Patient-Derived Models Recapitulate Heterogeneity of Molecular Signatures and Drug Response in Pediatric High-Grade Glioma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Neuronal Activity Promotes Glioma Growth Through Neuroligin-3 Secretion
Article Neuronal Activity Promotes Glioma Growth through Neuroligin-3 Secretion Graphical Abstract Authors Humsa S. Venkatesh, Tessa B. Johung, ..., Parag Mallick, Michelle Monje Correspondence [email protected] In Brief Neuronal activity promotes the growth of malignant glioma through activity- regulated secretion of the synaptic protein neuroligin-3, which acts as a mitogen, recruiting the PI3K-mTOR pathway to induce glioma cell proliferation. Highlights Accession Numbers d Neuronal activity promotes high-grade glioma (HGG) GSE62563 proliferation and growth d Neuroligin-3 is an activity-regulated secreted glioma mitogen d Neuroligin-3 induces PI3K-mTOR signaling in HGG cells d Neuroligin-3 expression is inversely correlated with survival in human HGG Venkatesh et al., 2015, Cell 161, 803–816 May 7, 2015 ª2015 Elsevier Inc. http://dx.doi.org/10.1016/j.cell.2015.04.012 Article Neuronal Activity Promotes Glioma Growth through Neuroligin-3 Secretion Humsa S. Venkatesh,1,2,3,4,5,9 Tessa B. Johung,1,2,3,4,5,9 Viola Caretti,1,2,3,4,5,9 Alyssa Noll,1,2,3,4,5 Yujie Tang,1,2,3,4,5 Surya Nagaraja,1,2,3,4,5 Erin M. Gibson,1,2,3,4,5 Christopher W. Mount,1,2,3,4,5 Jai Polepalli,6 Siddhartha S. Mitra,5 Pamelyn J. Woo,1,2,3,4,5 Robert C. Malenka,6 Hannes Vogel,1,2,3,4 Markus Bredel,7 Parag Mallick,8 and Michelle Monje1,2,3,4,5,* 1Department of Neurology 2Department of Pediatrics 3Department of Pathology 4Department of Neurosurgery 5Institute for Stem Cell Biology and Regenerative Medicine 6Nancy Pritzker Laboratory, Department of Psychiatry and Behavioral -

Neurooncology at the Limits
50th HEIDELBERG GRAND ROUNDS NeuroOncology at the Limits Chairs: December 9th, 2015 Prof. Dr. Wolfgang Wick 16.00 – 18.00 Prof. Dr. Michael Platten Lecture Hall, DKFZ Please register by 8th December Information and registration: Marketing sponsored by: at the latest. Fortbildungs- und Veranstaltungs- organisation des Nationalen Centrums Roche Pharma AG 1.000€ For this event, two points for für Tumorerkrankungen MSD Sharp & Dohme GmbH 800€ continuing education will be given Heidelberg School of Oncology Mundipharma GmbH 500€ by the Landesärztekammer. Im Neuenheimer Feld 460 Within the practical year, the points 69120 Heidelberg will be recognized in the field of Phone +49 (0)6221.566558 internal medicine and surgery. Fax +49 (0)6221.565094 [email protected] http://www.nct-heidelberg.de/nc/das-nct/veranstaltungen/anmeldung.html Then don‘t miss the far away? Too LIVE-VIDEO- STREAMING 50th HEIDELBERG GRAND ROUNDS on 9th December 2015, 16:00 – 18:00 I will participate. Person/s will accompany me. Fortbildungs- und Veranstaltungs- If not participating no reply necessary. organisation des Nationalen Centrums Name für Tumorerkrankungen Heidelberg School of Oncology First name Im Neuenheimer Feld 460 Location/street 69120 Heidelberg Signature (registration via fax: 06221.565094) 50th HEIDELBERG GRAND ROUNDS Heidelberg Grand Rounds (HGR) Michelle Monje, MD, oncology and a postdoctoral fellowship. The “Ground Rules” PhD joined the faculty scope of her research program encompasses The HGR have been established at Stanford University the molecular determinants of neural precur- as a forum to bring together in 2011 as an Assistant sor cell fate, neuronal-glial interactions, and basic scientists and clinicians. -

Consummate Neuro-Oncologist
THE CONSUMMATE NEURO-ONCOLOGIST Michelle Monje’s teenage project to aid the disabled led her to neurology and a research career that’s bringing new hope for the treatment of childhood brain cancers and the mind-fog caused by chemotherapy. Competitive figure skating was once a big abiding interest in neurology. In keeping part of Michelle Monje’s life. By the time she with her mother’s advice, Monje has over was in middle school in the Bay Area of San the past quarter century made significant Francisco, Monje was squeezing in as many contributions to our understanding of as 35 hours of practice every week at the the brain’s postnatal plasticity and the rink. Then