A Case of Envenomation by the False Fer-De-Lance
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Uromacer Catesbyi (Schlegel) 1. Uromacer Catesbyi Catesbyi Schlegel 2. Uromacer Catesbyi Cereolineatus Schwartz 3. Uromacer Cate
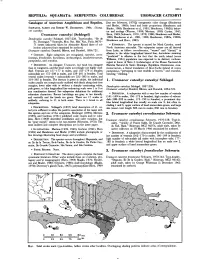
T 356.1 REPTILIA: SQUAMATA: SERPENTES: COLUBRIDAE UROMACER CATESBYI Catalogue of American Amphibians and Reptiles. [but see Schwartz,' 1970]); ontogenetic color change (Henderson and Binder, 1980); head and body proportions (Henderson and SCHWARTZ,ALBERTANDROBERTW. HENDERSON.1984. Uroma• Binder, 1980; Henderson et a\., 1981; Henderson, 1982b); behav• cer catesbyi. ior and ecology (Werner, 1909; Mertens, 1939; Curtiss, 1947; Uromacer catesbyi (Schlegel) Horn, 1969; Schwartz, 1970, 1979, 1980; Henderson and Binder, 1980; Henderson et a\., 1981, 1982; Henderson, 1982a, 1982b; Dendrophis catesbyi Schlegel, 1837:226. Type-locality, "lie de Henderson and Horn, 1983). St.- Domingue." Syntypes, Mus. Nat. Hist. Nat., Paris, 8670• 71 (sexes unknown) taken by Alexandre Ricord (date of col• • ETYMOLOGY.The species is named for Mark Catesby, noted lection unknown) (not examined by authors). North American naturalist. The subspecies names are all derived Uromacer catesbyi: Dumeril, Bibron, and Dumeril, 1854:72l. from Latin, as follow: cereolineatus, "waxen" and "thread," in allusion to the white longitudinal lateral line; hariolatus meaning • CONTENT.Eight subspecies are recognized, catesbyi, cereo• "predicted" in allusion to the fact that the north island (sensu lineatus,frondicolor, hariolatus, inchausteguii, insulaevaccarum, Williams, 1961) population was expected to be distinct; inchaus• pampineus, and scandax. teguii in honor of Sixto J. Inchaustegui, of the Museo Nacional de • DEFINITION.An elongate Uromacer, but head less elongate Historia Natural de Santo Domingo, Republica Dominicana; insu• than in congeners, and the head scales accordingly not highly mod• laevaccarum, a literal translation of lIe-a-Vache (island of cows), ified. Ventrals are 157-177 in males, and 155-179 in females; pampineus, "pertaining to vine tendrils or leaves;" and scandax, subcaudals are 172-208 in males, and 159-201 in females. -

Auto Guia Version Ingles
Parque Natural Metropolitano Tel: (507) 232-5516/5552 Fax: (507) 232-5615 www.parquemetropolitano.org Ave. Juan Pablo II final P.O. Box 0843-03129 Balboa, Ancón, Panamá República de Panamá 2 Taylor, L. 2006. Raintree Nutrition, Tropical Plant Database. http://www.rain- Welcome to the Metropolitan Natural Park, the lungs of Panama tree.com/plist.htm. Date accessed; February 2007 City! The park was established in 1985 and contains 232 hectares. It is one of the few protected areas located within the city border. Thomson, L., & Evans, B. 2006. Terminalia catappa (tropical almond), Species Profiles for Pacific Island Agroforestry. Permanent Agriculture Resources You are about to enter an ecosystem that is nearly extinct in Latin (PAR), Elevitch, C.R. (ed.). http://www.traditionaltreeorg . Date accessed March America: the Pacific dry forests. Whether your goals for this walk 2007-04-23 are a simple walk to keep you in shape or a careful look at the forest and its inhabitants, this guide will give you information about Young, A., Myers, P., Byrne, A. 1999, 2001, 2004. Bradypus variegatus, what can be commonly seen. We want to draw your attention Megalonychidae, Atta sexdens, Animal Diversity Web. http://animaldiversity.ummz.umich.edu/site/accounts/information/Bradypus_var toward little things that may at first glance seem hidden away. Our iegatus.html. Date accessed March 2007 hope is that it will raise your curiosity and that you’ll want to learn more about the mysteries that lie within the tropical forest. ACKNOWLEDGEMENTS The contents of this book include tree identifications, introductions Text and design: Elisabeth Naud and Rudi Markgraf, McGill University, to basic ecological concepts and special facts about animals you Montreal, Canada. -

