UNIT:3 Water Purification, Process by Which Undesired Chemical
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dual Edition
YEARS # 1 Indian American Weekly : Since 2006 VOL 15 ISSUE 20 ● NEW YORK / DALLAS ● MAY 14 - MAY 20, 2021 ● ENQUIRIES: 646-247-9458 ● [email protected] www.theindianpanorama.news 12 OPPOSITION LEADERS WRITE TO PM MODI, US lifts most mask DEMANDING FREE MASS VACCINATION, guidance in key step back SUSPENSION OF CENTRAL VISTA PROJECT to post - Covid normalcy Fully vaccinated Americans can ditch their masks in most settings, even indoors or in large groups. WASHINGTON (TIP): President Joe Biden took his biggest step yet toward declaring a victory over the coronavirus pandemic - as public health officials said fully vaccinated Americans can ditch their masks in most settings, even indoors or in large groups. "Today is a great day for America in our long battle with coronavirus," Biden said in the In a joint letter to PM Modi, 12 opposition White House Rose Garden on Thursday,May 13, party leaders, including Sonia Gandhi, have demanded Central govt to provide calling the US vaccination program an foodgrains to the needy and Rs 6,000 "historical logistical achievement." monthly to the unemployed. - File photo of The guidance shift Thursday, May 13, is a Prime Minister Narendra Modi | Twitter turning point in the fight against Covid-19 and @BJP4India comes as US caseloads fall and vaccinations NEW DELHI (TIP): In a joint letter rise. It signals a broad return to everyday to Prime Minister Narendra Modi, lifeand is also a bet that any surge in spread May 12, 12 Opposition parties have from relaxed guidelines won't be enough to urged the government to immediately reverse progress in inoculations. -

Issn - 2349-6746 Issn -2349-6738 the Role of Non Governmental Organizations in Promoting Sustainable Development
Research Paper Impact Factor: 5.646 IJMSRR Peer Reviewed & Indexed Journal E- ISSN - 2349-6746 www.ijmsrr.com ISSN -2349-6738 THE ROLE OF NON GOVERNMENTAL ORGANIZATIONS IN PROMOTING SUSTAINABLE DEVELOPMENT Dr. Kanchana Naidu* Dr.Kalpana Naidu* *Asst. Professor,Women’s Chrstian College,Chennai Abstract Sustainable development is a way of using resources without the resources running out for future generations. This development is a multidimensional process and cannot be created by Govt. independently. Other stakeholders are also required to contribute effectively towards enhancing sustainability. The present paper highlights the importance & role of NGOs in promoting sustainable development in India. Introduction Sustainability means meeting the needs of the present without compromising the ability of future generations to meet their needs. Sustainable Development is the organizing principle for meeting human development goals while simultaneously sustaining the ability of natural systems to provide the natural resources and ecosystem services upon which the economy and society depend. The desired result is a state of society where living conditions and resources are used to continue to meet human needs without undermining the integrity and stability of the natural system. It enables to attain a balance between environmental protection and human economic development and between the present and future needs. Sustainable Development implies development of four aspects viz Human, Social, Economic and Environmental. Human Sustainability refers to overall development of human capital by providing proper health, education, skills, knowledge, leadership and access to essential services. Social Sustainability is maintenance of social capital by focusing on investments and services that create the basic framework for society. -
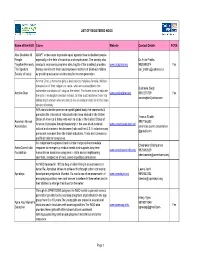
List of Registered Ngos
LIST OF REGISTERED NGOS Name of the NGO Cause Website Contact Details FCRA Able Disabled All ADAPT endeavours to provide equal opportunities to disabled people People especially in the field of education and employment. The society also Dr.Anita Prabhu Together(Formerly conducts awareness programs about rights of the disabled, provides www.adaptssi.org 9820588314 Yes The Spastics therapy services to them and empowers mothers of disabled children [email protected] Society of India) by providing education and training for income generation. Amcha Ghar, a home for girls is dedicated to helpless female children - irrespective of their religion or caste- who are susceptible to the Susheela Singh vulnerable conditions of living on the street. The home aims to educate Amcha Ghar www.amchaghar.org 9892270729 Yes the girls in an English medium school, to train and transform them into amchaghar2yahoo.com skilled adult women who are able to live an independent life in the main stream of society. AAA aims to be the premier non-profit global body that represents & promotes the interests of individuals who have studied in the United Yasmin Shaikh States of America & those who wish to study in the United States of American Alumni 9987156303 America. It provides thought leadership in the area of educational, www.americanalumni.net Association american.alumni.association cultural and economic ties between India and the U.S. It includes many @gmail.com prominent members from the Indian Industries, Trade and Commerce and Multinational companies. An independent registered trust in India that provides immediate Chadrakant Deshpande AmeriCares India response to emergency medical needs and supports long-term www.americaresindia.org 9920692629 Foundation humanitarian assistance programs in India and in neighbouring [email protected] countries, irrespective of race, creed or political persuasion. -

