Annual Report and Accounts 1 April 2019 to 31 March 2020
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

KKL UK Financial Declaration 2018
UK Template COMPANY NAME: YEAR: COUNTRY: DATE OF SUBMISSION TO CENTRAL PLATFORM: [insert date] METHODOLOGICAL NOTE (H) (Clause 24.10): [insert link here] DISCLOSURE OF PAYMENTS TO HEALTHCARE PROFESSIONALS (HCPs), OTHER RELEVANT DECISION MAKERS (ORDMs) AND HEALTHCARE ORGANISATIONS (HCOs) Article 2 - Section 2.03 & Schedule 2 & Clause 24 Date of publication: 28 June 2018 HCPs/ORDMs: City of Country of Principal Unique country local Fee for service and consultancy (Art. 3.01.1.c & 3.01.2.c & Clause Full Name Principal Practice HCOs: Principal Practice Address Contribution to costs of Events (Art. 3.01.1.b & 3.01.2.a & Clause 24) Blank Column (Clause X) Practice identifyer OPTIONAL 24) city where registered Donations and Grants to HCOs (Art. 3.01.1.a & Joint Working (Clause 20) TOTAL Clause 24) and Benefits in Kind to HCOs (Clause 24) Sponsorship agreements with Related expenses agreed in HCOs / third parties Blank Column Blank Column (Clause (Art. 1.01 & Clause 24) (Art. 3 & Clause 24) (Schedule 1 & Clause 24) (Art. 3 & Clause 24) (Art. 3 & Clause 24) Registration Fees Travel & Accommodation Fees the fee for service or appointed by HCOs to (Clause X) X) manage an Event consultancy contract HCPs/ORDMs: City of Principal Local Register ID or Title First Name Initial Last Name Speciality Role Practice HCOs: city where Country of Principal Practice Institution Name Location Address Line 1 Address Line 2 Post Code Email Third Party Database registered ID INDIVIDUAL NAMED DISCLOSURE - one line per HCP/ORDM (i.e. all transfers of value during a -

Northern Deanery Foundation School (NDFS) SOUTH TEES
Northern Deanery Foundation School (NDFS) SOUTH TEES HOSPITALS NHS Foundation Trust Individual Placement Description Placement FY1 –Acute Medicine, Friarage Hospital The department The F1 doctor who does Acute Medicine as part of their programme will work spend 4 months attached to a team of doctors in one specific clinical specialty with the opportunity to spend two sessions a week in other learning environments such as out-patients. The type of work to expect All F1 Doctors in hospital posts will generally and learning opportunities be ward based during the ‘normal’ working day and expected to deliver the daily medical care of all the patients on their ward irrespective of specialty. Whilst in the Acute Medicine attachment the F1 will be involved with the generic clerking of patients being admitted and the ongoing care of the patients in the unit. The overall educational objectives of the F1 year are to provide the trainee with the knowledge, skills and attitudes to be able to Take a history and examine a patient Identify and synthesise problems Prescribe safely Keep an accurate and relevant medical record Manage time and clinical priorities effectively Communicate effectively with patients, relatives and colleagues Use evidence, guidelines and audit to benefit patient care Act in a professional manner at all times Cope with ethical and legal issues which occur during the management of patients with general medical problems Educate patients effectively Become life-long learners and teachers. Where the placement is Friarage Hospital, Northallerton based Clinical Supervisor(s) for the Dr Nick Quinn placement Main duties of the placement The F1 doctor is responsible with other staff for the ward care of patients and the maintenance of the patient’s medical record. -

Summer 2019 Magazine for Staff, Members, Volunteers and People Who Use Our Services
Summer 2019 Magazine for staff, members, volunteers and people who use our services 100% Renewable Energy for ELFT Award Success We car We r s ect We ar i clus ve TRUSTtalk IMPROVED EXPERIENCE OF CARE Chief Executive FOREWORD THE Trust has hosted a flurry of events comfort of our offices at HQ. reminded us all to take time to listen and and conferences that has set me in I was joined by 12 colleagues from understand complexities and events in a spin! But to me, these are a good different staff groups who not only the lives of others. (See page 8) sign because it means that people are listened in and watched the conference, This issue of Trusttalk has a special talking - they are listening, they are but contributed key points from our table feature on Mental Health Research and curious, open to new ideas, articulating discussion. (Page 10) Development which is a massive part of their own theories and understanding, Our Quality Conference took place on our work here in ELFT. We underestimate happy to be challenged and happy to be 13 May and brought together staff from how much research undertaken in the with peers talking about their work. It is all corners of the Trust. I felt so proud Trust contributes to treatment, care, sociable and it is stimulating - exactly hearing of the often simple projects management and approaches across the what an NHS trust like ELFT should that make a massive difference to world. I am very proud of our research be all about. -

