The Fallopian Canal: a Comprehensive Review and Proposal of a New Classification
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Temporal Bone Trauma Effects on Auditory Anatomical Structures in Mastoid Obliteration
European Archives of Oto-Rhino-Laryngology (2019) 276:513–520 https://doi.org/10.1007/s00405-018-5227-6 HEAD & NECK Temporal bone trauma effects on auditory anatomical structures in mastoid obliteration Aranka Ilea1 · Anca Butnaru2 · Silviu Andrei Sfrângeu2 · Mihaela Hedeșiu3 · Cristian Mircea Dudescu4 · Bianca Adina Boșca5 · Veronica Elena Trombitaș6 · Radu Septimiu Câmpian7 · Silviu Albu6 Received: 8 August 2018 / Accepted: 28 November 2018 / Published online: 3 December 2018 © Springer-Verlag GmbH Germany, part of Springer Nature 2018 Abstract Purpose The risk of temporal bone fractures in head trauma is not negligible, as injuries also depend on the resistance and integrity of head structures. The capacity of mastoid cells to absorb part of the impact kinetic energy of the temporal bone is diminished after open cavity mastoidectomy, even if the surgical procedure is followed by mastoid obliteration. The aim of our study was to evaluate the severity of lesions in auditory anatomical structures after a lateral impact on cadaveric tem- poral bones in which open cavity mastoidectomy followed by mastoid obliteration was performed, compared to cadaveric temporal bones with preserved mastoids. Methods The study was carried out on 20 cadaveric temporal bones, which were randomly assigned to two groups. In the study group, open cavity mastoidectomy followed by mastoid obliteration with heterologous materials was performed. All temporal bones were impacted laterally under the same conditions. Temporal bone fractures were evaluated by CT scan. Results External auditory canal fractures were six times more seen in the study group. Tympanic bone fractures were present in 80% of the samples in the study group and 10% in the control group (p = .005). -
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD
Imaging of Nontraumatic Temporal Bone Emergencies Nitesh Shekhrajka, MD and Gul Moonis, MD This section aims to cover the non-traumatic pathologies affecting the temporal bone including external auditory canal, middle ear and inner ear which usually need emergent clinical attention. Many of the conditions in this section are secondary to infections in differ- ent clinical settings with resultant complications which may leave temporary or permanent sequelae if not suspected, timely diagnosed or treated. Semin Ultrasound CT MRI 40:116-124 © 2018 Elsevier Inc. All rights reserved. External Auditory Canal There is abnormal soft tissue thickening and enhancement along the margins of the EAC, auricle, and periauricular soft Malignant Otitis Externa tissue. There is effacement of the fat planes around the stylo- his is a more aggressive form of acute otitis externa mastoid foramen and infratemporal fossa5. The involvement T which affects the elderly, diabetic, and immunocompro- of the stylomastoid foramen may result in facial nerve mised patients.1 The term “Malignant” is a misnomer used to involvement. Opacification of middle ear cavity and mastoid describe the aggressive clinical nature and high mortality in air cells are frequently seen (Fig. 1). this condition. It is also referred to as necrotizing otitis If the disease extends inferiorly to involve the subtemporal externa (NOE). In most cases, the causative pathogen is Pseu- soft tissues, parotid, masticator, and parapharyngeal spaces, domonas aeruginosa2 which is not normally found in the imaging will demonstrate abnormal soft tissue enhancement, external acoustic meatus (EAC) but Aspergillus fumigatus is diffuse enlargement of the surrounding muscles, parotid also implicated in immunocompromised patients.3 enlargement, and effacement of the fat planes with or with- The infection begins as an area of granulation at the junc- out abscess. -