her mother, who’d started at IBM in neurological disorders caused by cancer the late 60’s as a computer programmer and therapies. She has also led the charge worked her way up to the executive ranks, against a swiftly lethal childhood cancer of had a little chat with her. “She pointed out the brainstem known as diffuse intrinsic that dedicating that much time to a sport pontine glioma (DIPG), charting new was great,” Monje recalls, “but perhaps I approaches to the treatment of the long- should also think about how I’m going to be neglected cancer and other high-grade productive and contribute to the rest of the gliomas that she is now—or soon will be— world.” Just 13 at the time, Monje mulled evaluating in clinical trials. the matter for a spell and came up with a precociously fitting answer: She created In 2018, Monje and her colleagues reported a figure skating program for children with in Cell their dissection of the cellular Down syndrome. -
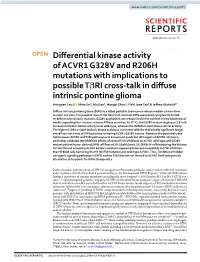
Differential Kinase Activity of ACVR1 G328V and R206H Mutations With
www.nature.com/scientificreports OPEN Diferential kinase activity of ACVR1 G328V and R206H mutations with implications to possible TβRI cross-talk in difuse intrinsic pontine glioma Hongnan Cao 1, Miao Jin2, Mu Gao1, Hongyi Zhou1, Yizhi Jane Tao2 & Jefrey Skolnick1* Difuse intrinsic pontine glioma (DIPG) is a lethal pediatric brain cancer whose median survival time is under one year. The possible roles of the two most common DIPG associated cytoplasmic ACVR1 receptor kinase domain mutants, G328V and R206H, are reexamined in the context of new biochemical results regarding their intrinsic relative ATPase activities. At 37 °C, the G328V mutant displays a 1.8-fold increase in intrinsic kinase activity over wild-type, whereas the R206H mutant shows similar activity. The higher G328V mutant intrinsic kinase activity is consistent with the statistically signifcant longer overall survival times of DIPG patients harboring ACVR1 G328V tumors. Based on the potential cross- talk between ACVR1 and TβRI pathways and known and predicted of-targets of ACVR1 inhibitors, we further validated the inhibition efects of several TβRI inhibitors on ACVR1 wild-type and G328V mutant patient tumor derived DIPG cell lines at 20–50 µM doses. SU-DIPG-IV cells harboring the histone H3.1K27M and activating ACVR1 G328V mutations appeared to be less susceptible to TβRI inhibition than SF8628 cells harboring the H3.3K27M mutation and wild-type ACVR1. Thus, inhibition of hidden oncogenic signaling pathways in DIPG such as TβRI that are not limited to ACVR1 itself may provide alternative entry points for DIPG therapeutics. Difuse intrinsic pontine glioma (DIPG) is an aggressive brainstem pediatric cancer with no efective treatment and a median survival of less than a year according to the International DIPG Registry1. -
Program Booklet
Program Description The NIH Common Fund, in the Office of the Director, supports programs that address key roadblocks in biomedical, behavioral, and social science research impeding basic scientific discovery and its translation into improved human health. Common Fund programs are designed to have broad impact, be catalytic, and tackle challenges that no other entity, including individual NIH Institutes, will be likely or able to do. There currently are 25 different Common Fund programs, spanning the broad mission of NIH. More information is available at commonfund.nih.gov. The NIH Common Fund’s High-Risk, High-Reward Research program was created to accelerate the pace of biomedical, behavioral, and social science discoveries by supporting exceptionally creative scientists with highly innovative research ideas of unusually broad impact. Four initiatives within this program—the NIH Director’s Pioneer, New Innovator, Transformative Research, and Early Independence Awards—serve distinct purposes in achieving this goal. Pioneer Award: Supports individual scientists of exceptional creativity at any career stage who propose bold, pioneering approaches to address major challenges. New Innovator Award: Supports unusually creative early career stage investigators with highly innovative research ideas with the potential for broad impact. Transformative Research Award: Supports individuals or teams proposing exceptionally innovative and/or unconventional research projects that have the potential to create or overturn fundamental paradigms. Early Independence Award: Provides a mechanism for outstanding junior scientists to move rapidly into independent research positions by omitting the traditional postdoctoral training period. 2019 High-Risk, High-Reward Research Symposium | 1 2 | 2019 High-Risk, High-Reward Research Symposium Agenda Wednesday, June 5, 2019 9:00 a.m. -