Other Contributions
Other Contributions NATURE NOTES Amphibia: Caudata Ambystoma ordinarium. Predation by a Black-necked Gartersnake (Thamnophis cyrtopsis). The Michoacán Stream Salamander (Ambystoma ordinarium) is a facultatively paedomorphic ambystomatid species. Paedomorphic adults and larvae are found in montane streams, while metamorphic adults are terrestrial, remaining near natal streams (Ruiz-Martínez et al., 2014). Streams inhabited by this species are immersed in pine, pine-oak, and fir for- ests in the central part of the Trans-Mexican Volcanic Belt (Luna-Vega et al., 2007). All known localities where A. ordinarium has been recorded are situated between the vicinity of Lake Patzcuaro in the north-central portion of the state of Michoacan and Tianguistenco in the western part of the state of México (Ruiz-Martínez et al., 2014). This species is considered Endangered by the IUCN (IUCN, 2015), is protected by the government of Mexico, under the category Pr (special protection) (AmphibiaWeb; accessed 1April 2016), and Wilson et al. (2013) scored it at the upper end of the medium vulnerability level. Data available on the life history and biology of A. ordinarium is restricted to the species description (Taylor, 1940), distribution (Shaffer, 1984; Anderson and Worthington, 1971), diet composition (Alvarado-Díaz et al., 2002), phylogeny (Weisrock et al., 2006) and the effect of habitat quality on diet diversity (Ruiz-Martínez et al., 2014). We did not find predation records on this species in the literature, and in this note we present information on a predation attack on an adult neotenic A. ordinarium by a Thamnophis cyrtopsis. On 13 July 2010 at 1300 h, while conducting an ecological study of A. -

Herpetological Information Service No
Type Descriptions and Type Publications OF HoBART M. Smith, 1933 through June 1999 Ernest A. Liner Houma, Louisiana smithsonian herpetological information service no. 127 2000 SMITHSONIAN HERPETOLOGICAL INFORMATION SERVICE The SHIS series publishes and distributes translations, bibliographies, indices, and similar items judged useful to individuals interested in the biology of amphibians and reptiles, but unlikely to be published in the normal technical journals. Single copies are distributed free to interested individuals. Libraries, herpetological associations, and research laboratories are invited to exchange their publications with the Division of Amphibians and Reptiles. We wish to encourage individuals to share their bibliographies, translations, etc. with other herpetologists through the SHIS series. If you have such items please contact George Zug for instructions on preparation and submission. Contributors receive 50 free copies. Please address all requests for copies and inquiries to George Zug, Division of Amphibians and Reptiles, National Museum of Natural History, Smithsonian Institution, Washington DC 20560 USA. Please include a self-addressed mailing label with requests. Introduction Hobart M. Smith is one of herpetology's most prolific autiiors. As of 30 June 1999, he authored or co-authored 1367 publications covering a range of scholarly and popular papers dealing with such diverse subjects as taxonomy, life history, geographical distribution, checklists, nomenclatural problems, bibliographies, herpetological coins, anatomy, comparative anatomy textbooks, pet books, book reviews, abstracts, encyclopedia entries, prefaces and forwords as well as updating volumes being repnnted. The checklists of the herpetofauna of Mexico authored with Dr. Edward H. Taylor are legendary as is the Synopsis of the Herpetofalhva of Mexico coauthored with his late wife, Rozella B. -