Aberrant Hyperpneumatization from Mastoid Cells to Skull Cervicalarea
Acta Medica Mediterranea, 2007, 23: 43 ABERRANT HYPERPNEUMATIZATION FROM MASTOID CELLS TO SKULL CERVICALAREA AGOSTINO SERRA - CALOGERO GRILLO - RITA CHIARAMONTE - CATERINA GRILLO - LUIGI MAIOLINO Università degli Studi di Catania - Dipartimento di Specialità Medico Chirurgiche - Sezione di Otorinolaringoiatria (Direttore: A. Serra) [Iperpneumatizzazione aberrante delle celle mastoidee alla regione cranio-cervicale] SUMMARY RIASSUNTO Authors report the observation of a patient who has Gli autori riportano l’osservazione di un paziente sotto - u n d e rgone an encephalon’s C.A.T. examination for ingrave- posto ad esame TC encefalo per cefalea ingravescente e verti - scent headache and dizziness. gini. The C.A.T. examination of the skull highlighted a L’esame TC del cranio evidenziò una marcata pneuma - marked pneumatization of mastoid cell and temporal bone pre- tizzazione delle celle mastoidee e dell’osso temporale prevalen - valently on the right side, and also pneumatization of the right temente a destra, ed altresì pneumatizzazione della parte squa - pars squamosa ossis occipitalis that spreads also to the condilo mosa destra dell’osso occipitale che si estendeva anche al con - and the lateral atlantis mass. dilo ed alla massa laterale dell’atlante. Authors sustain that the abnormal pneumatization origi- Gli autori ritengono che l’abnorme pneumatizzazione nated from normal cellular bands, deriving from the primary originatasi dalle normali strie cellulari derivante dall’asse pneumatic axis, then probably spreaded with a valve mechani- pneumatico primario si siano poi estese mediante un possibile sm. meccanismo a valvola. Key words: Mastoid hyperpneumatization, dizziness, TC Parole chiave: Iperpneumatizzazione mastoidea, vertigine, TC Introduction We have also highlighted a bleb of enphysema inside the spino-canalis lateral to the dens axis. -

Entrapment Neuropathy of the Central Nervous System. Part II. Cranial
Entrapment neuropathy of the Cranial nerves central nervous system. Part II. Cranial nerves 1-IV, VI-VIII, XII HAROLD I. MAGOUN, D.O., F.A.A.O. Denver, Colorado This article, the second in a series, significance because of possible embarrassment considers specific examples of by adjacent structures in that area. The same entrapment neuropathy. It discusses entrapment can occur en route to their desti- nation. sources of malfunction of the olfactory nerves ranging from the The first cranial nerve relatively rare anosmia to the common The olfactory nerves (I) arise from the nasal chronic nasal drip. The frequency of mucosa and send about twenty central proces- ocular defects in the population today ses through the cribriform plate of the ethmoid bone to the inferior surface of the olfactory attests to the vulnerability of the optic bulb. They are concerned only with the sense nerves. Certain areas traversed by of smell. Many normal people have difficulty in each oculomotor nerve are pointed out identifying definite odors although they can as potential trouble spots. It is seen perceive them. This is not of real concern. The how the trochlear nerves are subject total loss of smell, or anosmia, is the significant to tension, pressure, or stress from abnormality. It may be due to a considerable variety of causes from arteriosclerosis to tu- trauma to various bony components morous growths but there is another cause of the skull. Finally, structural which is not usually considered. influences on the abducens, facial, The cribriform plate fits within the ethmoid acoustic, and hypoglossal nerves notch between the orbital plates of the frontal are explored. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

Clinical Importance of the Middle Meningeal Artery
