The Great Forgotten in Rheumatoid Arthritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ubiquitin-Mediated Control of ETS Transcription Factors: Roles in Cancer and Development
International Journal of Molecular Sciences Review Ubiquitin-Mediated Control of ETS Transcription Factors: Roles in Cancer and Development Charles Ducker * and Peter E. Shaw * Queen’s Medical Centre, School of Life Sciences, University of Nottingham, Nottingham NG7 2UH, UK * Correspondence: [email protected] (C.D.); [email protected] (P.E.S.) Abstract: Genome expansion, whole genome and gene duplication events during metazoan evolution produced an extensive family of ETS genes whose members express transcription factors with a conserved winged helix-turn-helix DNA-binding domain. Unravelling their biological roles has proved challenging with functional redundancy manifest in overlapping expression patterns, a common consensus DNA-binding motif and responsiveness to mitogen-activated protein kinase signalling. Key determinants of the cellular repertoire of ETS proteins are their stability and turnover, controlled largely by the actions of selective E3 ubiquitin ligases and deubiquitinases. Here we discuss the known relationships between ETS proteins and enzymes that determine their ubiquitin status, their integration with other developmental signal transduction pathways and how suppression of ETS protein ubiquitination contributes to the malignant cell phenotype in multiple cancers. Keywords: E3 ligase complex; deubiquitinase; gene fusions; mitogens; phosphorylation; DNA damage 1. Introduction Citation: Ducker, C.; Shaw, P.E. Cell growth, proliferation and differentiation are complex, concerted processes that Ubiquitin-Mediated Control of ETS Transcription Factors: Roles in Cancer rely on careful regulation of gene expression. Control over gene expression is maintained and Development. Int. J. Mol. Sci. through signalling pathways that respond to external cellular stimuli, such as growth 2021, 22, 5119. https://doi.org/ factors, cytokines and chemokines, that invoke expression profiles commensurate with 10.3390/ijms22105119 diverse cellular outcomes. -

Confirmation of Pathogenic Mechanisms by SARS-Cov-2–Host
Messina et al. Cell Death and Disease (2021) 12:788 https://doi.org/10.1038/s41419-021-03881-8 Cell Death & Disease ARTICLE Open Access Looking for pathways related to COVID-19: confirmation of pathogenic mechanisms by SARS-CoV-2–host interactome Francesco Messina 1, Emanuela Giombini1, Chiara Montaldo1, Ashish Arunkumar Sharma2, Antonio Zoccoli3, Rafick-Pierre Sekaly2, Franco Locatelli4, Alimuddin Zumla5, Markus Maeurer6,7, Maria R. Capobianchi1, Francesco Nicola Lauria1 and Giuseppe Ippolito 1 Abstract In the last months, many studies have clearly described several mechanisms of SARS-CoV-2 infection at cell and tissue level, but the mechanisms of interaction between host and SARS-CoV-2, determining the grade of COVID-19 severity, are still unknown. We provide a network analysis on protein–protein interactions (PPI) between viral and host proteins to better identify host biological responses, induced by both whole proteome of SARS-CoV-2 and specific viral proteins. A host-virus interactome was inferred, applying an explorative algorithm (Random Walk with Restart, RWR) triggered by 28 proteins of SARS-CoV-2. The analysis of PPI allowed to estimate the distribution of SARS-CoV-2 proteins in the host cell. Interactome built around one single viral protein allowed to define a different response, underlining as ORF8 and ORF3a modulated cardiovascular diseases and pro-inflammatory pathways, respectively. Finally, the network-based approach highlighted a possible direct action of ORF3a and NS7b to enhancing Bradykinin Storm. This network-based representation of SARS-CoV-2 infection could be a framework for pathogenic evaluation of specific 1234567890():,; 1234567890():,; 1234567890():,; 1234567890():,; clinical outcomes. -