The Tremendous Role of Non-Government Organizations in Lockdown Situation of India
International Journal of Humanities and Social Science Invention (IJHSSI) ISSN (Online): 2319 – 7722, ISSN (Print): 2319 – 7714 www.ijhssi.org ||Volume 9 Issue 8 Ser. II || August 2020 || PP 11-19 The Tremendous Role of Non-Government Organizations in Lockdown Situation of India ShamsherRahaman Assistant Professor, Department of History, VidyasagarMahavidyalaya, University of Calcutta ABSTRACT:Non-Governmental Organizations are still playing a very important role to keep the society safe, generating awareness and development throughout lockdown India. In the eye of the rising COVID-19 storm, non-government organizations, big and small, are performing a massive task. The novel coronavirus lockdown has comfortably cooped most of us at house but marginalized communities in the unorganized sector, such as daily laborers, construction workers, street vendors and people involved in the cottage industry are terribly affected by the economic and social reflection of lockdown. NGOs coming forward to support the migrant workers and to fight the pandemic and provided food, water and transportation at their cost. In this paper I briefly analyze the role and contribution of NGOs (first half of 2020) in the lockdown situation of India. In this situation NGOs become unassuming heroes because they help fill in the gaps that governments often neglect and sprung into action to fill in gaps of communication and delivery of essential items to poor underserved communities. KEYWORDS: Pandemic, NGOs, combat against COVID-19, unassuming heroes, marginalized communities ----------------------------------------------------------------------------------------------------------------------------- ---------- Date of Submission: 28-07-2020 Date of Acceptance: 11-08-2020 ------------------------------------------------------------------------------------------------------------------------ --------------- I. INTRODUCTION The novel coronavirus (Covid-19) has now spread to almost all countries of the world as an epidemic. -

Feminist Research Studies
supporting women to challenge violence and negotiate equality feminist research studies perspective and capacity development on feminist principles and strategiesalliance building and networking supporting women’s leadership and agency annual report2018-19 1 JAGORI TABLE OF CONTENTS INTRODUCTION 1. PERSPECTIVE AND LEADERSHIP BUILDING ON WOMEN’S RIGHTS AND SAFETY 1 A. Feminist Leadership Development Course (FLDC) B. Feminist Counselling Workshop C. Need-based Sessions D. Community Leadership Development Programme (CLDP), Delhi E. Strengthening the Community Women’s Safety Forum (CWSF), Ranchi & Hazaribag F. Partnership with Pradan G. Gender Strategy Development Workshop H. Internship 2. ENABLING WOMEN SURVIVORS OF VIOLENCE 10 A. Crisis Intervention B. Survivor Support Groups C. Collective Interventions D. Interactions with Service Providers E. Internal Committee on Sexual Harassment at the Workplace 3. EXPANDING ENGAGEMENT ON WOMEN’S SAFETY 17 A. Collective Action for Women’s Safety in Delhi B. Creation of Safe Public Spaces for Women and Girls in Jharkhand 4. RESEARCH AND KNOWLEDGE MANAGEMENT 27 A. Research Studies B. Material Production C. Dissemination 5. NETWORKING AND JOINT ACTION 36 A. Campaigns B. Meetings/Consultations Organised/Co-organised by Jagori C. Partner Engagement 6. THE SANGAT PROJECT 45 A. Capacity Building B. Promotion of Feminist Culture, Information, Communication and Media C. Campaigns and Networking 7. INSTITUTION BUILDING 50 A. Organisational Matters B. Capacity Building of the Team C. Monitoring D. Governance Matters ACKNOWLEDGEMENTS 53 FINANCIAL AUDIT 54 BOARD MEMBERS 56 PARTNERS 57 Jagori Annual Report 2018-2019 INTRODUCTION Much has changed in the discourse on women’s rights since Jagori came into being 34 years ago. During this period, Jagori has worked with marginalised women in urban and rural areas primarily on issues around violence against women, women’s rights, and their safety in public spaces. -