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Jagiellonian Univeristy Repository FOLIA MEDICA CRACOVIENSIA 41 Vol. LIII, 1, 2013: 41–46 PL ISSN 0015-5616 Przemysław Chmielewski1, Janusz skrzat1, Jerzy waloCha1 CLINICAL IMPORTANCE OF THE MIDDLE MENINGEAL ARTERY Abstract: Middle meningeal artery (MMA)is an important branch which supplies among others cranial dura mater. It directly attaches to the cranial bones (is incorporated into periosteal layer of dura mater), favors common injuries in course of head trauma. This review describes available data on the MMA considering its varability, or treats specific diseases or injuries where the course of MMA may have clinical impact. Key words: Middle meningeal artery (MMA), aneurysm of the middle meningeal artery, epidural he- matoma, anatomical variation of MMA. TOPOGRAPHY OF THE MIDDLE MENINGEAL ARTERY AND ITS BRANCHES Middle meningeal artery (MMA) [1] is most commonly the strongest branch of maxillary artery (from external carotid artery) [2]. It supplies blood to cranial dura mater, and through the numerous perforating branches it nourishes also periosteum of the inner aspect of cranial bones. It enters the middle cranial fossa through the foramen spinosum, and courses between the dura mater and the inner aspect of the vault of the skull. Next it divides into two terminal branches — frontal (anterior) which supplies blood to bones forming anterior cranial fossa and the anterior part of the middle cranial fossa; parietal branch (posterior), which runs more horizontally toward the back and supplies posterior part of the middle cranial fossa and supratentorial part of the posterior cranial fossa. -
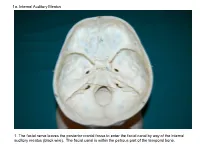
1A. Internal Auditory Meatus
1a. Internal Auditory Meatus 1. The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). The facial canal is within the petrous part of the temporal bone. 1b. Internal Auditory Meatus The facial nerve leaves the posterior cranial fossa to enter the facial canal by way of the internal auditory meatus (black wire). 2. Hiatus of the Canal and Groove for the Greater Superficial Petrosal Nerve The greater superficial petrosal nerve leaves the facial canal to enter the middle cranial fossa by way of the hiatus of the canal for the greater superficial petrosal nerve (black wire). 3. Pterygoid Canal at Anterior Lip of the Lacerate Foramen The greater superficial petrosal nerve is joined by the deep petrosal nerve to form the nerve of the pterygoid canal (black and red wire). This nerve leaves the middle cranial fossa to enter the pterygopalatine fossa by way of the pterygoid canal. The posterior opening of the pterygoid canal is at the anterior lip of the lacerate foramen. The greater superficial nerve and the deep petrosal nerve travel within the cavernous sinus. 4. Pterygopalatine Fossa Seen Through the Pterygomaxillary Fissure The anterior opening of the pterygoid canal is into the pterygopalatine fossa (black wire). The pterygopalatine fossa is located medial to the pterygomaxillary fissure and contains the pterygopalatine ganglion. 5. External Auditory Meatus The chorda tympani nerve leaves the facial canal and crosses the middle ear (black wire). It then leaves the middle ear to arrive in the infratemporal fossa by way of the petrotympanic fissure. -

Research Reports
ARAŞTIRMALAR (ResearchUnur, Ülger, Reports) Ekinci MORPHOMETRICAL AND MORPHOLOGICAL VARIATIONS OF MIDDLE EAR OSSICLES IN THE NEWBORN* Yeni doğanlarda orta kulak kemikciklerinin morfometrik ve morfolojik varyasyonları Erdoğan UNUR 1, Harun ÜLGER 1, Nihat EKİNCİ 2 Abstract Özet Purpose: Aim of this study was to investigate the Amaç: Yeni doğanlarda orta kulak kemikciklerinin morphometric and morphologic variations of middle ear morfometrik ve morfolojik varyasyonlarını ortaya ossicles. koymak. Materials and Methods: Middle ear of 20 newborn Gereç ve yöntem: Her iki cinse ait 20 yeni doğan cadavers from both sexes were dissected bilaterally and kadavrasının orta kulak boşluğuna girilerek elde edilen the ossicles were obtained to investigate their orta kulak kemikcikleri üzerinde morfometrik ve morphometric and morphologic characteristics. morfolojik