District HIV/AIDS Epidemiological Profiles
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

ಕ ೋವಿಡ್ ಲಸಿಕಾಕರಣ ಕ ೋೇಂದ್ರಗಳು (COVID VACCINATION CENTRES) Sl No District CVC Na
ಕ ೋ풿蓍 ಲಕಾಕರಣ ಕ ೋᲂ飍ರಗಳು (COVID VACCINATION CENTRES) Sl No District CVC Name Category 1 Bagalkot SC Karadi Government 2 Bagalkot SC TUMBA Government 3 Bagalkot Kandagal PHC Government 4 Bagalkot SC KADIVALA Government 5 Bagalkot SC JANKANUR Government 6 Bagalkot SC IDDALAGI Government 7 Bagalkot PHC SUTAGUNDAR COVAXIN Government 8 Bagalkot Togunasi PHC Government 9 Bagalkot Galagali Phc Government 10 Bagalkot Dept.of Respiratory Medicine 1 Private 11 Bagalkot PHC BENNUR COVAXIN Government 12 Bagalkot Kakanur PHC Government 13 Bagalkot PHC Halagali Government 14 Bagalkot SC Jagadal Government 15 Bagalkot SC LAYADAGUNDI Government 16 Bagalkot Phc Belagali Government 17 Bagalkot SC GANJIHALA Government 18 Bagalkot Taluk Hospital Bilagi Government 19 Bagalkot PHC Linganur Government 20 Bagalkot TOGUNSHI PHC COVAXIN Government 21 Bagalkot SC KANDAGAL-B Government 22 Bagalkot PHC GALAGALI COVAXIN Government 23 Bagalkot PHC KUNDARGI COVAXIN Government 24 Bagalkot SC Hunnur Government 25 Bagalkot Dhannur PHC Covaxin Government 26 Bagalkot BELUR PHC COVAXINE Government 27 Bagalkot Guledgudd CHC Covaxin Government 28 Bagalkot SC Chikkapadasalagi Government 29 Bagalkot SC BALAKUNDI Government 30 Bagalkot Nagur PHC Government 31 Bagalkot PHC Malali Government 32 Bagalkot SC HALINGALI Government 33 Bagalkot PHC RAMPUR COVAXIN Government 34 Bagalkot PHC Terdal Covaxin Government 35 Bagalkot Chittaragi PHC Government 36 Bagalkot SC HAVARAGI Government 37 Bagalkot Karadi PHC Covaxin Government 38 Bagalkot SC SUTAGUNDAR Government 39 Bagalkot Ilkal GH Government -

After the Deluge
http://www.hinduonnet.com/thehindu/thscrip/print.pl?file=2009110626... Vol:26 Iss:22 URL: http://www.flonnet.com/fl2622/stories/20091106262203000.htm Back NATURAL DISASTER After the deluge VIKHAR AHMED SAYEED & RAVI SHARMA The floods have inundated almost 4,500 villages and destroyed over 500,000 dwellings in Karnataka. SHAILENDRA BHOJAK/PTI AT TALMARI VILLAGE in Raichur district in Karnataka on October 6, when the flood waters had receded. FOR 55-year-old Shankaramma, a marginal farmer of Pattadakal village in Karnataka’s Bagalkot district, the south-west monsoon this year was a big disappointment. Her family’s joint holding of three acres (1.2 hectares) of farm land and its corn and jowar crops were up against the weakest monsoon in 40 years. And the Karnataka government declared 2009 a drought year. But on September 30, what is considered the last day of the monsoon season, Shankaramma’s prayers of the past four months were answered. The skies opened up. However, to her consternation, the rain never seemed to stop. It flooded the entire village, inundating her crops and destroying her house. To make matters worse, the Bennihalla, a nearby rivulet and a tributary of the Malaprabha river, breached its banks at many places. It was unable to discharge its flood waters into the Malaprabha fast enough, which was also in spate by October 2, thanks to a number of encroachments and obstructions. Hundreds of kilometres away, Halvi Veerabhadra Gowda, 46, a resident of T.S. Kudlu village in Siruguppa taluk in Bellary district, became the hero of his village of 550 families. -