JICA India NGO Directory
JICA India NGO Directory S. NO. NAME OF ORGANISATION THEMATIC AREA OPERATIONAL STATE (S) CONTACT INFORMATION Tel: 9871100334 1 17000 Ft Foundation Education Jammu & Kashmir Email: [email protected] Website: http://www.17000ft.org Agriculture, Disaster Prevention, Education, Environment, Forestry, Tel: 9448370387 2 Abhivruddi Society For Social Development Health, Livelihood, Rural Development, Water, Sanitation & Hygiene, Karnataka Email: [email protected] Women Empowerment Website: http://www.abhivruddi.com Tel: 9801331700 Agriculture, Education, Health, Livelihood, Rural Development, Water, 3 Abhivyakti Foundation Jharkhand Email: [email protected] Sanitation & Hygiene, Women Empowerment Website: https://www.avfindia.org/ Tel: 9422702353 Education, Environment, Livelihood, Rural Development, Women 4 Abhivyakti Media For Development Maharashtra Email: [email protected] Empowerment Website: http://www.abhivyakti.org.in Andhra Pradesh, Bihar, Delhi, Gujarat, Haryana, Jharkhand, Karnataka, Tel: 9769500292 5 Accion Technical Advisors India Education, Livelihood, Women Empowerment Madhya Pradesh, Maharashtra, Odisha, Rajasthan, Telangana, Uttarakhand, Email: [email protected] Uttar Pradesh, West Bengal Website: http://www.accion.org Andhra Pradesh, Assam, Chandigarh, Chhattisgarh, Delhi, Goa, Gujarat, Tel: 9810410600 6 Action For Autism Education, Livelihood, Rural Development Haryana, Karnataka, Madhya Pradesh, Maharashtra, Odisha, Punjab, Email: [email protected] Rajasthan, Tamil Nadu, Uttar Pradesh, -

Sdm Self-Sponsored Fellows
resume book system design & management sdm self-sponsored fellows SHWETA AGARWAL 235 Albany Street, Apt # 3069, Cambridge, MA 02139 +1 (917) 435-2825 | [email protected] EDUCATION Massachusetts Institute of Technology Cambridge, MA School of Engineering & Sloan School of Management 08/2016 – 01/2018 Candidate for M.S., System Design and Management, Jan 2018 | CGPA 4.5/5 Active member of Technology, Product Management, FinTech, and Entrepreneurship and Innovation clubs Project: Designed image recognition tool for restaurants to identify customers, their emotion and fetch their food preferences from past records, enabling personalized services to the right customer at the right time GMAT: 720 Indian School of Business (ISB) Hyderabad, India Post Graduate Programme in Management (M.B.A.) 2013 - 2014 Concentration: Information and Technology Management; Marketing Events Coordinator, Women in Business Club; Lead Coordinator, Business Technology Club Galgotias College of Engineering and Technology Greater Noida, India Bachelor of Technology, Electronics and Communication Engineering 2005 - 2009 Graduated 1st / 125 students in my department & among top 5% of university B.Tech batch of ~26,000 students EXPERIENCE Axis Bank Mumbai, India India’s leading private bank, offering a wide range of consumer and corporate banking services; annual turnover: $6.2B Senior Manager, IT - Technology & Digital Innovation Group 05/2014 – 02/2016 Innovation Management and IT Strategy - CIO Advisory Handpicked by the senior management to devise digital transformation -