ETV7 293T Cell Transient Overexpression Lysate(Denatured)
Produktinformation Diagnostik & molekulare Diagnostik Laborgeräte & Service Zellkultur & Verbrauchsmaterial Forschungsprodukte & Biochemikalien Weitere Information auf den folgenden Seiten! See the following pages for more information! Lieferung & Zahlungsart Lieferung: frei Haus Bestellung auf Rechnung SZABO-SCANDIC Lieferung: € 10,- HandelsgmbH & Co KG Erstbestellung Vorauskassa Quellenstraße 110, A-1100 Wien T. +43(0)1 489 3961-0 Zuschläge F. +43(0)1 489 3961-7 [email protected] • Mindermengenzuschlag www.szabo-scandic.com • Trockeneiszuschlag • Gefahrgutzuschlag linkedin.com/company/szaboscandic • Expressversand facebook.com/szaboscandic ETV7 293T Cell Transient Overexpression Lysate(Denatured) Catalog # : H00051513-T01 規格 : [ 100 uL ] List All Specification Application Image Transfected 293T Western Blot Cell Line: Plasmid: pCMV-ETV7 full-length Host: Human Theoretical MW 39 (kDa): Quality Control Transient overexpression cell lysate was tested with Anti-ETV7 antibody Testing: (H00051513-B01) by Western Blots. SDS-PAGE Gel ETV7 transfected lysate. Western Blot Lane 1: ETV7 transfected lysate ( 39 KDa) Lane 2: Non-transfected lysate. Storage Buffer: 1X Sample Buffer (50 mM Tris-HCl, 2% SDS, 10% glycerol, 300 mM 2- mercaptoethanol, 0.01% Bromophenol blue) Storage Store at -80°C. Aliquot to avoid repeated freezing and thawing. Instruction: MSDS: Download Applications Page 1 of 2 2016/5/23 Western Blot Gene Information Entrez GeneID: 51513 GeneBank NM_016135.2 Accession#: Protein - Accession#: Gene Name: ETV7 Gene Alias: TEL-2,TEL2,TELB -

Alteration of Gene Expression in Response to Bone Morphogenetic Protein-2 in Androgen-Dependent Human Prostate Cancer Lncap Cells
KUMAGAI 26_8 30/12/05 14:22 Page 285 INTERNATIONAL JOURNAL OF MOLECULAR MEDICINE 17: 285-291, 2006 285 Alteration of gene expression in response to bone morphogenetic protein-2 in androgen-dependent human prostate cancer LNCaP cells TORU KUMAGAI, KENTARO TOMARI, TAKAHISA SHIMIZU and KEN TAKEDA Department of Hygiene-Chemistry, Faculty of Pharmaceutical Sciences, Tokyo University of Science, 2641 Yamazaki Noda-shi, Chiba 278-8510, Japan Received August 26, 2005; Accepted October 14, 2005 Abstract. Bone morphogenetic protein (BMP)-2, a multi- ectopic bone formation in vivo (3,4). In addition to functions functional member of the transforming growth factor (TGF)-ß as a possible bone-inducing factor, BMPs have been shown superfamily with powerful osteoinductive effects, has various to play important roles in various biological processes such biological activities in a variety of cells. We observed that as chemotaxis of monocytes (5), migration of osteoblasts BMP-2 inhibits cell proliferation in the androgen-dependent (6) and differentiation of neural cells (7). BMPs and their human prostate cancer cell line, LNCaP. To investigate the receptors are widely distributed not only in bone and cartilage mechanism of inhibition of androgen-dependent growth by but also in other tissue. BMP receptor (BMPR) mRNA is BMP-2, we compared the gene expression in LNCaP cells expressed at higher levels in the prostate than in other organs treated with dihydrotestosterone (DHT) to that of LNCaP (8), and the expression of BMPRs (9) and BMP-2 (10) cells treated with DHT and BMP-2, using DNA microarray decreases with the progression of prostate cancer. -