2011 Annual Report 2011 Annual Report Table of Contents
Institute for Stem Cell Biology and Regenerative Medicine 2011 Annual Report 2011 Annual Report Table of Contents 2 Director’s Statement 4 The New Stem Cell Therapy Center CIRM Disease Teams 6 CD47 and Cancer 7 iPS Cells and Skin Diseases 8 Blood Stem Cell Transplantation Research 10 Embryonic and iPS Cells 15 Cancer Stem Cells 20 Tissue-Specific (Adult) Stem Cells 24 Program in Regenerative Medicine Education 26 PhD Program 26 CIRM Training Grants 27 Training Course in Stem Cell Techniques 28 People at the Institute 32 Institute Members and Associate Members 36 New Funding in 2011 37 Development 38 2011 Publications Director’s Statement 2 The institute was established nearly ten years ago, with a vision of building basic and translational stem cell science through collaboration across every area of scientific research.We have succeeded spectacularly, creating a uniquely strong program that is poised to fundamentally change medicine in the next decade. A number of research initiatives at the institute are rapidly heading toward clinical trials. One very exciting effort concerns CD47, a cell surface protein that protects cancer from the immune system and seems to be found on nearly every kind of cancer. In the coming years, we will be moving forward with preparations for a clinical trial of the anti-CD47 antibody. When this antibody blocks the CD-47 “don’t eat me” signal on cancer cells, the body’s own immune system attacks the cancer, shrinking large tumors, eliminating small ones, and blocking the metastatic spread of cancer. Renee Reijo Pera, in conjuction with Stanford bioengineers, has developed a system to monitor the development of blastocysts produced by in-vitro fertilization, so that only the most viable embryos are used for implantation. -

Pediatric High-Grade Glioma: Biologically and Clinically in Need of New Thinking
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Neurology Faculty Publications Neurology 2-1-2017 Pediatric high-grade glioma: biologically and clinically in need of new thinking. Chris Jones Matthias A Karajannis David T W Jones Mark W Kieran Michelle Monje See next page for additional authors Follow this and additional works at: https://hsrc.himmelfarb.gwu.edu/smhs_neuro_facpubs Part of the Neurology Commons, and the Oncology Commons APA Citation Jones, C., Karajannis, M., Jones, D., Kieran, M., Monje, M., Baker, S., Packer, R., & +several additional authors (2017). Pediatric high- grade glioma: biologically and clinically in need of new thinking.. Neuro Oncology, 19 (2). http://dx.doi.org/10.1093/neuonc/ now101 This Journal Article is brought to you for free and open access by the Neurology at Health Sciences Research Commons. It has been accepted for inclusion in Neurology Faculty Publications by an authorized administrator of Health Sciences Research Commons. For more information, please contact [email protected]. Authors Chris Jones, Matthias A Karajannis, David T W Jones, Mark W Kieran, Michelle Monje, Suzanne J Baker, Roger J Packer, and +several additional authors This journal article is available at Health Sciences Research Commons: https://hsrc.himmelfarb.gwu.edu/smhs_neuro_facpubs/402 153 Review Neuro-Oncology 19(2), 153–161, 2017 | doi:10.1093/neuonc/now101 | Advance Access date 9 June 2016 Pediatric high-grade glioma: biologically and clinically in need of new thinking Chris Jones, Matthias A. Karajannis, David T. W. Jones, Mark W. Kieran, Michelle Monje, Suzanne J. Baker, Oren J. Becher, Yoon-Jae Cho, Nalin Gupta, Cynthia Hawkins, Darren Hargrave, Daphne A. -

Michelle Monje
