SYMPTOM DISORDER A. One or more somatic symptoms that are distressing or result in significant disruption of daily life B. Excessive thoughts, feelings, or behaviors related to the somatic symptoms or associated health concerns as manifested by at least one of the following 1. Disproportionate and persistent thoughts about the seriousness or one’s symptoms 2. Persistently high level of anxiety about health or symptoms 3. Excessive time and energy devoted to these symptoms or health concerns C. Although any one somatic symptom may not be continuously present, the state of being symptomatic is persistent (typically more than 6 months) SOMATIZATION AND RELATED DISORDERS - SSD TREATMENT ▸ Regular office visits with the same physician ▸ Psychotherapy ▸ Validate the patient’s feelings/experience of symptoms SOMATIZATION AND RELATED DISORDERS - ILLNESS ANXIETY DISORDER ILLNESS ANXIETY DISORDER A. Formerly hypochondriasis B. Preoccupation with having or acquiring a serious illness C. Somatic symptoms are not present or, if present, are only mild in intensity. If another medical condition is present or there is a high risk for developing a medical condition (strong FH), the preoccupation is clearly excessive or disproportionate D. There is a high level of anxiety about health, and the individual is easily alarmed about personal health status (preoccupation with idea one is sick) E. The individual performs excessive health-related behaviors (checking body) or exhibits maladaptive avoidance (avoids doctors) F. -

Memory Deficits Associated with Clonidine
Letter to the Editor Letters to the Editor are invited for comment on a topic of current interest or on Table material published in GENERAL HOSPITAL PSYCHIATRY. Letters should be typed doubled spaced and are subject to editing according to space limitations. - Memory Deficits Associated with Attent KnO Clonidine WA Verbal WA Drugs used in the treatment of essential hyperten- Initiation of clonidine therapy (0.1 mg b.i.d.) in WA sion are among the most commonly prescribed. April 1984 resulted in well-controlled hypertension Tactilc Some of these agents have primary effects on neu- without immediately apparent adverse effects. Fulc rotransmitter systems and are centrally active. However, the coincidence of the onset of memory Verba Thus, drugs such as a-methyldopa, propranalol, complaints and the beginning of clonidine treat- 3% ment suggested that clonidine might be respon- List Ll and reserpine have well-established neuropsychia- Fulc tric complications, ranging from depression to cog- sible. si nitive impairments and psychosis [l].Since the use After consultation with the patient's internist, a R of these drugs is widespread and unavoidable, we switch was made to captopril, an angiotensin-con- T must be alert to the possibility that these drugs verting enzyme inhibitor. Before the change we T administered tests of attention, concentration, and contribute to psychologic complaints and symp- -R toms of our patients. verbal skills as well as the Fuld Object-Memory Evaluation, which includes a measure of verbal 'Age-a Clonidine, a presynaptic adrenergic a2agonist, bNonc has become well established as a useful and rela- fluency as well as a selective reminding list learning tively safe therapeutic agent. -

THE USE of MIRTAZAPINE AS a HYPNOTIC O Uso Da Mirtazapina Como Hipnótico Francisca Magalhães Scoralicka, Einstein Francisco Camargosa, Otávio Toledo Nóbregaa
ARTIGO ESPECIAL THE USE OF MIRTAZAPINE AS A HYPNOTIC O uso da mirtazapina como hipnótico Francisca Magalhães Scoralicka, Einstein Francisco Camargosa, Otávio Toledo Nóbregaa Prescription of approved hypnotics for insomnia decreased by more than 50%, whereas of antidepressive agents outstripped that of hypnotics. However, there is little data on their efficacy to treat insomnia, and many of these medications may be associated with known side effects. Antidepressants are associated with various effects on sleep patterns, depending on the intrinsic pharmacological properties of the active agent, such as degree of inhibition of serotonin or noradrenaline reuptake, effects on 5-HT1A and 5-HT2 receptors, action(s) at alpha-adrenoceptors, and/or histamine H1 sites. Mirtazapine is a noradrenergic and specific serotonergic antidepressive agent that acts by antagonizing alpha-2 adrenergic receptors and blocking 5-HT2 and 5-HT3 receptors. It has high affinity for histamine H1 receptors, low affinity for dopaminergic receptors, and lacks anticholinergic activity. In spite of these potential beneficial effects of mirtazapine on sleep, no placebo-controlled randomized clinical trials of ABSTRACT mirtazapine in primary insomniacs have been conducted. Mirtazapine was associated with improvements in sleep on normal sleepers and depressed patients. The most common side effects of mirtazapine, i.e. dry mouth, drowsiness, increased appetite and increased body weight, were mostly mild and transient. Considering its use in elderly people, this paper provides a revision about studies regarding mirtazapine for sleep disorders. KEYWORDS: sleep; antidepressive agents; sleep disorders; treatment� A prescrição de hipnóticos aprovados para insônia diminuiu em mais de 50%, enquanto de antidepressivos ultrapassou a dos primeiros. -