ETV7 Regulates Breast Cancer Stem-Like Cell Plasticity by Repressing IFN- Response Genes
bioRxiv preprint doi: https://doi.org/10.1101/2020.09.02.279133; this version posted September 3, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 ETV7 regulates breast cancer stem-like cell plasticity by repressing IFN- 2 response genes 3 4 5 6 7 Laura Pezzè1,#, Mattia Forcato2, Stefano Pontalti1,^, Kalina Aleksandra Badowska1,#, Dario 8 Rizzotto3,°, Ira-Ida Skvortsova4,5, Silvio Bicciato2, Yari Ciribilli1,§ 9 10 11 12 1 Laboratory of Molecular Cancer Research, Department of Cellular, Computational and Integrative 13 Biology (CIBIO), University of Trento, Italy; 2 Department of Life Sciences, University of Modena 14 and Reggio Emilia, Italy; 3 Laboratory of Transcriptional Networks, Department CIBIO, University 15 of Trento, Italy; 4 EXTRO-Lab, Department of Therapeutic Radiology and Oncology, Medical 16 University of Innsbruck, Austria; 5 Tyrolean Cancer Research Institute, Innsbruck, Austria 17 # present address: Alia Therapeutics s.r.l., Trento, Italy 18 ^ present address: Azienda Provinciale per i Servizi Sanitari, APSS, Trento, Italy 19 °present address: CeMM Research Center for Molecular Medicine of the Austrian Academy of 20 Sciences, Vienna, Austria 21 § correspondence: [email protected] (YC) 22 23 24 25 Running Title: ETV7 regulates BCSCs plasticity 26 27 28 Keywords: ETV7 – Cancer stem cells – Breast cancer – Interferon – Chemoresistance 29 30 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.09.02.279133; this version posted September 3, 2020. -
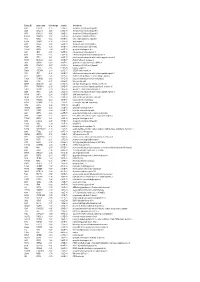
Entrez ID Gene Name Fold Change Q-Value Description
Entrez ID gene name fold change q-value description 4283 CXCL9 -7.25 5.28E-05 chemokine (C-X-C motif) ligand 9 3627 CXCL10 -6.88 6.58E-05 chemokine (C-X-C motif) ligand 10 6373 CXCL11 -5.65 3.69E-04 chemokine (C-X-C motif) ligand 11 405753 DUOXA2 -3.97 3.05E-06 dual oxidase maturation factor 2 4843 NOS2 -3.62 5.43E-03 nitric oxide synthase 2, inducible 50506 DUOX2 -3.24 5.01E-06 dual oxidase 2 6355 CCL8 -3.07 3.67E-03 chemokine (C-C motif) ligand 8 10964 IFI44L -3.06 4.43E-04 interferon-induced protein 44-like 115362 GBP5 -2.94 6.83E-04 guanylate binding protein 5 3620 IDO1 -2.91 5.65E-06 indoleamine 2,3-dioxygenase 1 8519 IFITM1 -2.67 5.65E-06 interferon induced transmembrane protein 1 3433 IFIT2 -2.61 2.28E-03 interferon-induced protein with tetratricopeptide repeats 2 54898 ELOVL2 -2.61 4.38E-07 ELOVL fatty acid elongase 2 2892 GRIA3 -2.60 3.06E-05 glutamate receptor, ionotropic, AMPA 3 6376 CX3CL1 -2.57 4.43E-04 chemokine (C-X3-C motif) ligand 1 7098 TLR3 -2.55 5.76E-06 toll-like receptor 3 79689 STEAP4 -2.50 8.35E-05 STEAP family member 4 3434 IFIT1 -2.48 2.64E-03 interferon-induced protein with tetratricopeptide repeats 1 4321 MMP12 -2.45 2.30E-04 matrix metallopeptidase 12 (macrophage elastase) 10826 FAXDC2 -2.42 5.01E-06 fatty acid hydroxylase domain containing 2 8626 TP63 -2.41 2.02E-05 tumor protein p63 64577 ALDH8A1 -2.41 6.05E-06 aldehyde dehydrogenase 8 family, member A1 8740 TNFSF14 -2.40 6.35E-05 tumor necrosis factor (ligand) superfamily, member 14 10417 SPON2 -2.39 2.46E-06 spondin 2, extracellular matrix protein 3437 -

(12) United States Patent (10) Patent No.: US 8,148,129 B2 Frankel Et Al