Michelle Monje Associate Professor of Neurology and, by courtesy, of Neurosurgery, of Pediatrics, of Pathology and of Psychiatry and Behavioral Sciences Neurology & Neurological Sciences CLINICAL OFFICES ACADEMIC CONTACT INFORMATION • Division of Child Neurology • Administrative Assistant 265 Campus Dr Rm G3077 Julie Hitchcock - Administrative Assistant Lokey Stem Cell Bldg Email [email protected] Palo Alto, CA 94305 Tel (650) 721-8564 Tel (650) 736-0885 Fax (650) 724-5824 • Child Neurology 750 Welch Rd Ste 317 MC 5784 Palo Alto, CA 94304 Tel (650) 736-0885 Fax (650) 723-7299 • Pediatric Oncology Clinic 725 Welch Rd Ste 150 Palo Alto, CA 94304 Tel (650) 497-8953 Fax (650) 497-8101 Bio CLINICAL FOCUS • Neurology • Neuro Oncology ACADEMIC APPOINTMENTS • Associate Professor, Neurology & Neurological Sciences • Associate Professor (By courtesy), Neurosurgery • Associate Professor (By courtesy), Pediatrics - Operations • Associate Professor (By courtesy), Pathology • Associate Professor (By courtesy), Psychiatry and Behavioral Sciences • Member, Bio-X • Member, Institute for Stem Cell Biology and Regenerative Medicine • Member, Maternal & Child Health Research Institute (MCHRI) • Member, Stanford Cancer Institute Page 1 of 4 Michelle Monje http://cap.stanford.edu/profiles/Michelle_Monje-Deisseroth/ • Member, Wu Tsai Neurosciences Institute HONORS AND AWARDS • Young Investigator Award, Hagerty Foundation for Glioma Research (2006) • K08 Mentored Clinical Scientist Career Development Award, National Institutes of Neurological Disorders and -

Eighty Seventh Annual Meeting of the American Association of Neuropathologists
PROGRAM EIGHTY SEVENTH ANNUAL MEETING OF THE AMERICAN ASSOCIATION OF NEUROPATHOLOGISTS JUNE 23-26, 2011 SHERATON SEATTLE HOTEL SEATTLE, WASHINGTON This activity is sponsored by the American Association of Neuropathologists For additional information about the accreditation of this program, please contact the AANP office at 216-368-3671 or via email at [email protected] CONTENTS Page AANP Organization Officers and Committees 1-2 CME Information 3-4 Disclosures 4-10 General Information – Hotel and Registration 11 Author/ Presenter Information PowerPoint Presenters 11 Poster Presenters 12 Speaker Ready Room 13 Microscope Room 13 Business Meeting 13 Special Meetings 13 Published Abstracts 14 Annual Reception 14 Meeting Sponsors and Donors 14 Hotel Floor Plan 15 Program and Scientific Sessions Overview 16 MEETING AT A GLANCE 17-18 Special Course 19 Trainee Lunch and Special Lecture 20 Presidential Symposium 21 Scientific Sessions Platform Presentations Friday Morning (Abstracts 1-16) 22-23 Friday Afternoon (Abstracts 17-32) 24-25 Saturday Morning (Abstracts 97-112) 30-31 Saturday Afternoon (Abstracts 113-128) 32-33 Poster Presentations Friday Poster Session I (Abstracts 33-96) Saturday Poster Session II (Abstracts 129-192) 26-29 34-37 SPECIAL LECTURES 38-44 MERITORIOUS AWARDS 45-48 PRESIDENTIAL SYMPOSIUM 49-57 Author Index 58 AMERICAN ASSOCIATION OF NEUROPATHOLOGISTS Office of Secretary-Treasurer C. Harker Rhodes, MD, PhD Pathology Department Dartmouth Hitchcock Medical Center Borwell 530W, DHMC 1 Medical Drive Lebanon, NH 03756 Phone: 603-650-7744 Administrative Assistant – Peggy Harris Phone: 216-368-3671 Email: [email protected] Home page http://www.neuropath.org OFFICERS Steven A. Moore, MD, PhD, University of Iowa College of Medicine, President Arie Perry, MD, University of California San Francisco, Vice-President Raymond A. -

Neuro-Oncology Fairmont Orchid Hotel Cme Conference Waimea, Hawaii
July 23-27, 2018 Asia-Pacific NEURO-ONCOLOGY FAIRMONT ORCHID HOTEL CME CONFERENCE WAIMEA, HAWAII Join us for our inaugural 5-day comprehensive educational conference on neuro-oncology. Presenters from around the world will share their expertise on this ever evolving multi-disciplinary field. Register by June 4, 2018 to receive $100 off your registration fee! COURSE DIRECTOR Tracy Batchelor, M.D. Massachusetts General Hospital Cancer Center COURSE CO-DIRECTORS Nino Chiocca, M.D., Ph.D. Nancy Tarbell, M.D. Brigham and Women’s Hospital Harvard Medical School Jay Loeffler, M.D. Patrick Wen, M.D. Massachusetts General Hospital Dana-Farber Cancer Institute www.hms-apno.com General Information Overview Neuro-oncology is a rapidly evolving multi-disciplinary field, which involves the medical, surgical