Xenosaurus Tzacualtipantecus. the Zacualtipán Knob-Scaled Lizard Is Endemic to the Sierra Madre Oriental of Eastern Mexico
Xenosaurus tzacualtipantecus. The Zacualtipán knob-scaled lizard is endemic to the Sierra Madre Oriental of eastern Mexico. This medium-large lizard (female holotype measures 188 mm in total length) is known only from the vicinity of the type locality in eastern Hidalgo, at an elevation of 1,900 m in pine-oak forest, and a nearby locality at 2,000 m in northern Veracruz (Woolrich- Piña and Smith 2012). Xenosaurus tzacualtipantecus is thought to belong to the northern clade of the genus, which also contains X. newmanorum and X. platyceps (Bhullar 2011). As with its congeners, X. tzacualtipantecus is an inhabitant of crevices in limestone rocks. This species consumes beetles and lepidopteran larvae and gives birth to living young. The habitat of this lizard in the vicinity of the type locality is being deforested, and people in nearby towns have created an open garbage dump in this area. We determined its EVS as 17, in the middle of the high vulnerability category (see text for explanation), and its status by the IUCN and SEMAR- NAT presently are undetermined. This newly described endemic species is one of nine known species in the monogeneric family Xenosauridae, which is endemic to northern Mesoamerica (Mexico from Tamaulipas to Chiapas and into the montane portions of Alta Verapaz, Guatemala). All but one of these nine species is endemic to Mexico. Photo by Christian Berriozabal-Islas. amphibian-reptile-conservation.org 01 June 2013 | Volume 7 | Number 1 | e61 Copyright: © 2013 Wilson et al. This is an open-access article distributed under the terms of the Creative Com- mons Attribution–NonCommercial–NoDerivs 3.0 Unported License, which permits unrestricted use for non-com- Amphibian & Reptile Conservation 7(1): 1–47. -

Zootaxa, Molecular Phylogeny, Classification, and Biogeography Of
Zootaxa 2067: 1–28 (2009) ISSN 1175-5326 (print edition) www.mapress.com/zootaxa/ Article ZOOTAXA Copyright © 2009 · Magnolia Press ISSN 1175-5334 (online edition) Molecular phylogeny, classification, and biogeography of West Indian racer snakes of the Tribe Alsophiini (Squamata, Dipsadidae, Xenodontinae) S. BLAIR HEDGES1, ARNAUD COULOUX2, & NICOLAS VIDAL3,4 1Department of Biology, 208 Mueller Lab, Pennsylvania State University, University Park, PA 16802-5301 USA. E-mail: [email protected] 2Genoscope. Centre National de Séquençage, 2 rue Gaston Crémieux, CP5706, 91057 Evry Cedex, France www.genoscope.fr 3UMR 7138, Département Systématique et Evolution, Muséum National d’Histoire Naturelle, CP 26, 57 rue Cuvier, 75005 Paris, France 4Corresponding author. E-mail : [email protected] Abstract Most West Indian snakes of the family Dipsadidae belong to the Subfamily Xenodontinae and Tribe Alsophiini. As recognized here, alsophiine snakes are exclusively West Indian and comprise 43 species distributed throughout the region. These snakes are slender and typically fast-moving (active foraging), diurnal species often called racers. For the last four decades, their classification into six genera was based on a study utilizing hemipenial and external morphology and which concluded that their biogeographic history involved multiple colonizations from the mainland. Although subsequent studies have mostly disagreed with that phylogeny and taxonomy, no major changes in the classification have been proposed until now. Here we present a DNA sequence analysis of five mitochondrial genes and one nuclear gene in 35 species and subspecies of alsophiines. Our results are more consistent with geography than previous classifications based on morphology, and support a reclassification of the species of alsophiines into seven named and three new genera: Alsophis Fitzinger (Lesser Antilles), Arrhyton Günther (Cuba), Borikenophis Hedges & Vidal gen. -