Analysis of Micronutrients in Soils from Bagalkot
IOSR Journal of Applied Chemistry (IOSR-JAC) e-ISSN: 2278-5736.Volume 10, Issue 7 Ver. III (July. 2017), PP 33-36 www.iosrjournals.org Analysis of Micronutrients in Soils from Bagalkot *Sumangala Kaladagi1 and Basavaraj M.Kalashetty2 1. Research and Development Center, Bharathiar University. Coimbatore, Tamilnadu. 2. BLDEA’S Science College, Jamkhandi Karnataka, India. Corresponding Author: *Sumangala Kaladagi Abstract: Micronutrients are vital for plant growth and human health. Soil and foliar applications are the most prevalent methods of micronutrient addition but the cost involved and difficulty in obtaining high quality micronutrient fertilizers are major concerns with these in developing countries. Although required in minute quantities however, micronutrients have the same agronomic importance as macronutrients and play vital roles in the growth of plants. The transformation from the fallow and shifting cultivation practices prevalent among farmers to intensive continuous cultivation of soils and the use of improved crop varieties which take up many nutrients from the soil are major causes of deficiency of these micronutrients. A total of 36 composite soil samples were collected at 0-15 and 15-30 cm depths from different taluka, purposively selected representative locations of Badami,Bilagi,Hunagund,Jamakhandi,Mudhol and Bagalkot of Karnataka State, Standard laboratory methods were used to determine the micronutrients of the soil samples. Keywords: Micronutrients, Soil properties, zinc,iron, Copper, manganese, etc. ----------------------------------------------------------------------------------------------------------------------------- -

Land Identified for Afforestation in the Forest Limits of Bagalkot District
Land identified for afforestation in the forest limits of Bagalkot District Kajibilagi Gothe Kalabilagi µ Kurgod Tungal Gadyal Kanoli Krishna Nagar Savalagi Nakur Adihudiahtti Hosa Shurpali Tadalabagi Takkoda Maigur Tupchi Muttur Shiraguppi Chik Jambagi Takkalaki Hire Padsalagi Hosa Janawad Naganur Shurpali Chikkalagi Kadkol Alabal Hosa Kovatgi Kankanawadi Hire Jambagi Algur Chik Padsalagi Hippargi Hosa Muttur Jamakhandi Rahimatpur Kavatgi Kumbarahal Tamadaddi Kunchanur Janwad Kulahalli Bairappana GudiJaknur Chingundi Bidari Asagi Mundaganur Halingali Ramtirth Temple Madalamatti Madrakhandi Terdal Asangi Yellatti Belvalmatti Kolur Hangandi Banhatti Bhandegani Rabkavi Linganur Kalhalli Jamkhandi Jagdal Hunsikatti Bijapur Sa Salhatti Hosur Hulyal Budni Kaltippi Siddapura RABAKAVI BANAHATTI Girgaon Yargatti Rabkavi Chavadapur Badagi Chimod Mareguddi Konnur Gani Galgali Budihal Hanchanala Gulbal Sonna Budni Kulali Yadhalli Girigaon Budni Shirol Bisnal Shivapur Samirwadi Bisnal Mahalinpur Belagali Mantur Amalihari Kontikal Saidapur Mugalkhod Kisuri Teggihal Sanganatti Siddapura Nagaral Malapur Dhavaleshwar Rolli Madbhavi Melligeri Girisagar Sorgaon Siddapura Tanda Badagandi Muttaldinni Bilgi Nagraj Malali Marapur Dhavleshwar Honnihal Mudhol Nandgaon Akkimardi Chenal Halagali Bilagi Mannikeri Vantigod Uttur Jaliber Gulbal Sitimani Mirji Ranjanagi Arakeri Tanda Gulbal Sitimani Tanda ManihalliHosur Badaradinni Chenal Hire Gulbal Tanda Tolmatti Rampur Nagaral Mallapur Rugi Ingalagi Bommanagi Sunaga Tanda Naynegali Jirgal Marakatti Janmatti Sunaga -

District Disaster Management Plan- Udupi
DISTRICT DISASTER MANAGEMENT PLAN- UDUPI UDUPI DISTRICT 2015-16 -1- -2- Executive Summary The District Disaster Management Plan is a key part of an emergency management. It will play a significant role to address the unexpected disasters that occur in the district effectively. The information available in DDMP is valuable in terms of its use during disaster. Based on the history of various disasters that occur in the district, the plan has been so designed as an action plan rather than a resource book. Utmost attention has been paid to make it handy, precise rather than bulky one. This plan has been prepared which is based on the guidelines from the National Institute of Disaster Management (NIDM). While preparing this plan, most of the issues, relevant to crisis management, have been carefully dealt with. During the time of disaster there will be a delay before outside help arrives. At first, self-help is essential and depends on a prepared community which is alert and informed. Efforts have been made to collect and develop this plan to make it more applicable and effective to handle any type of disaster. The DDMP developed touch upon some significant issues like Incident Command System (ICS), In fact, the response mechanism, an important part of the plan is designed with the ICS. It is obvious that the ICS, a good model of crisis management has been included in the response part for the first time. It has been the most significant tool for the response manager to deal with the crisis within the limited period and to make optimum use of the available resources. -

