Frequency of Myelin Oligodendrocyte Glycoprotein Antibody in Multiple Sclerosis a Multicenter Cross-Sectional Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
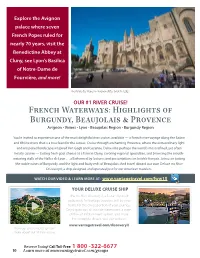
French Waterways: Highlights of Burgundy, Beaujolais & Provence
Explore the Avignon palace where seven French Popes ruled for nearly 70 years, visit the Benedictine Abbey at Cluny, see Lyon’s Basilica of Notre-Dame de Fourvière, and more! The Palais des Popes in Avignon dates back to 1252. OUR #1 RIVER CRUISE! French Waterways: Highlights of Burgundy, Beaujolais & Provence Avignon • Viviers • Lyon • Beaujolais Region • Burgundy Region You’re invited to experience one of the most delightful river cruises available — a French river voyage along the Saône and Rhône rivers that is a true feast for the senses. Cruise through enchanting Provence, where the extraordinary light and unspoiled landscapes inspired Van Gogh and Cezanne. Delve into perhaps the world’s most refined, yet often hearty cuisine — tasting fresh goat cheese at a farm in Cluny, savoring regional specialties, and browsing the mouth- watering stalls of the Halles de Lyon . all informed by lectures and presentations on la table français. Join us in tasting the noble wines of Burgundy, and the light and fruity reds of Beaujolais. And travel aboard our own Deluxe ms River Discovery II, a ship designed and operated just for our American travelers. WATCH OUR VIDEO & LEARN MORE AT: www.vantagetravel.com/fww15 Additional Online Content YOUR DELUXE CRUISE SHIP Facebook The ms River Discovery II, a 5-star ship built exclusively for Vantage travelers, will be your home for the cruise portion of your journey. Enjoy spacious, all outside staterooms, a state- of-the-art infotainment system, and more. For complete details, visit our website. www.vantagetravel.com/discoveryII View our online video to learn more about our #1 river cruise. -
Status Report
Status Report Gran Sasso detector Emulsion Scanning Sensitivity to oscillations September 2001 Installation and Schedule P. Strolin Conclusions Focus is on new developments Belgium IIHE(ULB-VUB) Brussels China IHEP Beijing, Shandong CERN COLLABORATION Croatia Zagreb 34 groups France ~ 160 physicists LAPP Annecy, IPNL Lyon, LAL Orsay, IRES Strasbourg Groups having joined Germany after the Proposal are Berlin, Hagen, Hamburg, Münster, Rostock underlined Israel Technion Haifa Italy Bari, Bologna, LNF Frascati, LNGS, Naples, Padova, Rome, Salerno Japan Aichi, Toho, Kobe, Nagoya, Utsunomiya Russia INR Moscow, ITEP Moscow, JINR Dubna Switzerland Bern, Neuchâtel Turkey METU Ankara To identify τ leptons, “see” their decays at the mm scale τ decay “kink” τ mm τ .6 ~ 0 ντ The challenge ν oscillation → massive target AND τ decay → micron resolution Lead – nuclear emulsion sandwich “Emulsion Cloud Chamber” The detector at Gran Sasso (modular structure, three “supermodules”) µ spectrometer superm odule Magnetised Iron Dipoles Drift tubes and RPCs brick (56 Pb/Em. “cells”) ν m 10 ~ 8 cm (10X ) module 0 ν target and τ decay detector Each “supermodule” is brick wall a sequence of 24 “modules” consisting of scintillator strips - a “wall” of Pb/emulsion “bricks” 235,000 - two planes of orthogonal scintillator strips bricks Status of the experiment Since the Proposal • Full scale prototypes to finalise the detector design • Progress in automatic scanning • Studies of detection efficiency and backgrounds • Sensitivity estimates updated with Super-K results • Organisation structure for detector construction Now: a “phase transition” from studies and tests to construction with related major investments of financial and human resources Gran Sasso Detector Preparation for production of emulsion films ! Ten small batch productions and one large production of emulsion films by Fuji Co. -