US008148129B2 (12) United States Patent (10) Patent No.: US 8,148,129 B2 Frankel et al. (45) Date of Patent: Apr. 3, 2012 (54) GENERATION OF POTENT DOMINANT 6,824,978 B1 1 1/2004 Cox, III et al. NEGATIVE TRANSCRIPTIONAL 6,933,113 B2 8, 2005 Case et al. 6,979,539 B2 12/2005 Cox, III et al. INHIBITORS 7,013,219 B2 3/2006 Case et al. 7,070,934 B2 7/2006 Cox, III et al. (75) Inventors: Alan Frankel, Mill Valley, CA (US); 7,163,824 B2 1/2007 Cox, III et al. Robert Nakamura, San Francisco, CA 7,220,719 B2 5/2007 Case et al. (US); Chandreyee Das, Brookline, MA 7,235,354 B2 6/2007 Case et al. 7,262,054 B2 8/2007 Jamieson et al. (US); Ivan D’Orso, San Francisco, CA 7,273,923 B2 9/2007 Jamieson et al. (US); Jocelyn Grunwell, San Mateo, 2003, OO82552 A1* 5, 2003 Wolffe et al. ..................... 435/6 CA (US) (73) Assignee: The Regents of the University of OTHER PUBLICATIONS California, Oakland, CA (US) Cramer et al., Coupling of Transcription with Alternative Splicing: RNA Pol II Promoters Modulate SF2. ASF and 9G8 Effects on an (*) Notice: Subject to any disclaimer, the term of this Exonic Splicing Enhancer, Molecular Cell, 1999, 4:251-258.* patent is extended or adjusted under 35 Cama-Carvalho et al., Nucleocytoplasmic shuttling of heterodimeric U.S.C. 154(b) by 806 days. splicing factor U2AF, JBC. Published on Dec. 15, 2000 as Manu script M008759200.* (21) Appl. No.: 11/765,592 Rosonina et al., Gene Expression: The Close Coupling of Transcrip tion and Splicing, Current Biology, vol. -

Table S1. 103 Ferroptosis-Related Genes Retrieved from the Genecards
Table S1. 103 ferroptosis-related genes retrieved from the GeneCards. Gene Symbol Description Category GPX4 Glutathione Peroxidase 4 Protein Coding AIFM2 Apoptosis Inducing Factor Mitochondria Associated 2 Protein Coding TP53 Tumor Protein P53 Protein Coding ACSL4 Acyl-CoA Synthetase Long Chain Family Member 4 Protein Coding SLC7A11 Solute Carrier Family 7 Member 11 Protein Coding VDAC2 Voltage Dependent Anion Channel 2 Protein Coding VDAC3 Voltage Dependent Anion Channel 3 Protein Coding ATG5 Autophagy Related 5 Protein Coding ATG7 Autophagy Related 7 Protein Coding NCOA4 Nuclear Receptor Coactivator 4 Protein Coding HMOX1 Heme Oxygenase 1 Protein Coding SLC3A2 Solute Carrier Family 3 Member 2 Protein Coding ALOX15 Arachidonate 15-Lipoxygenase Protein Coding BECN1 Beclin 1 Protein Coding PRKAA1 Protein Kinase AMP-Activated Catalytic Subunit Alpha 1 Protein Coding SAT1 Spermidine/Spermine N1-Acetyltransferase 1 Protein Coding NF2 Neurofibromin 2 Protein Coding YAP1 Yes1 Associated Transcriptional Regulator Protein Coding FTH1 Ferritin Heavy Chain 1 Protein Coding TF Transferrin Protein Coding TFRC Transferrin Receptor Protein Coding FTL Ferritin Light Chain Protein Coding CYBB Cytochrome B-245 Beta Chain Protein Coding GSS Glutathione Synthetase Protein Coding CP Ceruloplasmin Protein Coding PRNP Prion Protein Protein Coding SLC11A2 Solute Carrier Family 11 Member 2 Protein Coding SLC40A1 Solute Carrier Family 40 Member 1 Protein Coding STEAP3 STEAP3 Metalloreductase Protein Coding ACSL1 Acyl-CoA Synthetase Long Chain Family Member 1 Protein -

Genomic Gain at 6P21: a New Cryptic Molecular Rearrangement in Secondary Myelodysplastic Syndrome and Acute Myeloid Leukemia