Bidar District “Disaster Management Plan 2015-16” ©Ãzàgà F¯Áè
BIDAR DISTRICT DISASTER MANAGEMENT PLAN-2015-16 Government of Karnataka Bidar District “Disaster Management Plan 2015-16” ©ÃzÀgÀ f¯Áè “““«¥ÀvÀÄÛ“«¥ÀvÀÄÛ ¤ªÀðºÀuÁ AiÉÆÃd£É 20152015----16161616”””” fĒÁè¢üPÁjUÀ¼À PÁAiÀiÁð®AiÀÄ ©ÃzÀgÀ fĒÉè BIDAR DEPUTY COMMISSIONER OFFICE, BIDAR. BIDAR DISTRICT DISASTER MANAGEMENT PLAN-2015-16 CONTENTS SL NO TOPIC PAGE NO 1 Preface 03 2 Glossary 04 3 Chapter-1 :Introduction 05-13 4 Chapter-2 : Bidar District Profile 14-25 5 Chapter-3 : Hazard Risk Vulnerability and Capacity (HRVC) 26-41 Analyses 6 Chapter-4 : Institution Mechanism 42-57 7 Chapter-5: Mitigation Plan 58-73 8 Chapter-6: Response Plan 74-80 9 Chapter-7: Recovery and Reconstruction Plan 81-96 10 Chapter-8 : Resources and Contact Numbers 97-117 11 Chapter-9 : Standard Operating Processor (SOPs) 118-125 12 Chapter-10 : Maps 126-137 13 Conclusion 138 14 Bibliography 139 BIDAR DEPUTY COMMISSIONER OFFICE, BIDAR. Bidar District Disaster Management Pla n 2015-16 Office of the Deputy Commissioner Bidar District, Bidar Shri. Anurag Tewari I. A.S Chairman of Disaster Management & Deputy Commissioner Phone: 08482-225409 (O), 225262(Fax) Bidar District E-mail: [email protected] PREFACE “Disaster” means unforeseen and serious threat to public life with suddenness in terms of time. Declaration of disaster depends on gravity or magnitude of situ ation, number of victims involved, time factor i.e. suddenness of an event, non- availability of medical care in terms of space, equipment’s medical and pa ramedical staff, medicines and other basic human needs like food, shelter and clothing, weather conditions in the locali ty of incident etc., thus enhancing human sufferings and create human needs that the victim cann ot alleviate without assistance. -

Coastal Zone Environmental Management in Udupi District, Karnataka State, India
RESEARCH INVENTY: International Journal of Engineering and Science ISSN: 2278-4721, Vol. 1, Issue 3 (Sept 2012), PP 08-11 www.researchinventy.com Coastal Zone Environmental Management in Udupi District, Karnataka State, India 1. 2 3 Dodda Aswathanarayana Swamy, .Dr.B.E.Basavarajappa, .Prof.E.T.Puttaiah, Research Scholar 1Dept. of PG Studies & Research in Environmental Science, Kuvempu University Shankaraghatta-577451, Karnataka State 2Professor, Department of Chemistry, Bapuji Institute of Engineering and Technology, Davangere, Karnataka State, India 3Professor, Department of Environmental Science, Kuvempu University Shankaraghatta-577451, Karnataka State, India Abstract: The Udupi coastal zone represents varied and highly productive ecosystems such as mangroves, coral reefs and sand dunes. These ecosystems are under pressure on account of increased anthropogenic activities such as discharge of industrial and municipal sewage, land use, tourism, maritime transport, dumping at sea degrade the coast. It is necessary to protect these coastal ecosystems to ensure sustainable development. This requires information on habitats, landforms, coastal processes, water quality, natural hazards on a repetitive basis. The Coastal zone environmental management plan tool is also required for protection of environmental components. I. Introduction. Karnataka’s coast stretches for 320 kilometres along the three districts of Dakshina Kannada, Udupi and Uttara Kannada. Of these, Uttara Kannada has 160-kilometre long coastline while 98 kilometres are in Udupi district and the rest in Dakshina Kannada. It’s three distinct agro-climatic zones range from coastal flatlands in the west with undulating hills and valleys in the middle and high hill ranges in the east that separates it from the peninsula. There is a narrow strip of coastal plains with varying width between the mountain and the Arabian Sea, the average width being about 20 km. -

