Mono- Or Poly- Antimicrobial Prophylaxis in Colorectal Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Download Download
VOLUME 7 NOMOR 2 DESEMBER 2020 ISSN 2548 – 611X JURNAL BIOTEKNOLOGI & BIOSAINS INDONESIA Homepage Jurnal: http://ejurnal.bppt.go.id/index.php/JBBI IN SILICO STUDY OF CEPHALOSPORIN DERIVATIVES TO INHIBIT THE ACTIONS OF Pseudomonas aeruginosa Studi In Silico Senyawa Turunan Sefalosporin dalam Menghambat Aktivitas Bakteri Pseudomonas aeruginosa Saly Amaliacahya Aprilian*, Firdayani, Susi Kusumaningrum Pusat Teknologi Farmasi dan Medika, BPPT, Gedung LAPTIAB 610-612 Kawasan Puspiptek, Setu, Tangerang Selatan, Banten 15314 *Email: [email protected] ABSTRAK Infeksi yang diakibatkan oleh bakteri gram-negatif, seperti Pseudomonas aeruginosa telah menyebar luas di seluruh dunia. Hal ini menjadi ancaman terhadap kesehatan masyarakat karena merupakan bakteri yang multi-drug resistance dan sulit diobati. Oleh karena itu, pentingnya pengembangan agen antimikroba untuk mengobati infeksi semakin meningkat dan salah satu yang saat ini banyak dikembangkan adalah senyawa turunan sefalosporin. Penelitian ini melakukan studi mengenai interaksi tiga dimensi (3D) antara antibiotik dari senyawa turunan Sefalosporin dengan penicillin-binding proteins (PBPs) pada P. aeruginosa. Tujuan dari penelitian ini adalah untuk mengklarifikasi bahwa agen antimikroba yang berasal dari senyawa turunan sefalosporin efektif untuk menghambat aktivitas bakteri P. aeruginosa. Struktur PBPs didapatkan dari Protein Data Bank (PDB ID: 5DF9). Sketsa struktur turunan sefalosporin digambar menggunakan Marvins Sketch. Kemudian, studi mengenai interaksi antara antibiotik dan PBPs dilakukan menggunakan program Mollegro Virtual Docker 6.0. Hasil yang didapatkan yaitu nilai rerank score terendah dari kelima generasi sefalosporin, di antaranya sefalotin (-116.306), sefotetan (-133.605), sefoperazon (-160.805), sefpirom (- 144.045), dan seftarolin fosamil (-146.398). Keywords: antibiotik, penicillin-binding proteins, P. aeruginosa, sefalosporin, studi interaksi ABSTRACT Infections caused by gram-negative bacteria, such as Pseudomonas aeruginosa, have been spreading worldwide. -

Drug-Induced Anaphylaxis in China: a 10 Year Retrospective Analysis of The
Int J Clin Pharm DOI 10.1007/s11096-017-0535-2 RESEARCH ARTICLE Drug‑induced anaphylaxis in China: a 10 year retrospective analysis of the Beijing Pharmacovigilance Database Ying Zhao1,2,3 · Shusen Sun4 · Xiaotong Li1,3 · Xiang Ma1 · Huilin Tang5 · Lulu Sun2 · Suodi Zhai1 · Tiansheng Wang1,3,6 Received: 9 May 2017 / Accepted: 19 September 2017 © The Author(s) 2017. This article is an open access publication Abstract Background Few studies on the causes of (50.1%), mucocutaneous (47.4%), and gastrointestinal symp- drug-induced anaphylaxis (DIA) in the hospital setting are toms (31.3%). A total of 249 diferent drugs were involved. available. Objective We aimed to use the Beijing Pharma- DIAs were mainly caused by antibiotics (39.3%), traditional covigilance Database (BPD) to identify the causes of DIA Chinese medicines (TCM) (11.9%), radiocontrast agents in Beijing, China. Setting Anaphylactic case reports from (11.9%), and antineoplastic agents (10.3%). Cephalospor- the BPD provided by the Beijing Center for Adverse Drug ins accounted for majority (34.5%) of antibiotic-induced Reaction Monitoring. Method DIA cases collected by the anaphylaxis, followed by fuoroquinolones (29.6%), beta- BPD from January 2004 to December 2014 were adjudi- lactam/beta-lactamase inhibitors (15.4%) and penicillins cated. Cases were analyzed for demographics, causative (7.9%). Blood products and biological agents (3.1%), and drugs and route of administration, and clinical signs and plasma substitutes (2.1%) were also important contributors outcomes. Main outcome measure Drugs implicated in DIAs to DIAs. Conclusion A variety of drug classes were impli- were identifed and the signs and symptoms of the DIA cases cated in DIAs. -