Choosing Your Hospital
Choosing your hospital Redcar and Cleveland Primary Care Trust For most medical conditions, you can now choose where and when to have your treatment. This booklet explains more about choosing your hospital. You will also find information about the hospitals you can choose from. Second edition December 2006 Contents What is patient choice? 1 Making your choice 2 How to use this booklet 3 Where can I have my treatment? 4 Your hospitals A to Z 7 Your questions answered 32 How to book your appointment 34 What do the specialty names mean? 35 What does the healthcare jargon mean? 37 Where can I find more information and support? 39 How do your hospitals score? 40 Hospital score table 44 What is patient choice? If you and your GP decide that you need to see a specialist for more treatment, you can now choose where and when to have your treatment from a list of hospitals or clinics. Why has patient choice been introduced? Research has shown that patients want to be more involved in making decisions and choosing their healthcare. Most of the patients who are offered a choice of hospital consider the experience to be positive and valuable. The NHS is changing to give you more choice and flexibility in how you are treated. Your choices Your local choices are included in this booklet. If you do not want to receive your treatment at a local hospital, your GP will be able to tell you about your choices of other hospitals across England. As well as the hospitals listed in this booklet, your GP may be able to suggest community-based services, such as GPs with Special Interests or community clinics. -

May 2015 Update on the New Sexual Health Service
Stakeholder Briefing – May 2015 Update on the new sexual health service for North Yorkshire and York York Teaching Hospital NHS Foundation Trust has been commissioned by North Yorkshire County Council and City of York Council to deliver a new integrated sexual health service across North Yorkshire and York. The new service will commence on the 1st July and the service will be provided under the recognised name YorSexualHealth. Benefits of the new service will include improved access to services and better training and support to professionals. One advantage of the new service will be the introduction of ‘One stop shop’ clinics providing contraception, STI tests and treatments for all ages. This means that in most cases people will be able to have all their sexual health needs met by one practitioner without the need for onward referral. We are working in partnership with GP Alliances to maximise access and choice for people. We are also working with North Yorkshire AIDS Action to provide Services for People Living with HIV and with Yorkshire MESMAC to provide Community Outreach Services as part of the new integrated service. Improved access to services will be achieved through: • YorSexualHealth Centres in Northallerton, Harrogate, Scarborough, Selby and York • New community clinics across all district council areas • Targeted 'Satellite' clinics (including those targeted towards young people) • Provision for military personnel • Delivery of services in healthcare settings (including GP surgeries) • The use of “virtual” clinics including -
Improving Data Sharing Between Acute Hospitals in England
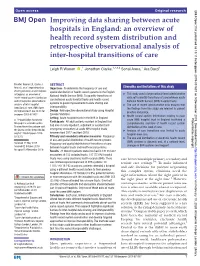
Open access Original research BMJ Open: first published as 10.1136/bmjopen-2019-031637 on 5 December 2019. Downloaded from Improving data sharing between acute hospitals in England: an overview of health record system distribution and retrospective observational analysis of inter- hospital transitions of care Leigh R Warren ,1 Jonathan Clarke,1,2,3,4 Sonal Arora,1 Ara Darzi1 To cite: Warren LR, Clarke J, ABSTRACT Strengths and limitations of this study Arora S, et al. Improving data Objectives To determine the frequency of use and sharing between acute hospitals spatial distribution of health record systems in the English ► This study used a large national-level administrative in England: an overview of National Health Service (NHS). To quantify transitions of health record system distribution data set to identify transitions of care between acute care between acute hospital trusts and health record and retrospective observational National Health Service (NHS) hospital trusts. systems to guide improvements to data sharing and analysis of inter- hospital ► The use of recent administrative data ensures that interoperability. transitions of care. BMJ Open the findings from this study are relevant to current Design Retrospective observational study using Hospital 2019;9:e031637. doi:10.1136/ practice and policy. bmjopen-2019-031637 Episode Statistics. ► Health record system information relating to each Setting Acute hospital trusts in the NHS in England. Protected by copyright. Prepublication history for acute NHS hospital trust in England facilitated a ► Participants All adult patients resident in England that this paper is available online. comprehensive overview of health record system had one or more inpatient, outpatient or accident and To view these files, please visit distribution at this level of care. -
Annual Report & Accounts
ANNUAL REPORT & ACCOUNTS 2017/18 Aintree University Hospital NHS Foundation Trust Annual Report and Accounts 2017/18 Presented to Parliament pursuant to Schedule 7, Paragraph 25 (4) (a) of the National Health Service Act 2006 Contents Chairman’s Foreword 6 Quality Report 2017/18 66 3 Performance Report 8 1 Governance & Organisational n Overview 10 4 Arrangements 124 Aintree University Hospital NHS Foundation Trust 10 n Code of Governance 126 Chief Executive’s statement on Council of Governors 126 Aintree’s performance in 2017/18 14 • Nominations Committee 128 • Achievements in 2017/18 16 • Membership & Membership Committee 128 Key issues and risks in delivery Board of Directors 129 of Trust objectives 20 • Audit Committee 135 Going concern disclosure 21 • Remuneration & Nominations Committee 138 n Performance Analysis 22 n Head of Internal Audit Opinion 139 Operational Performance 22 Financial Performance 26 n Statement of the Chief Investing in the Estate Infrastructure 29 Executive’s responsibilities Corporate & Social Responsibility 30 as Accounting Officer 140 • Community Engagement 30 • Sustainability and Environmental Performance 31 n Independent Auditors’ Report 141 • Equality, Diversity & Inclusion 33 n Annual Governance Statement 2017/18 148 Accountability Report 34 2 n Directors’ Report 36 Accounts 2017/18 154 Board of Directors 36 5 Foreword to the Accounts 156 NHS Improvement’s Single Oversight Framework 37 Accounts for the 12 months Quality Governance 39 April 2017 to March 2018 157 Responding to Patients 40 Volunteers Service 42 Research & Development 43 n Staff Report 49 Staff Engagement & Well-being 49 • Education & Learning 50 • Staff Survey 51 • Improving Staff Health & Well-being 54 • Occupational Health 56 Off-payroll arrangements 57 Remuneration Report 62 © 2018 Aintree University Hospital NHS Foundation Trust Chairman’s Foreword Welcome to our 2017/18 Annual Report where we share with you some of Aintree’s achievements and challenges over the past year in providing services to our communities across North Mersey. -