Top 100 NGO's
S.no Top 50 NGO's on basis of fund raising through SCMM 2009-11 : 50 Bibs 1 The Akanksha Foundation 2 Childline India Foundation 3 Paragon Charitable Trust 4 K.C. Mahindra Education Trust A/C Nanhi Kali 5 The Research Society for the Care, Treatment & Training of Children in Need of Special Care 6 Save The Children India 7 Shrimad Rajchandra Love and Care 8 Concern India Foundation 9 Aseema Charitable Trust 10 CRY - Child Rights and You 11 Mumbai Mobile Creches 12 Cancer Patients Aid Association 13 Helen Keller Institute for Deaf & Deafblind 14 ISHA Education 15 Bhagwan Mahaveer Viklang Sahayata Samiti 16 Iskcon Food Relief Foundation 17 Project Crayons 18 Rotary Club Bombay 19 Deeds Public Charitable Trust 20 Swayamsiddh Matimand Mulansathi Matrupalak Sanstha 21 National Liver Foundation 22 Alert India 23 Apnalaya 24 Vasantha Memorial Trust 25 Catalysts for Social Action 26 ChildLink India Foundation 27 Dignity Foundation 28 Teach to Lead 29 Vidya Integrated Development For Youth and Adults 30 Sanskriti Samvardhan Mandal 31 Salaam Baalak Trust 32 The Indian Council for Mental Health 33 Ummeed Child Development Center 34 HelpAge India 35 Kherwadi Social Welfare Association 36 Atma Education 37 Make a Wish Foundation of India 38 AMAR SEVA SANGAM 39 The Society For Door Step school 40 Seva Sadan Society 41 Maharashtra Dyslexia Association 42 The Foundation 43 Girivanvasi Educational Trust 44 Ballygunge Society for Children In Pain 45 Americares India Foundation 46 The Vatsalya Foundation 47 Nana Nani Foundation 48 Light of Life Trust 49 -

Volunteering in India
VOLUNTEERING IN INDIA Contexts, Perspectives and Discourses 1 Foreword Volunteerism has long been an integral part of the Indian society shaped by traditions and value systems rooted in the religion and cultural interactions. The volunteers from diverse backgrounds have gone about celebrating the spirit of volunteerism in the best manner they know – rendering selfless service to their fellow beings and the community at large. The observance of International Year of Volunteers (IYV) in 2001 underscores the importance of people-to-people relations as core values of volunteerism. The resolution adopted by the UN General Assembly to mark the Tenth Anniversary of the International Year of Volunteers (IYV+10) in 2011 rekindled the spirit of volunteerism and provided the opportunity to reflect on the status and growth of volunteerism worldwide. The role of volunteers in creation and development of social capital, civic engagement and social cohesion is now well documented. Against the backdrop of challenges, exciting new avenues for people to volunteer have opened up. It is also significant to note the role of technological revolution and its contribution to new forms of volunteering like micro-volunteering and online volunteering. These are going to be the key in future forms of volunteering discourses. It is notable that eighty-seven per cent of people aged 15 to 24 live in developing countries. They can play an important role to achieve the Millennium Development Goals adopting various ways to engage. Tenth International year of volunteers (IYV+10) offered the opportunity to the youth world over to further the volunteering agenda through their creativity, energy and commitment. -