PHARMACEUTICAL APPENDIX to the TARIFF SCHEDULE 2 Table 1
Harmonized Tariff Schedule of the United States (2020) Revision 19 Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2020) Revision 19 Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names INN which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service CAS registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. -

Consideration of Antibacterial Medicines As Part Of
Consideration of antibacterial medicines as part of the revisions to 2019 WHO Model List of Essential Medicines for adults (EML) and Model List of Essential Medicines for children (EMLc) Section 6.2 Antibacterials including Access, Watch and Reserve Lists of antibiotics This summary has been prepared by the Health Technologies and Pharmaceuticals (HTP) programme at the WHO Regional Office for Europe. It is intended to communicate changes to the 2019 WHO Model List of Essential Medicines for adults (EML) and Model List of Essential Medicines for children (EMLc) to national counterparts involved in the evidence-based selection of medicines for inclusion in national essential medicines lists (NEMLs), lists of medicines for inclusion in reimbursement programs, and medicine formularies for use in primary, secondary and tertiary care. This document does not replace the full report of the WHO Expert Committee on Selection and Use of Essential Medicines (see The selection and use of essential medicines: report of the WHO Expert Committee on Selection and Use of Essential Medicines, 2019 (including the 21st WHO Model List of Essential Medicines and the 7th WHO Model List of Essential Medicines for Children). Geneva: World Health Organization; 2019 (WHO Technical Report Series, No. 1021). Licence: CC BY-NC-SA 3.0 IGO: https://apps.who.int/iris/bitstream/handle/10665/330668/9789241210300-eng.pdf?ua=1) and Corrigenda (March 2020) – TRS1021 (https://www.who.int/medicines/publications/essentialmedicines/TRS1021_corrigenda_March2020. pdf?ua=1). Executive summary of the report: https://apps.who.int/iris/bitstream/handle/10665/325773/WHO- MVP-EMP-IAU-2019.05-eng.pdf?ua=1. -

Pharmaceutical Appendix to the Harmonized Tariff Schedule
Harmonized Tariff Schedule of the United States Basic Revision 3 (2021) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States Basic Revision 3 (2021) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names INN which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service CAS registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. -

BMJ Open Is Committed to Open Peer Review. As Part of This Commitment We Make the Peer Review History of Every Article We Publish Publicly Available
BMJ Open is committed to open peer review. As part of this commitment we make the peer review history of every article we publish publicly available. When an article is published we post the peer reviewers’ comments and the authors’ responses online. We also post the versions of the paper that were used during peer review. These are the versions that the peer review comments apply to. The versions of the paper that follow are the versions that were submitted during the peer review process. They are not the versions of record or the final published versions. They should not be cited or distributed as the published version of this manuscript. BMJ Open is an open access journal and the full, final, typeset and author-corrected version of record of the manuscript is available on our site with no access controls, subscription charges or pay-per-view fees (http://bmjopen.bmj.com). If you have any questions on BMJ Open’s open peer review process please email [email protected] BMJ Open Pediatric drug utilization in the Western Pacific region: Australia, Japan, South Korea, Hong Kong and Taiwan Journal: BMJ Open ManuscriptFor ID peerbmjopen-2019-032426 review only Article Type: Research Date Submitted by the 27-Jun-2019 Author: Complete List of Authors: Brauer, Ruth; University College London, Research Department of Practice and Policy, School of Pharmacy Wong, Ian; University College London, Research Department of Practice and Policy, School of Pharmacy; University of Hong Kong, Centre for Safe Medication Practice and Research, Department -