Check List the Journal Of
12 1 1838 the journal of biodiversity data 6 February 2016 Check List NOTES ON GEOGRAPHIC DISTRIBUTION Check List 12(1): 1838, 6 February 2016 doi: http://dx.doi.org/10.15560/12.1.1838 ISSN 1809-127X © 2016 Check List and Authors Leptophis ahaetulla (Linnaeus, 1758) (Serpentes, Colubridae): first record for the state of Rio Grande do Sul, Brazil Roberto Baptista de Oliveira1*, Christian Beier2, Giancarlo Ribeiro Bilo3, Tiago Gomes dos Santos3 and Gláucia Maria Funk Pontes4 1 Fundação Zoobotânica do Rio Grande do Sul, Museu de Ciências Naturais, Seção de Zoologia de Vertebrados, Rua Dr. Salvador França 1427, CEP 90690-000, Porto Alegre, RS, Brazil 2 Pontifícia Universidade Católica do Rio Grande do Sul, Museu de Ciências e Tecnologia, Programa de Pós-Graduação em Zoologia, Laboratório de Ornitologia, Av. Ipiranga 6681, CEP 90619-900, Porto Alegre, RS, Brazil 3 Universidade Federal do Pampa, Laboratório de Estudos em Biodiversidade Pampiana (LEBIP), Av. Antônio Trilha 1847, CEP 97300- 000, São Gabriel, RS, Brazil 4 Pontifícia Universidade Católica do Rio Grande do Sul, Museu de Ciências e Tecnologia, Setor de Herpetologia, Av. Ipiranga 6681, CEP 90619-900, Porto Alegre, RS, Brazil * Corresponding author: E-mail: [email protected] Abstract: We present the first record of Leptophis the extreme North to the state of Paraná, occupying a ahaetulla for the State of Rio Grande do Sul, Brazil. wide range of biomes, including the Amazon, Pantanal, Between November and December 2014, and February Cerrado, Caatinga and Atlantic Forest (Cunha and 2015, three specimens were found, respectively: one male Nascimento 1978; Vanzolini et al. -

Biology and Impacts of Pacific Island Invasive Species. 8
University of Nebraska - Lincoln DigitalCommons@University of Nebraska - Lincoln USDA National Wildlife Research Center - Staff U.S. Department of Agriculture: Animal and Publications Plant Health Inspection Service 2012 Biology and Impacts of Pacific Island Invasive Species. 8. Eleutherodactylus planirostris, the Greenhouse Frog (Anura: Eleutherodactylidae) Christina A. Olson Utah State University, [email protected] Karen H. Beard Utah State University, [email protected] William C. Pitt National Wildlife Research Center, [email protected] Follow this and additional works at: https://digitalcommons.unl.edu/icwdm_usdanwrc Olson, Christina A.; Beard, Karen H.; and Pitt, William C., "Biology and Impacts of Pacific Island Invasive Species. 8. Eleutherodactylus planirostris, the Greenhouse Frog (Anura: Eleutherodactylidae)" (2012). USDA National Wildlife Research Center - Staff Publications. 1174. https://digitalcommons.unl.edu/icwdm_usdanwrc/1174 This Article is brought to you for free and open access by the U.S. Department of Agriculture: Animal and Plant Health Inspection Service at DigitalCommons@University of Nebraska - Lincoln. It has been accepted for inclusion in USDA National Wildlife Research Center - Staff Publications by an authorized administrator of DigitalCommons@University of Nebraska - Lincoln. Biology and Impacts of Pacific Island Invasive Species. 8. Eleutherodactylus planirostris, the Greenhouse Frog (Anura: Eleutherodactylidae)1 Christina A. Olson,2 Karen H. Beard,2,4 and William C. Pitt 3 Abstract: The greenhouse frog, Eleutherodactylus planirostris, is a direct- developing (i.e., no aquatic stage) frog native to Cuba and the Bahamas. It was introduced to Hawai‘i via nursery plants in the early 1990s and then subsequently from Hawai‘i to Guam in 2003. The greenhouse frog is now widespread on five Hawaiian Islands and Guam. -