Leukemia (2006) 20, 958–964 & 2006 Nature Publishing Group All rights reserved 0887-6924/06 $30.00 www.nature.com/leu ORIGINAL ARTICLE Genomic gain at 6p21: a new cryptic molecular rearrangement in secondary myelodysplastic syndrome and acute myeloid leukemia R La Starza1, A Aventin2, C Matteucci1, B Crescenzi1, S Romoli1, N Testoni3, V Pierini1, S Ciolli4, C Sambani5, A Locasciulli6, E Di Bona7, M Lafage-Pochitaloff8, MF Martelli1, P Marynen9 and C Mecucci1 1Hematology and Bone Marrow Transplantation Unit, University of Perugia, Perugia, Italy; 2Servei de Hematologia, Hospital De La Santa Creu I Sant Pau, Barcelona, Spain; 3‘Istituto Seragnoli’, Hospital S Orsola, Bologna, Italy; 4Hematology Unit, University of Firenze, Firenze, Italy; 5Laboratory of Health Physics and Environmental Hygiene, NCSR ‘Demokritos’, Athens, Greece; 6Hematology, Hospital ‘S Camillo’ of Rome, Rome, Italy; 7Hematology, Hospital ‘S Bortolo’ Vicenza, Vicenza, Italy; 8Laboratoire de Biopathologie, Institut Paoli-Calmettes, INSERM U119, Marseille, France and 9Center for Human Genetics and Flanders Interuniversity Institute for Biotechnology (VIB), University of Leuven, Campus Gasthuisberg, Leuven, Belgium Fluorescence in situ hybridization and comparative genomic ter aberrantly activates the cyclin D3, which is overexpressed;5,6 hybridization characterized 6p rearrangements in eight primary in MM with t(6;14)(p25;q32), the IgH gene juxtaposes to MUM/ and in 10 secondary myeloid disorders (including one patient IRF4.7 with Fanconi anemia) and found different molecular lesions in In secondary myelodysplastic syndrome (MDS) and AML, 6p each group. In primary disorders, 6p abnormalities, isolated in six patients, were highly heterogeneous with different break- rearrangements account for less than 2% of cytogenetic 8 points along the 6p arm. -
BGGN 213 Pathway Analysis and the Interpretation of Gene Lists
BGGN 213 Pathway Analysis and the Interpretation of Gene Lists Barry Grant http://thegrantlab.org/bggn213 My high-throughput experiment generated a long list of genes/proteins… What do I do now? Pathway analysis! (a.k.a. geneset enrichment) Use bioinformatics methods to help extract biological meaning from such lists… Pathway analysis (a.k.a. geneset enrichment) Principle DEGs Pathway Differentially Pathway Expressed (geneset) Genes (DEGs) Enriched Not enriched • Variations of the math: overlap, ranking, networks... ➢ Not critical, different algorithms show similar performances • DEGs come from your experiment ➢ Critical, needs to be as clean as possible • Pathway genes (“geneset”) come from annotations ➢ Important, but typically not a competitive advantage Pathway analysis (a.k.a. geneset enrichment) Limitations • Post-transcriptional regulation is neglected • Directionality is hard to capture sensibly • e.g. IκBα/NF-κB • Tissue-specific variations of pathways are not annotated • e.g. NF-κB regulates metabolism, not inflammation, in adipocytes • Size bias: stats are influenced by the size of the pathway • Geneset annotation bias: can only discover what is already known • Non-model organisms: no high-quality genesets available • Many pathways/receptors converge to few regulators • e.g. tens of innate immune receptors activate 4 TFs: NF-kB, AP-1, IRF3/7, NFAT Starting point for pathway analysis: Your gene list • You have a list of genes/proteins of interest • You have quantitative data for each gene/protein • Fold change 228018_at F26A1.8NP_000192 -
NOTCH1 Signaling in Oral Squamous Cell Carcinoma Via a TEL2/ SERPINE1 Axis