In Love with Lyon, France and Everything French
jadorelyon In Love with Lyon, France and Everything French Lyon, September 2017 By Aga Marchewka yOUR gUIDE TO LYON WWW.JADORELYON.COM jadorelyon By Aga Marchewka I am a Polish Girl who felt in love with Lyon from the first sight! So I moved here to discover ABOUT AGA AT France…starting from Lyon I want to learn more about France and everything what’s French. I love all JADORELYON those culture’s differences and I love to explore more. I like to share my observations through my IN LOVE WITH LYON, FRANCE AND EVERYTHING blog and photos which I love to take. So that’s why FRENCH jadorelyon was born. Because I truly love Lyon & France & Everything what is French. jadorelyon is my WWW.JADORELYON.COM way of exploring France, the French way of life, food, places to visit, things to do & adding Polish influence to it! jadorelyon By Aga Marchewka fIND ME : JOin Me here & Discover More About Lyon, France & Everything French FB JadoreLyon By Aga JadoreLyon Instagram Google Plus J'adorelyon Tumblr ShopaholicAga Pinterest JadoreLyon Twitter Aga at LinkedIn jadorelyon By Aga Marchewka Summary: 1. LOCATION- Lyon is 2. BASIC NUMBERS ABOUT LYON 3. MAIN FACTS ABOUT LYON AND LYONNAIS 4. PUBLIC TRANSPORT IN LYON 5. LEISURE ACTIVITIES - Top 10 Things To Do In Lyon 6. TOP 5 TRIPS AROUND LYON 7. TOP 5 MUSEUMS AROUND LYON 8. TOP 5 EVENTS IN LYON 9. MY FAVORITE EXPATS WEBSITES AND COMMUNITIES 10. TOP 5 BLOGS ABOUT LYON 11. TOP 5 ONLINE MAGAZINES ABOUT LYON AND FRANCE IN ENGLISH 12. -

Senator's Pre-Tour from Sunday 5Th May to Wednesday 8Th May, 2019
JCI Senator's Pre-Tour From Sunday 5th May to Wednesday 8th May, 2019 It is a tradition to propose a pre-tour to the Senators to discover the region of the European Conference site. This year, we propose to discover the south part of the region, called "Drôme-Provençale". It's located 100 kilometres south from Lyon in the Rhône Valley and it's the beginning of the Provence. The pre-tour starts from Lyon city centre on Sunday 5th May 2019 morning and it finishes in Lyon, just in front of the conference site on Wednesday 8th May (end of morning). The price we propose is "All inclusive": – 3 nights and breakfast (Su, Mo, Tu), it means you don't have to pack and unpack your luggage every day. – All lunches and dinners from Sunday to Tuesday. – Transport from Sunday morning to Wednesday morning in a comfortable coach. – Visits and guides. – And… surprises! The Senators and the members of Jeune Chambre Economique de Valence will be very happy to welcome you for a unique experience! JCI Senators of Auvergne Rhône-Alpes SENATOR'S PRE-TOUR Discover Drôme From the cliffs of the Vercors to the plains of Provence, from the sun-drenched vineyards to the upland villages, Drôme is both shadow and light, spacious yet intimate. From one end to the other, Drôme is a mosaic of scenery with breath-taking panoramas, perfumed with the fragrances of the South. 2 SENATOR'S PRE-TOUR Valence, our base-camp Situated astride the greatest European North-South route, Valence-sur-Rhône, the main city of Drôme, is a staging post par excellence and also an attractive place for a longer stay. -

Colors of Provence Cruising the Rhône with Amawaterways
October 21–31, 2019 Colors of Provence Cruising the Rhône with AmaWaterways Join Mary Gaffney-Ward and fellow Madison Club members on a magical French culinary and wine adventure. Our cruise begins in Arles, Provence, a city of Roman treasures, in one of the world’s great wine regions. We travel the Rhône River in luxury aboard the AmaCello for on our journey to the French culinary capital, the UNESCO Heritage city of Lyon. A journey of French wine & culinary delights From romantic cities to foodie havens and artistic epicenters, our itinerary features will enliven the senses. We’ll trace the steps of Van Gogh in Arles, discover the Carriéres de Lumiéres, savor the beauty of legendary vineyards and enjoy local vintages Beaujolais and Côtes du Rhône. We’ll go in search of the highly prized “Black $3497* Madison Club member price Diamond” truffles, learn to pair chocolate with wines and per participant double occupancy stateroom discover how olives became the Mediterranean’s nector, olive oil. We’ll cap our adventure in France’s culinary PUBLISHED PRICE $4798 capital, Lyon. *Pre-cruise, port charges & airfare additional *Early bird pricing--must book before Feburary 20 2019 Your $700 deposit per person secures one of our fourteen staterooms. KARL GUTKNECHT | 608/345.6557 [email protected] Colors of Provence The Rhône River Besides providing captivating views of medieval towns and colorful landscapes, the Rhône River connects the dots between thousands of vineyards from Lyon to Avignon. Our Colors of Provence itinerary takes you through this prized wine-producing region in southeastern France, known across the globe as the Rhône Valley. -