inceleme yapıldı. Results: The average of morphometric parameters Bulgular: Morfometrik sonuçlar; malleus’un toplam showed that the malleus was 7.69 mm in total length with uzunluğu 7.69 mm, manibrium mallei’nin uzunluğu 4.70 an angle of 137 o; the manibrium mallei was 4.70 mm, mm, caput mallei ve processus lateralis arasındaki and the total length of head and neck was 4.85 mm; the uzaklık 4.85 mm, manibrium mallei’nin ekseni ve caput incus had a total length of 6.47 mm, total width of 4.88 mallei arasındaki açı 137 o, incus’un toplam uzunluğu mm , and a maximal distance of 6.12 mm between the 6.47 mm, toplam genişliği 4.88 mm, crus longum ve tops of the processes, with an angle of 99.9 o; the stapes breve’nin uçları arasındaki uzaklık 6.12 mm, cruslar had a total height of 3.22 mm, with stapedial base being arasındaki açı 99.9 o, stapesin toplam uzunluğu 2.57 mm in length and 1.29 mm in width. -

MBB: Head & Neck Anatomy
MBB: Head & Neck Anatomy Skull Osteology • This is a comprehensive guide of all the skull features you must know by the practical exam. • Many of these structures will be presented multiple times during upcoming labs. • This PowerPoint Handout is the resource you will use during lab when you have access to skulls. Mind, Brain & Behavior 2021 Osteology of the Skull Slide Title Slide Number Slide Title Slide Number Ethmoid Slide 3 Paranasal Sinuses Slide 19 Vomer, Nasal Bone, and Inferior Turbinate (Concha) Slide4 Paranasal Sinus Imaging Slide 20 Lacrimal and Palatine Bones Slide 5 Paranasal Sinus Imaging (Sagittal Section) Slide 21 Zygomatic Bone Slide 6 Skull Sutures Slide 22 Frontal Bone Slide 7 Foramen RevieW Slide 23 Mandible Slide 8 Skull Subdivisions Slide 24 Maxilla Slide 9 Sphenoid Bone Slide 10 Skull Subdivisions: Viscerocranium Slide 25 Temporal Bone Slide 11 Skull Subdivisions: Neurocranium Slide 26 Temporal Bone (Continued) Slide 12 Cranial Base: Cranial Fossae Slide 27 Temporal Bone (Middle Ear Cavity and Facial Canal) Slide 13 Skull Development: Intramembranous vs Endochondral Slide 28 Occipital Bone Slide 14 Ossification Structures/Spaces Formed by More Than One Bone Slide 15 Intramembranous Ossification: Fontanelles Slide 29 Structures/Apertures Formed by More Than One Bone Slide 16 Intramembranous Ossification: Craniosynostosis Slide 30 Nasal Septum Slide 17 Endochondral Ossification Slide 31 Infratemporal Fossa & Pterygopalatine Fossa Slide 18 Achondroplasia and Skull Growth Slide 32 Ethmoid • Cribriform plate/foramina -

Surgical Management of Posterior Petrous Meningiomas
Neurosurg Focus 14 (6):Article 7, 2003, Click here to return to Table of Contents Surgical management of posterior petrous meningiomas JAMES K. LIU, M.D., OREN N. GOTTFRIED, M.D., AND WILLIAM T. COULDWELL, M.D., PH.D. Department of Neurosurgery, University of Utah School of Medicine, Salt Lake City, Utah Posterior petrous meningiomas (commonly termed posterior pyramid meningiomas and/or meningiomas of the pos- terior surface of the petrous pyramid) are the most common meningiomas of the posterior cranial fossa. They are locat- ed along the posterior surface of the temporal bone in the region of the cerebellopontine angle. They often mimic vestibular schwannomas, both clinically and on neuroimaging studies. Common clinical symptoms include hearing loss, cerebellar ataxia, and trigeminal neuropathy. The site of dural origin determines the direction of cranial nerve dis- placement. Total resection can be achieved in most cases with a low morbidity rate and an excellent prognosis. The authors review the surgical management of posterior petrous meningiomas. KEY WORDS • meningioma • cerebellopontine angle • skull base surgery • petrous bone Posterior fossa meningiomas comprise approximately In their series Samii and Ammirati18 used the term “pos- 10% of all intracranial meningiomas.8 Castellano and terior pyramid meningiomas” and defined them as tumors Ruggiero4 reviewed Olivecrona’s experience with treat- whose main direction of growth brings them in contact ing posterior fossa meningiomas and classified them with the posterior pyramid, irrespective of their site of based on the site of dural attachment. They described the dural attachment. They also designated those located ante- location as cerebellar convexity (10%), tentorium (30%), rior and those posterior to the internal acoustic meatus. -