The Future of Children's and Maternity Services at the Friarage Hospital
The future of children’s and maternity services at the Friarage Hospital, Northallerton Public engagement event – Thursday 22 May 2012 Tennants Auction House, Leyburn The panel Name Role Cllr Jim Clark Cllr Clark chaired tonight’s meeting. He also chairs the North Yorkshire Scrutiny of Health Committee. Vicky Pleydell Dr Pleydell is a local GP. She is also the Shadow Accountable Officer and tonight’s lead clinician from the Hambleton, Richmondshire and Whitby Clinical Commissioning Group Fiona Dr Hampton is a consultant paediatrician and clinical director of paediatrics Hampton and community child health and was tonight’s lead clinician from South Tees Hospitals NHS Foundation Trust Many of the questions and consultant paediatrician’s comments made below were in the context of the current thinking that option 5 is the preferred option of doctors and staff working with children at the Friarage Hospital – which was discussed in detail during the presentation. Q & A What happens if a child had a tonsillectomy or other procedure as a day case but was too unwell to go home overnight? Fiona Hampton – The child would need to be transferred to another hospital. What would happen if you needed an emergency caesarean section and James Cook was full? I’ve heard that Darlington, York and Harrogate will only take planned caesarean sections? Fran Toller (a midwife and divisional manager for women and children at South Tees Hospitals NHS Foundation Trust) – I can understand people’s concerns. If a caesarean section was required you want to be assured that you would get that care from whichever hospital you went to. -

South Tees Hospitals NHS Foundation Trust: Annual Report And
South Tees Hospitals NHS Foundation Trust Annual Report and Accounts 1 April 2018 to 31 March 2019 South Tees Hospitals NHS Foundation Trust Annual Report and Accounts 1 April 2018 to 31 March 2019 Presented to Parliament pursuant to Schedule 7, paragraph 25 (4)(a) of the National Health Service Act 2006 © 2019 South Tees Hospitals NHS Foundation Trust Contents 1 Performance report ..................................................................... 07 Introduction to South Tees Hospitals NHS Foundation Trust ............ 09 Overview by the Chairman and Chief Executive .............................. 10 Delivery of our 2018/19 Annual Plan ............................................... 24 Strategic Direction .......................................................................... 46 2 Accountability report .................................................................. 51 Director’s Report ............................................................................ 53 Foundation Trust Membership ........................................................ 54 Council of Governors ...................................................................... 56 Board of Directors .......................................................................... 60 Annual Remuneration Report ......................................................... 70 Staff Report .................................................................................... 82 Compliance with NHS Foundation Trust Code of Governance ......... 98 NHS Improvement’s Single Oversight -