SDG CSR LINKAGES.Cdr
CSR Published by Sustainable Development Goals Coordination Centre (SDGCC Haryana) Swarna Jayanti Haryana Institute for Fiscal Management Yojana Bhawan Bays 21-28 Sector 4, Panchkula, Haryana 134112 TABLE OF CONTENT Website: www.sdgcc.in List of Figures 1 Research and Analysis by List of Tables 2 NGOBOX Executive Summary 3 Background 5 Role of Corporate Social Responsibility in addressing the developmental challenges in India 6 CSR-SDG Alignment Matrix Objectives and Methodology 9 Objectives 9 Research Methodology 15 Analytics and Key Findings 17 Location of company head-quarters 21 CSR in Haryana by MNCs 23 Contribution to SDGs by CSR projects by industrial sectors in Haryana 27 Top ten companies contributing to SDGs through CSR projects 29 The budget range of CSR projects 31 CSR thematic foci of organisations 33 Targeted communities through CSR projects 34 SDGs addressed through CSR projects in Haryana 37 Spatial distribution of SDG-aligned CSR projects in Haryana 39 SDG alignment of CSR projects in aspirational districts 41 CSR project implementation 42 CSR projects in collaboration with Government Agencies 45 Company ownership and SDG reporting 47 CSR, governance and project drivers 47 Unspent CSR fund (Fy2019). 50 Corporate Social Responsibility and Key SDGs 51 SDG 4 (Quality Education) 59 Published by Sustainable Development Goals Coordination Centre (SDGCC Haryana) Swarna Jayanti Haryana Institute for Fiscal Management Yojana Bhawan Bays 21-28 Sector 4, Panchkula, Haryana 134112 TABLE OF CONTENT Website: www.sdgcc.in List of Figures -

Spot Improving Menstrual Health and Hygiene in India
Spot Improving Menstrual Health and Hygiene in India USAID Kiawah Trust FROM THE AMERICAN PEOPLE -'USAID FROM THE AMERICAN PEOPLE The United States Agency for International Development (USAID) is the United States federal government agency that provides economic development and humanitarian assistance around the world in support of the foreign policy goals of the United States. USAID works in over 100 countries around the world to promote broadly shared economic prosperity, strengthen democracy and good governance, protect human rights, improve global health, further education and provide humanitarian assistance. This report is made possible by the support of the American People through the United States Agency for International Development (USAID). The contents of this report are the sole responsibility of Dasra and do not necessarily reflect the views of USAID or the United States government. [email protected] Kiawah Trust The Kiawah Trust is a UK family foundation that is committed to improving the lives of vulnerable and disadvantaged adolescent girls in India. The Kiawah Trust believes that educating adolescent girls from poor communities allows them to thrive, to have greater choice in their life and a louder voice in their community. This leads to healthier, more prosperous and more stable families, communities and nations. [email protected] In Sanskrit, Dasra means Enlightened Giving. Dasra is India's leading strategic philanthropy foundation. Dasra works with philanthropists and successful social entrepreneurs to bring together knowledge, funding and people as a catalyst for social change. We ensure that strategic funding and capacity building skills reach non-profit organizations and social businesses to have the greatest impact on the lives of people living in poverty. -

Urban Poverty Vis-A-Vis Informal Sector
International Journal of Science and Research (IJSR) ISSN (Online): 2319-7064 Impact Factor (2012): 3.358 Urban Poverty Vis-A-Vis Informal Sector Gouri Manoj Sattigeri1 MA Economics, D/O Dr.Manoj.Sattigeri, B-101, B-Wing, Nishad Nr Vandana Hospital, Behind Aishwarya Apartments, Ellorapark, Vadodara-390023, Gujarat, India Abstract: India’s population is around 1.21 billion (Census 2011) and rising; 836 million people are poor and 395 million earn their livelihood by working in the informal sector. Developing India and the poor struggling to survive is the common view of India’s urban cities. Poverty is multidimensional; a socio-economic phenomenon which defies any precise definition. Urban poverty has been differentiated by two broad complementary approaches i.e. economic and anthropological interpretations. Urban poor is basically engaged in the urban informal sector. The quest for better livelihood opportunities has led to large-scale migration and the mushrooming of slums in several Indian cities. Several governmental programmes are in progress to alleviate poverty. India now has that rare window of opportunity to improve the quality of life for its 1.2 billion citizens and lay the foundations for a truly prosperous future–a future that will impact the country and its people for generations to come. “The test of our progress is not whether we add more to the abundance of those who have much; it is whether we provide enough for those who have too little.” ― Franklin Roosevelt; bearing this in mind, India must march inclusively forward to realize its dream of “DEVELOPED INDIA”. Keywords: Urban Poverty, Informal Sector, Globalization, Liberalisation, Urbanization, Poor, Employment, NGO’s, Government.