Morphometric Analysis of Stylomastoid Foramen Location and Its Clinical Importance
Dental Communication Biosc.Biotech.Res.Comm. Special Issue Vol 13 No 8 2020 Pp-108-111 Morphometric Analysis of Stylomastoid Foramen Location and its Clinical Importance Hemanth Ragav N V1 and Yuvaraj Babu K2* 1Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai- 600077, India 2Assistant Professor, Department of Anatomy, Saveetha Dental College and Hospitals, Saveetha Institute of Medical and Technical Science, Saveetha University, Chennai- 600077, India ABSTRACT The stylomastoid foramen is located between the styloid process and mastoid process of the temporal bone. Facial nerve and Stylomastoid branch of posterior auricular artery passes through this stylomastoid foramen. The facial nerve can be blocked at this stylomastoid foramen but it has high risk of nerve damage. For Nadbath facial nerve block, stylomastoid foramen is the most important site. Facial canal ends at this foramen and it is the important motor portion of this stylomastoid foramen. A total of 50 dry skulls from the Anatomy Department of Saveetha Dental College were studied to locate the position of the centre of the stylomastoid foramen with respect to the tip of mastoid process and the articular tubercle of the zygomatic arch by a digital vernier caliper. All measurements were tabulated and statistically analysed. In our study, we found the mean distance of stylomastoid foramen from mastoid processes 16.31+2.37 mm and 16.01+2.08 mm on right and left. Their range is 10.48-23.34 mm and 11.5-21.7 mm. The mean distance of stylomastoid foramen from articular tubercle is 29.48+1.91 mm and 29.90+1.62 mm on right and left. -

The Braincase of Two Late Cretaceous Asian Multituberculates Studied by Serial Sections
The braincase of two Late Cretaceous Asian multituberculates studied by serial sections J0RN H. HURUM Hurum, J.H. 1998. The braincase of two Late Cretaceous Asian multituberculatesstudied by serial sections. -Acta Palaeontologica Polonica 43, 1, 21-52. The braincase structure of two Late Cretaceous Mongolian djadochtatherian multituber- culates Nemegtbaatar gobiensis and Chulsanbaatar vulgaris from the ?late Campanian of Mongolia is presented based on the two serially sectioned skulls and additional specimens. Reconstructions of the floor of the braincase in both taxa are given. The complete intracranial sphenoid region is reconstructed for the first time in multitubercu- lates. Cavum epiptericum is a separate space with the taenia clino-orbitalis (ossified pila antotica) as the medial wall, anterior lamina of the petrosal and possibly the alisphenoid as the lateral wall, and the basisphenoid, petrosal and possibly alisphenoid ventrally. The fovea hypochiasmatica is shallow, tuberculurn sellae is wide and more raised from the skull base than it is in the genus Pseudobolodon. The dorsal opening of the carotid canal is situated in the fossa hypophyseos. The taenia clino-orbitalis differs from the one described in Pseudobolodon and Lambdopsalis in possessing just one foramen (metoptic foramen). Compared to all extant mammals the braincase in Nemegtbaatar and Chulsan- baatar is primitive in that both the pila antotica and pila metoptica are retained. In both genera the anterior lamina of the petrosal is large with a long anterodorsal process while the alisphenoid is small. A review is given of the cranial anatomy in Nemegtbaatar and Chulsanbaatar. K e y w o r d s : Braincase structure, sphenoid complex, cavum epiptericum,Mammalia, Multituberculata,Djadochtatheria, Cretaceous, Mongolia.