Insa: Engineering Professionals
#Landscape Design #ResearchLaboratories #PhD #Engineering #Architecture #Landscape Design #ResearchLaboratories #PhD #Engineering #Architecture #Landscape Design #ResearchLaboratories #PhD #Engineering #Architecture #Landscape Design #PhD #Engineering #Architecture #Landscape Design #ResearchLaboratories #PhD #Engineering #Landscape Design #PhD #Engi- National Institute of neering #Architecture Science and Technology #Lands- More than 40 specializations covering almost every field of science and technology #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #PhD #Architecture #PhD #Architecturee #Landscape Design #ResearchLaboratories #Engineering #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture #PhD #Engineering #Landscape Design #ResearchLaboratories #Architecture -

Paris in the Spring, Burgundy & Provence
Exclusive Charter NBSAC presents Paris in the Spring, Burgundy & Provence River Cruise featuring 2 Nights in Paris & 7 nights aboard the Amadeus Provence 11 Days April 13 - April 23, 2020 Booking Discount - Save $200 per couple! Daily Itinerary Cities & Ports Paris in the Spring, Burgundy & Provence River Cruise Paris Enjoy a panoramic Paris City Tour, the “City of Light,” to see the beloved land- 11 Days April 13 - 23, 2020 Ship - Amadeus Provence marks of Paris that line the Seine including the grand Notre Dame Cathedral and the palatial façade of the Louvre. The river’s historic banks are a UNESCO World Day 1 Depart US - Overnight Flight Heritage Site. Enjoy an afternoon of leisure time to admire the masterpieces of Day 2 Arrive Paris the Louvre or ascend the Eiffel Tower for fantastic views. Meet your PWD Tour/Cruise Manager - Transfer to your hotel for 2-Night Stay Dijon Welcome Drink at the hotel Overnight - Paris Enroute from Paris to your ship, stop for a Dijon Walking Tour. Best known for its Day 3 Paris mustard, Dijon is also one of the most beautiful cities in France with a wonder- Morning Paris City Tour ful historical center registered as a UNESCO World Heritage site. Dijon mustard Afternoon at leisure or Optional Excursion to Versailles originated in 1856, when Jean Naigeon substituted, the acidic juice of not-ripe Meal - B Overnight - Paris grapes, for vinegar in the traditional mustard recipe. Day 4 Paris - Dijon - Lyon Lyon Travel to Dijon via motorcoach and enjoy a Dijon Walking Tour Lyon, a city in France’s historical Rhône-Alpes region, sits at the junction of the Continue to Lyon and board the MS Amadeus Provence for 7 nights Rhône & Saône Rivers with a history dating back to ancient Roman times. -