Annual Report and Accounts 1 April 2011 to 31 March 2012
Annual Report and Accounts 1 April 2011 to 31 March 2012 Our mission is to deliver world-class outcomes, dependable safety and an outstanding experience for patients, their families and carers. South Tees Hospitals NHS Foundation Trust Annual report and Accounts 1 April 2011 to 31 March 2012 Presented to Parliament pursuant to Schedule 7, paragraph 25 (4) of the National Health Service Act 5 Contents South Tees Hospitals NHS Foundation Trust Annual Report 2012 7 9 13 17 Chairman and Directors report About the Highlights of chief executive’s and business trust the year statement review 21 37 47 29 Service Patient experience Keeping Our performance developments and and the you safe change environment 53 63 69 75 Partnerships and The board of Our staff Sustainability engagement directors 81 83 87 91 Audit Remuneration Council of Membership Committee Report Governors 95 Summary of 110 financial Quality account performance “Without the TAVI, Eric could have suffered life- threatening heart failure but just look at him now” - Margaret Leeper, Eric’s wife 7 About the trust South Tees Hospitals NHS Foundation Trust Annual Report 2012 South Tees Hospitals NHS Foundation Trust is the largest hospital trust in the Tees Valley, serving the people of Middlesbrough, Redcar and Cleveland, Hambleton and Richmondshire and beyond. We pride ourselves on patients receiving high quality, safe and efficient healthcare thanks to the hard work and dedication of our staff. The trust runs The James Cook University Hospital in Middlesbrough and the Friarage Hospital in Northallerton providing district general hospital services for the local population. We also provide community services from Hambleton, Richmondshire, Middlesbrough and Redcar and Cleveland including services at: • Redcar Primary Care Hospital • Guisborough Primary Care Hospital • Carter Bequest Hospital in Middlesbrough “Very helpful • East Cleveland Primary Care Hospital in Brotton staff, friendly • The Rutson Rehabilitation Unit in Northallerton and willing to help. -
Benchmark Report
PEN National Awards 2019 Re:thinking the experience Introduction Welcome to PENNA 2019 - our 10th year of celebrating the great work being done to improve the experience of care for both patients and staff. With the ever-increasing uncertainty and challenges in the workplace it is incredibly heartening to see that so many organisations continue to innovate to improve and are willing to share their work. You are what makes PENNA so special so a heartfelt thank you! There is evidence that when there is so much pressure and change we are actually at our most creative, finding ways to do more and be better with less. This year has produced so many fantastic examples of this…..so keep driving forward. PEN will continue to support you by doing our best to share and celebrate these superb examples of best practice. Thank you for joining us Enjoy the day Ruth Evans MBE, Managing Director – Patient Experience Network NHS England and NHS Improvement Every PENNA ceremony has been special but, on this, the tenth anniversary of these awards, we have a rare opportunity to pause and reflect on how important this showcase of patient experience has been, and remains, for the NHS. Over the last decade, the awards have resulted in many hundreds of inspiring stories and many thousands of useful conversations about driving up the quality of experience and delivering what matters most to patients. Not just on the day of the ceremony itself, but through the year, they showcase excellence, innovation, resilience and evolution, helping the system and its partners to share and co-operate in the interests of patients. -

Board of Directors
Board of Directors 5 November 2019 1.30 pm Board Room, Murray Building, James Cook University Hospital MEETING OF THE SOUTH TEES HOSPITALS NHS FOUNDATION TRUST BOARD OF DIRECTORS TO BE HELD IN PUBLIC ON TUESDAY 5 NOVEMBER 2019 AT 1.30 PM IN THE BOARD ROOM, MURRAY BUILDING, JAMES COOK UNVERSITY HOSPITAL AGENDA ITEM PURPOSE LEAD FORMAT 1. Patient Story Discussion Director of Presentation Nursing CHAIR’S BUSINESS 2. Welcome and Introductions Information Chair Verbal 3. Apologies for Absence Information Chair Verbal 4. Quorum and Declarations of Interest Information Chair ENC 1 5. Minutes of the last meetings held on 3 Approval Chair ENC 2 September 2019 6. Matters Arising Review Chair ENC 3 7. Chairman’s report Information Chair Verbal 8. Chief Executive’s report Information Chief Executive Verbal QUALITY AND SAFETY 9. Healthcare-associated Infection Monthly Information Director of ENC 4 Report Nursing & Quality 10. Safe Staffing Monthly Report Information Director of ENC 5 Nursing & Quality 11. Quality, Safety, Performance and Finance Discussion Deputy Chief Presentation / Exception Report Executive/ ENC 6 Director of Nursing and Quality/ Medical Directors/ Director of Finance ITEM PURPOSE LEAD FORMAT PERFORMANCE AND FINANCE 12. 5 Year STP Planning Information Director of ENC 7 Finance 13. Electronic Patient Record update Information Director of ENC 8 Estates, ICT and Healthcare Records 14. EPPR Core Standards report Information Director of ENC 9 Estates, ICT and Healthcare Records 15. Cancelled Operations report Information Chief Operating ENC 10 Officer STRATEGY AND PLANNING 16. Strategic Issues Affecting the Trust and Information Chair Verbal Wider Health Economy update 17.