www.oncotarget.com Oncotarget, 2019, Vol. 10, (No. 63), pp: 6791-6804 Research Paper NOTCH1 signaling in oral squamous cell carcinoma via a TEL2/ SERPINE1 axis Vasiliki Salameti1,*, Priyanka G. Bhosale1,*, Ashley Ames-Draycott1, Kalle Sipilä1 and Fiona M. Watt1 1Centre for Stem Cells and Regenerative Medicine, King's College London, Tower Wing, Guy's Hospital, London, UK *These authors contributed equally to this work Correspondence to: Fiona M. Watt, email: [email protected] Keywords: oral squamous cell carcinoma (OSCC); NOTCH1; SERPINE1; ETV7/TEL2; cell adhesion Received: April 29, 2019 Accepted: October 21, 2019 Published: November 26, 2019 Copyright: Salameti et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License 3.0 (CC BY 3.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. ABSTRACT Inactivating mutations in the EGF-like ligand binding domain of NOTCH1 are a prominent feature of the mutational landscape of oral squamous cell carcinoma (OSCC). In this study, we investigated NOTCH1 mutations in keratinocyte lines derived from OSCC biopsies that had been subjected to whole exome sequencing. One line, SJG6, was found to have truncating mutations in both NOTCH1 alleles, resulting in loss of NOTCH1 expression. Overexpression of the NOTCH1 intracellular domain (NICD) in SJG6 cells promoted cell adhesion and differentiation, while suppressing proliferation, migration and clonal growth, consistent with the previously reported tumour suppressive function of NOTCH1 in OSCC. Comparative gene expression profiling identified SERPINE1 as being downregulated on NICD overexpression and predicted an interaction between SERPINE1 and genes involved in cell proliferation and migration. -
![BIMM 143 Reads R1 Reads R2 Control Pathway Analysis and the [Optional] Fastqc Fastq Fastq Interpretation of Gene Lists Treatment 2](https://docslib.b-cdn.net/cover/3702/bimm-143-reads-r1-reads-r2-control-pathway-analysis-and-the-optional-fastqc-fastq-fastq-interpretation-of-gene-lists-treatment-2-7473702.webp)
BIMM 143 Reads R1 Reads R2 Control Pathway Analysis and the [Optional] Fastqc Fastq Fastq Interpretation of Gene Lists Treatment 2
Inputs Steps Reads R1 Reads R2 [optional] Control FastQ FastQ 1. Quality BIMM 143 Reads R1 Reads R2 Control Pathway Analysis and the [optional] FastQC FastQ FastQ Interpretation of Gene Lists Treatment 2. Reference Lecture 15 Alignment Genome (Mapping) UCSC Fasta TopHat2 Barry Grant Count Last day’s step Table 4. 3. data.frame Annotation Read Differential http://thegrantlab.org/bimm143 Counting expression UCSC GTF Count analysis! CuffLinks Table DESeq2 data.frame Volcano Plot Fold change vs P-value Significant (P < 0.01 & log2 > 2) My high-throughput experiment generated a Pathway analysis! long list of genes/proteins… (a.k.a. geneset enrichment) What do I do now? Use bioinformatics methods to help extract biological meaning from such lists… Inputs Steps Basic idea Reads R1 Reads R2 [optional] Control FastQ FastQ 1. Differentially Expressed Genes (DEGs) Gene-sets (Pathways, Quality annotations, etc...) Reads R1 Reads R2 Control [optional] FastQC 5. Gene set Annotate... FastQ FastQ enrichment Treatment analysis 2. nalysis! Reference KEGG, GO, … Alignment Genome (Mapping) UCSC Fasta TopHat2 Count Table 4. 3. data.frame Annotation Read Differential Counting expression UCSC GTF Count analysis! CuffLinks Table DESeq2 data.frame Basic idea Pathway analysis (a.k.a. geneset enrichment) Principle Differentially Expressed Genes (DEGs) Gene-sets (Pathways, annotations, etc...) Annotate... DEGs Pathway Differentially Pathway Expressed (geneset) Genes (DEGs) Enriched Not enriched Differentially Pathways • DEGs come from your experiment ➢ Critical, needs to be as clean as possible Expressed Overlap... • Pathway genes (“geneset”) come from annotations ➢ Important, but typically not a competitive advantage Genes • Variations of the math: overlap, ranking, networks... ➢ Not critical, different algorithms show similar performances (DEGs) Pathway analysis (geneset enrichment) Side-note: Pathway analysis (a.k.a.