Study Abroad Manual for Lyon, France
Study Abroad Manual for Lyon, France Lyon, France is located in south-east France in the Rhône-Alps region. (Département: Rhône(69)) It is the country’s second largest city with a metropolitan population just under 2 million people. Table of Contents: . Things to do in Lyon . Preparing to Study Abroad in Lyon . Studying at the Univeristy . CIEF Language Program . International Office in Lyon . Banking in France . Housing . Transportation around Lyon . Health Insurance . Cell Phones . CAF . Travelling . Where to Stay while travelling Take some time to Things to do in Lyon get to know the city before you arrive in Lyon! Tourist Office: The tourist office is located in Place Bellecour. You can pick up maps and ask them what there is to do around the city. VISIT: http://www.en.lyon-france.com/ Also Visit: http://www.petit-bulletin.fr/lyon/index.html Some starter ideas: . Basilique Notre-Dame de Fourvière . Tête d’Or Park (There is a zoo with free admission) . Vieux Lyon (the old part of Lyon) . Place Bellecour (City Center) . La Confluence (Neighborhood and Shopping Center) . Musée des Beaux Arts . Musée d’art contemporain de Lyon . La Croix Rousse (Vintage Shops!) . Food Markets are held in Vieux Lyon and Quai Saint Antoine throughout the week! Visit this Website: http://lyon- eats.blogspot.com/2009/02/lyon- markets.html . Indoor Ice Skating Rink by the Confluence . Go to a Soccer Game http://www.olweb.fr/en/ . Eat at a Bouchon (Traditional Lyonnais Food) http://www.en.lyon-france.com/Restaurants/Lyonnais-Bouchon-Traditional- Restaurant/?page=2 . Fête des Lumières: http://euronews.com/2012/12/07/light-artists-commemorate-the- saving-of-lyon/ . -
University Lyon 1 Degree Programs Taught in English
FRANCE UNIVERSITY LYON 1 Sciences - Technology Health Sciences DEGREE PROGRAMS TAUGHT IN ENGLISH Office of International Affairs / April 2014 WELCOME TO LYON 1! 3 WELCOME TO LYON 1! BACHELOR’S DEGREE 4 The Claude Bernard University Lyon 1 is a multidisciplinary institution that is involved in basic research BACHELOR’S PROGRAMS IN GEOSCIENCES 4 and its applications. Lyon 1 offers more than 300 degree-granting programs in Health, Sciences,Technology. MASTER’S DEGREE IN LIFE SCIENCES 5 Almost 80% of students are enrolled on courses leading to professional qualifications. MASTER’S PROGRAM IN GENETICS, CELL BIOLOGY, PATHOLOGIES 5 It currently has 69 research laboratories whose work focuses in particular on the areas of Health, MASTER’S PROGRAM IN BIOSCIENCES 6 Environment and Material Sciences. MASTER’S PROGRAM IN NEUROSCIENCES RESEARCH 2nd Year 8 KEY FIGURES OF LYON 1 MASTER’S DEGREE IN CHEMISTRY 9 • 40 000 students MASTER’S PROGRAM IN SYNTHESIS, CATALYSIS AND SUSTAINABLE CHEMISTRY 9 • 10,5 % of foreign students of 134 nationalities • 4700 employees MASTER’S DEGREE IN ENGINEERING 11 • A budget of 388,5 million euros MASTER’S PROGRAM IN MECHANICAL ENGINEERING 1st Year 11 MASTER’S PROGRAM IN MECHANICAL ENGINEERING 2nd Year 11 • 69 research units • More than 4 500 international publications per year MASTER’S DEGREE IN EARTH SCIENCES 12 • 40 patent applications per year MASTER’S PROGRAM IN EARTH SCIENCES 1 s t Year 12 MASTER’S PROGRAM IN EARTH SCIENCES 2 n d Year 12 MASTER’S DEGREE IN NANOSCALE ENGINEERING 13 MASTER’S DEGREE PROGRAM IN NANOSCALE -

Naviguer Sur Le Rhône Navigating the Rhône Schiffart Auf Der Rhône 2 INFOS / PASSAGE DES ÉCLUSES / LE RHÔNE De Lyon À La Mer Sommaire
LE RHÔNE DE LYON À LA MER THE RHÔNE FROM LYON TO THE SEA DIE RHÔNE ZWISCHEN LYON UND MEER L’énergie au cœur des territoires 2 rue André Bonin INFOS 69316 LYON CEDEX 04 - FRANCE Tél. : +33 (0) 472 00 69 69 NAVIGUER cnr.tm.fr SUR LE RHÔNE NavigaTING THE RHÔNE SCHIFFART auF DER RHÔNE Graphistar | Juin 2015 Crédits photos CNR Camille Moirenc illustrations : Geronimo CONTACTS ECLUSES Lock contact numbers Schleusen Écluse vhf Tél. n Pierre Bénite 19 +33 (0)4 78 70 99 89 n Vaugris 22 +33 (0)4 74 53 45 72 n Sablons 20 +33 (0)4 75 31 04 49 n Gervans 19 +33 (0)4 75 03 35 75 n Bourg-lès-Valence 22 +33 (0)4 75 83 81 35 n Beauchastel 20 +33 (0)4 75 85 17 94 n Logis Neuf 19 +33 (0)4 75 90 06 24 n Châteauneuf 22 +33 (0)4 75 90 70 33 n Bollène 20 +33 (0)4 90 30 52 94 n Caderousse 19 +33 (0)4 90 34 20 70 n Villeneuve-lès-Avignon 22 +33 (0)4 90 86 80 69 n Vallabrègues Beaucaire 20 +33 (0)4 66 59 58 43 n Barcarin 22 +33 (0)4 42 86 23 72 Passage interdit à la plaisance No entry for leisure boat / Durchfahrt verboten fürFreizeitboote n Port-Saint-Louis du Rhône 19 +33 (0)4 42 86 02 04 INFORHONE 0 820 10 10 20*/ www.inforhone.fr* * serveur vocal interactif facturé 0.12 euro TTC/min depuis un poste fixe * interactive information line (within France only), Euro 0.12/min (inc. -