Historia Natural Y Cultural De La Región Del Golfo Dulce, Costa Rica
Natural and Cultural History of the Golfo Dulce Region, Costa Rica Historia natural y cultural de la región del Golfo Dulce, Costa Rica Anton WEISSENHOFER , Werner HUBER , Veronika MAYER , Susanne PAMPERL , Anton WEBER , Gerhard AUBRECHT (scientific editors) Impressum Katalog / Publication: Stapfia 88 , Zugleich Kataloge der Oberösterreichischen Landesmuseen N.S. 80 ISSN: 0252-192X ISBN: 978-3-85474-195-4 Erscheinungsdatum / Date of deliVerY: 9. Oktober 2008 Medieninhaber und Herausgeber / CopYright: Land Oberösterreich, Oberösterreichische Landesmuseen, Museumstr.14, A-4020 LinZ Direktion: Mag. Dr. Peter Assmann Leitung BiologieZentrum: Dr. Gerhard Aubrecht Url: http://WWW.biologieZentrum.at E-Mail: [email protected] In Kooperation mit dem Verein Zur Förderung der Tropenstation La Gamba (WWW.lagamba.at). Wissenschaftliche Redaktion / Scientific editors: Anton Weissenhofer, Werner Huber, Veronika MaYer, Susanne Pamperl, Anton Weber, Gerhard Aubrecht Redaktionsassistent / Assistant editor: FritZ Gusenleitner LaYout, Druckorganisation / LaYout, printing organisation: EVa Rührnößl Druck / Printing: Plöchl-Druck, Werndlstraße 2, 4240 Freistadt, Austria Bestellung / Ordering: http://WWW.biologieZentrum.at/biophp/de/stapfia.php oder / or [email protected] Das Werk einschließlich aller seiner Teile ist urheberrechtlich geschütZt. Jede VerWertung außerhalb der en - gen GrenZen des UrheberrechtsgesetZes ist ohne Zustimmung des Medieninhabers unZulässig und strafbar. Das gilt insbesondere für VerVielfältigungen, ÜbersetZungen, MikroVerfilmungen soWie die Einspeicherung und Verarbeitung in elektronischen SYstemen. Für den Inhalt der Abhandlungen sind die Verfasser Verant - Wortlich. Schriftentausch erWünscht! All rights reserVed. No part of this publication maY be reproduced or transmitted in anY form or bY anY me - ans Without prior permission from the publisher. We are interested in an eXchange of publications. Umschlagfoto / CoVer: Blattschneiderameisen. Photo: AleXander Schneider. -

A Molecular Phylogeny of the Lamprophiidae Fitzinger (Serpentes, Caenophidia)
Zootaxa 1945: 51–66 (2008) ISSN 1175-5326 (print edition) www.mapress.com/zootaxa/ ZOOTAXA Copyright © 2008 · Magnolia Press ISSN 1175-5334 (online edition) Dissecting the major African snake radiation: a molecular phylogeny of the Lamprophiidae Fitzinger (Serpentes, Caenophidia) NICOLAS VIDAL1,10, WILLIAM R. BRANCH2, OLIVIER S.G. PAUWELS3,4, S. BLAIR HEDGES5, DONALD G. BROADLEY6, MICHAEL WINK7, CORINNE CRUAUD8, ULRICH JOGER9 & ZOLTÁN TAMÁS NAGY3 1UMR 7138, Systématique, Evolution, Adaptation, Département Systématique et Evolution, C. P. 26, Muséum National d’Histoire Naturelle, 43 Rue Cuvier, Paris 75005, France. E-mail: [email protected] 2Bayworld, P.O. Box 13147, Humewood 6013, South Africa. E-mail: [email protected] 3 Royal Belgian Institute of Natural Sciences, Rue Vautier 29, B-1000 Brussels, Belgium. E-mail: [email protected], [email protected] 4Smithsonian Institution, Center for Conservation Education and Sustainability, B.P. 48, Gamba, Gabon. 5Department of Biology, 208 Mueller Laboratory, Pennsylvania State University, University Park, PA 16802-5301 USA. E-mail: [email protected] 6Biodiversity Foundation for Africa, P.O. Box FM 730, Bulawayo, Zimbabwe. E-mail: [email protected] 7 Institute of Pharmacy and Molecular Biotechnology, University of Heidelberg, INF 364, D-69120 Heidelberg, Germany. E-mail: [email protected] 8Centre national de séquençage, Genoscope, 2 rue Gaston-Crémieux, CP5706, 91057 Evry cedex, France. E-mail: www.genoscope.fr 9Staatliches Naturhistorisches Museum, Pockelsstr. 10, 38106 Braunschweig, Germany. E-mail: [email protected] 10Corresponding author Abstract The Elapoidea includes the Elapidae and a large (~60 genera, 280 sp.) and mostly African (including Madagascar) radia- tion termed Lamprophiidae by Vidal et al. -