WO 2011/089216 Al
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date t 28 July 2011 (28.07.2011) WO 2011/089216 Al (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 47/48 (2006.01) C07K 1/13 (2006.01) kind of national protection available): AE, AG, AL, AM, C07K 1/1 07 (2006.01) AO, AT, AU, AZ, BA, BB, BG, BH, BR, BW, BY, BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, (21) Number: International Application DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, PCT/EP201 1/050821 HN, HR, HU, ID, J , IN, IS, JP, KE, KG, KM, KN, KP, (22) International Filing Date: KR, KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, 2 1 January 201 1 (21 .01 .201 1) ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, PE, PG, PH, PL, PT, RO, RS, RU, SC, SD, (25) Filing Language: English SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, (26) Publication Language: English TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (30) Priority Data: (84) Designated States (unless otherwise indicated, for every 1015 1465. 1 22 January 2010 (22.01 .2010) EP kind of regional protection available): ARIPO (BW, GH, GM, KE, LR, LS, MW, MZ, NA, SD, SL, SZ, TZ, UG, (71) Applicant (for all designated States except US): AS- ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, MD, RU, TJ, CENDIS PHARMA AS [DK/DK]; Tuborg Boulevard TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, 12, DK-2900 Hellerup (DK). -

Currently Available Antimicrobial Agents and Their Potential for Use As Monotherapy L
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector REVIEW 10.1111/j.1469-0691.2008.02125.x Currently available antimicrobial agents and their potential for use as monotherapy L. R. Peterson Northwestern University’s Feinberg School of Medicine, Departments of Medicine and Pathology, Chicago, IL; Evanston Northwestern Healthcare, Department of Medicine, Division of Infectious Diseases and Department of Pathology and Laboratory Medicine, Division of Microbiology, Evanston, IL, USA ABSTRACT Infectious diseases remain a serious and now re-emerging threat to human life, contributing to over ten million deaths per year. Treatment of major infectious diseases with antibacterial agents creates an ongoing and escalating public health issue that currently leads to more problems than solutions. By processes of adaptation and survival, bacteria consistently develop mechanisms to overcome the effects of the newest and most potent antibacterial compounds. Simultaneously, progressively fewer antibacterial agents are being developed by pharmaceutical and biotechnology companies. Although this dilemma is an inherent trade-off and has no imminent resolution, the most prudent paradigm to pursue is the judicious use of antibacterial agents in the most limited way possible to attain the desired treatment results. One straightforward approach to antimicrobial stewardship is to use a single agent as opposed to combination therapy, so as to subject bacteria to lower total antibiotic exposure whenever feasible. This article reviews current trends in antibacterial drug development and describes a context for adherence to monotherapy with newer agents. Keywords Antibiotic resistance, antimicrobial stewardship, glycylcycline, monotherapy, tigecycline Clin Microbiol Infect 2008; 14 (Suppl. -
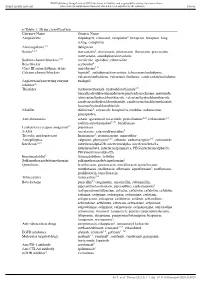
E-Table 1. Drug Classification Category Name Generic Name
BMJ Publishing Group Limited (BMJ) disclaims all liability and responsibility arising from any reliance Supplemental material placed on this supplemental material which has been supplied by the author(s) Thorax e-Table 1. Drug classification Category Name Generic Name Antiplatelets clopidogrel, cilostazol, ticlopidine2, beraprost, beraprost–long acting, complavin Anticoagulants 2,3 dabigatran Statins1,2,3 atorvastatin2, simvastatin, pitavastatin, fluvastatin, pravastatin, rosuvastatin, amlodipine/atorvastatin Sodium channel blockers4,5† mexiletine, aprindine, cibenzoline Beta blocker acebutolol2 Class III antiarrhythmic drugs amiodarone1–6 Calcium channel blockers bepridil1, amlodipine/atorvastatin, telmisartan/amlodipine, valsartan/amlodipine, valsartan/cilnidipine, candesartan/amlodipine Angiotensin/converting enzyme enalapril inhibitor2‡ Thiazides trichlormethiazide, hydrochlorothiazide3,5, benzylhydrochlorothiazide/reserpine/carbazochrome, mefruside, telmisartan/hydrochlorothiazide, valsartan/hydrochlorothiazide, candesartan/hydrochlorothiazide, candesartan/trichlormethiazide, losartan/hydrochlorothiazide NSAIDs diclofenac2, celecoxib, loxoprofen, etodolac, nabumetone, pranoprofen Anti-rheumatics actarit, iguratimod, tofacitinib, penicillamine2–5, leflunomide1,3, sodium aurothiomalate2–6#, bucillamine Leukotriene receptor antagonist2* pranlukast 5-ASA mesalazine, salazosulfapyridine5 Tricyclic antidepressant Imipramine5, cromipramine, maprotiline Antiepileptics valproate, phenytoin2,3,5, ethotoin, carbamazepine2–5, zonisamide Interferon1,2,3 -