IHH Notification Form Guide
Integrated Health Home Health Home Notification Form Guide Introduction This is to assist in providing the Health Home with information on criteria and how to enroll the member into an Integrated Health Home (IHH). Enrollment Criteria Member needs to 1. Be eligible for Medicaid. 2. Have 1 or more Serious Mental Illness (SMI) or Serious Emotional Disturbance (SED). 3. Meet the Functional Impairment (FI) as determined by a Licensed Mental Health Professional. SMI & SED Definitions Diagnosis must be determined by use the Diagnostic and Statistical Manual (DSM) of Mental Disorders published by the American Psychiatric Association or its most recent International Classification of Diseases (ICD). SMI is defined as an Adult that has a persistent or chronic mental illness, a behavioral, or emotional disorder that causes serious functional impairment and substantially interferes with or limits one or more major life activities including functioning in the family, school, employment or community. SMI may co-occur with substance use disorder, developmental, neurodevelopmental or intellectual disabilities but those diagnoses may not be the clinical focus for health home services. SED is defined by a Child having a diagnosable mental, behavioral or emotional disorder which results in a functional impairment that substantially interferes with or limits the child’s role or functioning in family, school, or community activities. SED may co-occur with substance use disorder, developmental, neurodevelopmental or intellectual disabilities but those diagnoses may not be the clinical focus for health home services. Mental Health Professional Definition Mental health professional meets all of the following conditions: 1. Holds at least a master’s degree in a mental health field including, but not limited to, psychology, counseling and guidance, psychiatric nursing and social work; or is a doctor of medicine or osteopathic medicine; and 2. -

Mirtazapine (Remeron)
What is most important to remember? If you have questions: Strong Internal Medicine • It may take a few weeks for you to see the benefits of taking this Ask your doctor, nurse or pharmacist for medicine more information about mirtazapine (Remeron®). • Do not suddenly stop taking mirtazapine; you could have unpleasant withdrawal symptoms. Talk with your doctor about how to slowly discontinue this medicine • Seek help from a doctor or pharmacist if you have thoughts of suicide or hurting yourself • This medication may impair your thinking or reactions. Be careful if Strong Internal Medicine you drive or do anything that 601 Elmwood Avenue requires you to be alert. Ambulatory Care Facility, 5th Floor Rochester, NY 14642 • Do not start any new medications, Phone: (585) 275 -7424 over-the-counter drugs or herbal Mirtazapine (Remeron®): remedies without talking to your Visit our website at: Important Patient Information www.urmc.rochester.edu/medicine/ - doctor general-medicine/patientcare/ • If you think there has been an overdose, call your poison control center or get medical care right away What does mirtazapine (Remeron®) do? What side effects could occur with mirtazapine What are some things that I need to be aware of when • It is in a class of medications called antidepressants. It (Remeron®)? taking mirtazapine (Remeron®)? works by increasing certain types of activity in the brain • Lightheaded, dizzy, or sleepy • Tell your doctor or pharmacist if you are allergic to mirtazapine, any other medicines, foods, or substances to maintain mental balance • Blurred eyesight or a change in thinking clearly • It may take a few weeks for you to see the benefits of taking • It is used to treat depression (low mood) • Constipation, dry mouth, and weight gain this medicine. -