Clelia Plumbea Wied, 1820.Musurana Misionera O Gris
Cuad. herpetol. 26 (Supl. 1): 327-374 (2012) Categoría UICN plejos de cabañas, clubes recreativos, aumento de No evaluada pobladores en zonas ribereñas, extracción de leña, construcción de represas). Esta especie presenta Justificación otras características que la convierten en Vulnerable Esta especie había sido excluida de Argentina por como ser su especialización en alimentación (ofio- Zaher (1996), y varios taxones que incluyen princi- fagia), crecimiento lento y maduración tardía con palmente a Boiruna maculata, Clelia clelia y Clelia puestas relativamente pequeñas y largos períodos plumbea, habían sido confundidas frecuentemente entre puestas, además de su gran tamaño (Giraudo, en la literatura (Giraudo, 2001). Posteriormente 2001; Webb et al., 2002; Pizzatto, 2005). Scott et al., (2006) examinaron los géneros Boiru- na y Clelia en Argentina y Paraguay, incluyendo Sugerencias y acciones de conservación nuevamente a Clelia clelia en Argentina, mediante Su área de distribución posee pocas áreas protegidas material examinado del este de Formosa, Chaco, y estas están pobremente implementadas (Giraudo, Santa Fe y norte de Corrientes (posiblemente áreas 2001; Arzamendia y Giraudo, 2012). Se debería limítrofes de Misiones). Su distribución está asociada aumentar su superficie, representatividad e invertir a los grandes ríos Paraná y Paraguay (Arzamendia mayor cantidad de recursos humanos y materiales y Giraudo, 2009), donde habita principalmente en para mejorar la situación de las áreas protegidas bosques húmedos, que están siendo rápidamente existentes (por ejemplo: Sitios Ramsar Jaaukanigás y modificados en estas áreas por actividades humanas Chaco, Reserva de Biósfera Laguna Oca, Isla Apipé, (urbanización, construcción de viviendas, com- entre otras). Clelia plumbea Wied, 1820. Musurana misionera o gris Giraudo, A. -

New Records and Notes on Defensive Behavior of Thamnodynastes Rutilus (Prado 1942)
Neotropical Biology and Conservation 12(2):154-158, may-august 2017 Unisinos - doi: 10.4013/nbc.2017.122.09 SHORT COMMUNICATION New records and notes on defensive behavior of Thamnodynastes rutilus (Prado 1942) Novos registros e notas sobre comportamento defensivo de Thamnodynastes rutilus (Prado 1942) Jhonny José Magalhães Abstract Guedes1* [email protected] Snakes of the genus Thamnodynastes Wagler 1830 are viviparous, opisthoglyphous and have elliptical vertical pupil. Among all of the 11 species that occur in Brazil, T. rutilus is 1 Clodoaldo Lopes de Assis easily diagnosed by having a reddish spot in the sixth infralabial. Information about biolo- [email protected] gy, ecology, distribution and behavior of T. rutilus is very scarce in the literature. Such lack 1 of information leads to poor species management and difficulty for taking conservation Douglas Henrique da Silva measures when needed. Thus, this study brought new insights about T. rutilus geographi- [email protected] cal distribution, amplifying its previously known occurrence area, as well as providing new Renato Neves Feio1 data about the species natural defensive behavior. [email protected] Keywords: Squamata, Tachymenini tribe, snakes, conservation, Minas Gerais. Resumo Serpentes do gênero Thamnodynastes Wagler 1830 são vivíparas, opistóglifas e pos- suem pupila vertical elíptica. Dentre todas as 11 espécies que ocorrem no Brasil, T. ru- tilus é facilmente diagnosticada por possuir uma mancha vermelha na sexta infralabial. Informações sobre a biologia, ecologia, distribuição e comportamento dessa espécie são escassas na literatura. Tais lacunas podem acarretar em um manejo inadequado da es- pécie e em dificuldades na tomada de medidas conservacionistas, quando necessárias.