Revision of Precautions
Published by Translated by Ministry of Health, Labour and Welfare Pharmaceuticals and Medical Devices Agency This English version is intended to be a reference material to provide convenience for users. In the event of inconsistency between the Japanese original and this English translation, the former shall prevail. Revision of Precautions Cefmenoxime hydrochloride Ceftibuten hydrate Cefaclor Cefazolin sodium Cefazolin sodium hydrate Cefalexin Cefalotin sodium Cefixime hydrate Cefepime dihydrochloride hydrate Cefozopran hydrochloride Cefotiam hydrochloride Cefoperazone sodium/sulbactam sodium Cefcapene pivoxil hydrochloride hydrate Cefditoren pivoxil Pharmaceuticals and Medical Devices Agency 3-3-2 Kasumigaseki, Chiyoda-ku, Tokyo 100-0013 Japan E-mail: [email protected] Published by Translated by Ministry of Health, Labour and Welfare Pharmaceuticals and Medical Devices Agency This English version is intended to be a reference material to provide convenience for users. In the event of inconsistency between the Japanese original and this English translation, the former shall prevail. Cefdinir Ceftazidime hydrate Ceftizoxime sodium Cefteram pivoxil Ceftriaxone sodium hydrate Cefpirome sulfate Cefpodoxime proxetil Cefminox sodium hydrate Cefmetazole sodium Cefroxadine hydrate Flomoxef sodium Latamoxef sodium March 28, 2019 Non-proprietary name Cefmenoxime hydrochloride, ceftibuten hydrate, cefaclor, cefazolin sodium, cefazolin sodium hydrate, cephalexin, cefalotin sodium, cefixime hydrate, cefepime dihydrochloride hydrate, cefozopran hydrochloride, cefotiam hydrochloride, cefoperazone Pharmaceuticals and Medical Devices Agency 3-3-2 Kasumigaseki, Chiyoda-ku, Tokyo 100-0013 Japan E-mail: [email protected] Published by Translated by Ministry of Health, Labour and Welfare Pharmaceuticals and Medical Devices Agency This English version is intended to be a reference material to provide convenience for users. In the event of inconsistency between the Japanese original and this English translation, the former shall prevail. -

WHO-EMP-RHT-TSN-2018.1-Eng.Pdf
WHO/EMP/RHT/TSN/2018.1 The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 WHO/EMP/RHT/TSN/2018.1 © World Health Organization [2018] Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances. Geneva: World Health Organization; 2018 (WHO/EMP/RHT/TSN/2018.1). Licence: CC BY-NC-SA 3.0 IGO. -

Point Prevalence Survey of Healthcare-Associated Infections and Antimicrobial Use in European Acute Care Hospitals
TECHNICAL DOCUMENT Point prevalence survey of healthcare-associated infections and antimicrobial use in European acute care hospitals Protocol version 5.3 www.ecdc.europa.eu ECDC TECHNICAL DOCUMENT Point prevalence survey of healthcare- associated infections and antimicrobial use in European acute care hospitals Protocol version 5.3, ECDC PPS 2016–2017 Suggested citation: European Centre for Disease Prevention and Control. Point prevalence survey of healthcare- associated infections and antimicrobial use in European acute care hospitals – protocol version 5.3. Stockholm: ECDC; 2016. Stockholm, October 2016 ISBN 978-92-9193-993-0 doi 10.2900/374985 TQ-04-16-903-EN-N © European Centre for Disease Prevention and Control, 2016 Reproduction is authorised, provided the source is acknowledged. ii TECHNICAL DOCUMENT PPS of HAIs and antimicrobial use in European acute care hospitals – protocol version 5.3 Contents Abbreviations ............................................................................................................................................... vi Background and changes to the protocol .......................................................................................................... 1 Objectives ..................................................................................................................................................... 3 Inclusion/exclusion criteria .............................................................................................................................. 4 Hospitals .................................................................................................................................................