Nuedexta, INN-Dextromethorphan/Quinidine
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT NUEDEXTA 15 mg/9 mg hard capsules 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each capsule contains dextromethorphan hydrobromide monohydrate, equivalent to 15.41 mg dextromethorphan and quinidine sulfate dihydrate, equivalent to 8.69 mg quinidine. Excipient with known effect: Each hard capsule contains 119.1 mg of lactose (as monohydrate). For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Hard capsule Brick red gelatin capsule, size 1, with “DMQ / 20-10” printed in white ink on the capsule. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications NUEDEXTA is indicated for the symptomatic treatment of pseudobulbar affect (PBA) in adults (see section 4.4). Efficacy has only been studied in patients with underlying Amyotrophic Lateral Sclerosis or Multiple Sclerosis (see section 5.1). 4.2 Posology and method of administration Posology The recommended starting dose is NUEDEXTA 15 mg/9 mg once daily. The recommended dose titration schedule is outlined below: Week 1 (day 1-7): The patient should take one NUEDEXTA 15 mg/9 mg capsule once daily, in the morning, for the initial 7 days. Weeks 2-4 (day 8-28): The patient should take one NUEDEXTA 15 mg/9 mg capsule, two times per day, one in the morning and one in the evening, 12-hours apart, for 21 days. From Week 4 on: If the clinical response with NUEDEXTA 15 mg/9 mg is adequate, the dose taken in weeks 2-4 should be continued. 2 If the clinical response with NUEDEXTA 15 mg/9 mg is inadequate, NUEDEXTA 23 mg/9 mg should be prescribed, taken two times per day, one in the morning and one in the evening, 12 hours apart. -
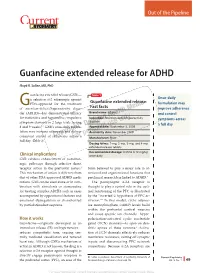
Guanfacine Extended Release for ADHD
Out of the Pipeline p Guanfacine extended release for ADHD Floyd R. Sallee, MD, PhD uanfacine extended release (GXR)— Table 1 α Once-daily a selective -2 adrenergic agonist Guanfacine extended release: GFDA-approved for the treatment formulation may of attention-defi cit/hyperactivity disor- Fast facts improve adherence der (ADHD)—has demonstrated effi cacy Brand name: Intuniv and control for inattentive and hyperactive/impulsive Indication: Attention-defi cit/hyperactivity symptoms across disorder symptom domains in 2 large trials lasting® Dowden Health Media a full day 8 and 9 weeks.1,2 GXR’s once-daily formu- Approval date: September 3, 2009 lation may increase adherence and deliver Availability date: November 2009 consistent control of symptomsCopyright across a For personalManufacturer: use Shire only full day (Table 1). Dosing forms: 1-mg, 2-mg, 3-mg, and 4-mg extended-release tablets Recommended dosage: 0.05 to 0.12 mg/kg Clinical implications once daily GXR exhibits enhancement of noradren- ergic pathways through selective direct receptor action in the prefrontal cortex.3 brain believed to play a major role in at- This mechanism of action is different from tentional and organizational functions that that of other FDA-approved ADHD medi- preclinical research has linked to ADHD.3 cations. GXR can be used alone or in com- The postsynaptic α-2A receptor is bination with stimulants or atomoxetine thought to play a central role in the opti- for treating complex ADHD, such as cases mal functioning of the PFC as illustrated accompanied by oppositional features and by the “inverted U hypothesis of PFC ac- emotional dysregulation or characterized tivation.”4 In this model, cyclic adenos- by partial stimulant response. -

What's New in Psychopharmacology
Wednesday, 3:00 – 4:30, F2 What's New in Psychopharmacology Joel M. Sanchez, MD [email protected] Objectives: Identify advances in clinical assessment and management of selected healthcare issues related to persons with developmental disabilities Notes: 4/7/2016 What’s New in Nuedexta Psychopharmacology • A new medication for pseudobulbar affect (PBA) • Pseudobulbar Affect: Joel M. Sanchez, M.D. • Frequent, uncontrollable outbursts of crying or laughing in people with certain neurologic conditions or brain injuries Diplomate of the American Board of Psychiatry and Neurology, Psychiatry • Episodes may occur several times per day and can last seconds to minutes Diplomate of the American Board of Psychiatry and Neurology, Child/Adolescent Psychiatry • “emotional incontinence” • “pathological laughing and crying” The Right Door for Hope, Recovery and Wellness Wedgwood Christian Services Turning Leaf Behavioral Health Services Community Mental Health Authority - CEI ADHD Medications Antidepressants • Stimulants • SSRIs • Adzenys XR-ODT (amphetamine extended release oral dissolving tablet) • Brintellix (vortioxetine) • Quillivant XR (methylphenidate extended release liquid) • Viibryd (vilazodone) • Daytrana (methylphenidate transdermal) • SNRIs • Non-Stimulants • Fetzima (levomilnacipran) • Clonidine (Catapres / Kapvay) • Pristiq (desvenlafaxine) • Guanfacine (Tenex / Intuniv) • Strattera (atomoxetine) Antipsychotics Blood Pressure Medications • Abilify Maintena & Aristada (aripiprazole) • What’s Old is New • Every 4 weeks or Every 4-6