Le Château De La Rochepot : De La Forteresse Gothique Au Château Néo-Gothique
Le château de La Rochepot : de la forteresse gothique au château néo-gothique LAURENT SACCARO* *Le château de La Rochepot, situé ménager l’exactitude historique et à 15 km au sud-ouest de Beaune, est l’habitabilité des lieux. Cet intérêt en une figure emblématique de la soi du château restauré avait déjà été Bourgogne. Ses toits de tuiles pressenti par Françoise Bercé, qui vernissées font depuis un siècle le voyait en La Rochepot une « savante bonheur des guides et des albums reconstruction [...] Mais peut-être touristiques, qui répètent à l’envie s’agit-il là moins d’une création néo- comment le fils du président de la gothique que d’une restitution archéo- République Sadi Carnot, au début du logique réussie... »3. XXe siècle, a reconstruit à grands frais Le château mérite donc les ruines du château bâti par la famille aujourd’hui d’être étudié d’une part Pot au XVe siècle. Cette restauration a comme bâtiment médiéval, dont les souvent été décriée par de nombreux vestiges sont très visibles et bien auteurs comme un sommet de identifiables en sous-œuvre, d’autre l’architecture troubadour, qui aurait part comme édifice néo-gothique, fait table rase des vestiges médiévaux : puisqu’il s’agit d’un édifice tout à fait de ce point de vue, le Guide du exemplaire pour ce type d’architecture Routard1 et des auteurs scientifiques en Bourgogne. comme Jean Mesqui2 sont au diapason! Pourtant, une étude plus précise Le château, du Moyen Âge à la des archives de Sadi Carnot d’une part, Révolution et des vestiges d’autre part, montrent que Charles Suisse, l’architecte de la Un premier château reconstruction, a rebâti le château à partir de travaux archéologiques tout à Sur le haut de la colline du fait sérieux, et avec le double souci de Châtelot, qui porte le château actuel (fig. -

Metabolites OH
H OH metabolites OH Article Metabolomics of Small Intestine Neuroendocrine Tumors and Related Hepatic Metastases Alessio Imperiale 1,2,3,4,*, Gilles Poncet 5 , Pietro Addeo 6, Elisa Ruhland 1,3, Colette Roche 7, Stephanie Battini 3 , A. Ercument Cicek 8, Marie Pierrette Chenard 2,9, Valérie Hervieu 7,10, Bernard Goichot 2,11, Philippe Bachellier 2,6, Thomas Walter 12,13 and Izzie Jacques Namer 1,2,3 1 Biophysics and Nuclear Medicine, University Hospitals of Strasbourg, 67098 Strasbourg, France; [email protected] (E.R.); [email protected] (I.J.N.) 2 Faculty of Medicine, University of Strasbourg, FMTS, 67000 Strasbourg, France; [email protected] (M.P.C.); [email protected] (B.G.); [email protected] (P.B.) 3 MNMS Platform, University Hospitals of Strasbourg, 67098 Strasbourg, France; [email protected] 4 Molecular Imaging—Institut Pluridisciplinaire Hubert Curien (IPHC), UMR 7178 – CNRS/Unistra, 67098 Strasbourg, France 5 Digestive and Oncologic Surgery, Edouard-Herriot University Hospital, Claude-Bernard Lyon 1 University, 69622 Lyon, France; [email protected] 6 Hepato-Pancreato-Biliary Surgery and Liver transplantation, University Hospitals of Strasbourg, University of Strasbourg, 67098 Strasbourg, France; [email protected] 7 INSERM U1052/CNRS UMR5286/University of Lyon, Cancer Research Center of Lyon, 69622 Lyon, France; [email protected] (C.R.); [email protected] (V.H.) 8 Computer Engineering