and radiation management of adult and pediatric patients with primary and metastatic brain and spinal cord tumors. In addition, modern molecular neuropathology and neuroradiology concepts are essential for accurate diagnosis and classification. This five-day CME course is designed to provide an international audience with a comprehensive review of the diagnosis and management of adult and pediatric patients with primary and metastatic brain and spinal cord tumors and neurologic complications of cancer. Target Audience This course is targeted to health care specialists involved in the care of adult and pediatric neuro-oncology patients (oncologists, radiation oncologists, neurosurgeons, neurologists, neuroradiologists, and Conference Site neuropathologists). -

OMB No. 0925-0046, Biographical Sketch Format Page
OMB No. 0925-0001 and 0925-0002 (Rev. 03/2020 Approved Through 02/28/2023) BIOGRAPHICAL SKETCH Provide the following information for the Senior/key personnel and other significant contributors. Follow this format for each person. DO NOT EXCEED FIVE PAGES. NAME: Michelle Monje MD PhD eRA COMMONS USER NAME (credential, e.g., agency login): deisseroth.michelle POSITION TITLE: Associate Professor of Neurology and Neurological Sciences EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, include postdoctoral training and residency training if applicable. Add/delete rows as necessary.) DEGREE Completion (if Date FIELD OF STUDY INSTITUTION AND LOCATION applicable) MM/YYYY Vassar College, Poughkeepsie, NY BA 05/1998 Biology Stanford University, Stanford, CA PhD 05/2004 Neuroscience Stanford University, Stanford, CA MD 05/2004 Medicine Stanford University/Stanford Hospital, Stanford, CA 06/2005 Medicine Internship Harvard Medical School/MGH/BWH, Boston, MA 06/2008 Neurology Residency Stanford University/Lucile Packard Children’s 06/2010 Neuro-Oncology Hospital, Stanford, CA Fellowship Stanford University, Stanford California 10/2011 Postdoctoral Fellowship in Cancer Biology A. Personal Statement I am a neuroscientist and neuro-oncologist whose research program focuses at the intersection of neuroscience and brain cancer biology on neuron-glial interactions in health and oncological disease. The regulation of normal and malignant glial cells by neuronal activity is an area of particular emphasis. -
Undergraduate Summer Research Program 2020 Stanford Bio-X Undergraduate Summer Research Program
UNDERGRADUATE SUMMER RESEARCH PROGRAM 2020 STANFORD BIO-X UNDERGRADUATE SUMMER RESEARCH PROGRAM 2019 Undergraduate Summer Research Program (USRP) Participants The outbreak of COVID-19 has placed tremendous and unanticipated pressures on individuals and organizations around the world. The Stanford community, with its unique culture of collaboration and innovation, has risen to the challenge. Faculty, students, and staff from countless departments have come together and pooled resources to provide new insights by studying the virus, analyzing and predict- ing its spread, and diligently researching tests and treatments. Stanford has also hosted numerous virtual conferences attended by thousands worldwide. Facing the pandemic head-on, for the 16th year of our Stanford Bio-X Undergraduate Summer Research Program, we have successfully adapted the program to allow for a vibrant, valuable, and fulfilling virtual undergraduate experience, maintaining our com- mitment to sharpening students’ research skills and techniques despite the distance. The Stanford Bio-X USRP has provided a ten-week summer research opportunity to a total of 708 students to date. We have partnered with 303 Stanford faculty mentors to provide this one-of-a-kind educational opportunity to these passionate young researchers. Our 2020 cohort of 66 students and 5 student mentors and their respective laboratories have adjusted the students’ projects so that their research can be conducted long-distance. Bio-X has sustained the hallmarks of our summer program in a virtual format so that students can participate live from home. Numerous workshops throughout the spring and summer quarters explore a variety of research-related skills, including analyzing manuscripts, formulating scientific questions, designing experiments, preparing posters, and more.