Synchronized Population Estimation of the Asian Elephant in Forest Divisions of Karnataka -2012
Synchronized Population Estimation of the Asian Elephant in Forest Divisions of Karnataka -2012 Final report submitted to Karnataka Forest Department – December 2012 1 Karnataka Forest Department Synchronized Population Estimation of the Asian Elephants in Forest Divisions of Karnataka -2012 Final report submitted to Karnataka Forest Department – December 2012 by Surendra Varma and R. Sukumar With inputs from Mukti Roy, Sujata, S. R., M.S. Nishant, K. G. Avinash and Meghana S. Kulkarni Karnataka Forest 1 Department Suggested Citation: Varma, S. and Sukumar, R. (2012). Synchronized Population Estimation of the Asian Elephant in Forest Divisions of Karnataka -2012; Final report submitted to Karnataka Forest Department – December 2012. Asian Nature Conservation Foundation and Centre for Ecological Sciences, Indian Institute of Science, Bangalore - 560 012, Karnataka. Photo credits: Figures 1a, b, 3a, b, 4a, b, 8a, b, 9a, b, 10a and b: Karnataka Forest Department; Front and back cover: Surendra Varma 1 Contents Background 1 Training programme and population estimation methods 1 Results 1 Sample block count 3 Line transect indirect (dung) count 7 Overall status of elephant and their distribution in Karnataka 9 Population structure (sex and age classification) 11 Salient observations of the 2012 enumeration 11 Summary of recommendations 11 Captive Elephant population 12 Appendix 1: 14 Methods of population estimates and demographic profiling Appendix 2: 19 Exploratory analysis of detection of elephants in blocks of varying sizes Acknowledgements 21 References 21 1 1 Background Karnataka Forest Department, in coordination with neighbouring southern states (Kerala, Tamil Nadu, Andhra Pradesh, Maharashtra and Goa), conducted a synchronized elephant census from 23rd to 25th May 2012 in the state. -

International Research Spatio-Temopral Rain Fall of Hunsur Taluk, Mysore Di International Journal of Trend in Scientific Researc
International Journal of Trend in Scientific Research and Development (IJTSRD) International Open Access Journal ISSN No: 2456 - 6470 | www.ijtsrd.com | Volume - 1 | Issue – 6 Spatio-Temopral Rain Fall Variation ; A Case Study of Western Part of Hunsur Taluk, Mysore District, Karnataka, India Gangadhara G Research scholar, Department of Studies in Geography, Manasagangotri, University of Mysore ABSTRACT The present study has been conducted to assess the agriculture it helps to explaining the various socio- spatial variations in rainfall in Hunsur taluk, economic problems The amount of rainfall does not Karnataka, India. In order to discuss spatial and show an equal distribution, either in space or in time. temporal variations in rainfall, 5 rain gauge stations It varies from heavy rain to scanty in different parts. It have been chosen to collect data for the years 1985 to also has great regional and temporal variations in 2005. Data have been collected mainly from the distribution. Therefore, the study has been conducted District Statistical Office, Mysore. These collected in order to help farmers to for cultivation process data have been used to examine year-wise spatial variations of rainfall using ArcGIS. Co-efficient of STUDY AREA: HUNSUR TALUK, variation has also been computed to assess the area KARNATAKA INDIA. where average rainfall can be expected, in the future. The result shows that, the study area has fluctuations Western part of Hunsur The taluk is bound on the in rainfall and Hyrige raingage station received north by Mysore and part of k r nagar taluk and on the maximum annual rain, Hunsur tobacco research east by H D kote. -
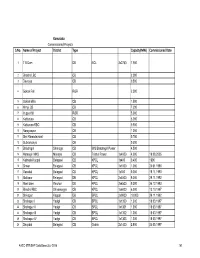
Karnataka Commissioned Projects S.No. Name of Project District Type Capacity(MW) Commissioned Date
Karnataka Commissioned Projects S.No. Name of Project District Type Capacity(MW) Commissioned Date 1 T B Dam DB NCL 3x2750 7.950 2 Bhadra LBC CB 2.000 3 Devraya CB 0.500 4 Gokak Fall ROR 2.500 5 Gokak Mills CB 1.500 6 Himpi CB CB 7.200 7 Iruppu fall ROR 5.000 8 Kattepura CB 5.000 9 Kattepura RBC CB 0.500 10 Narayanpur CB 1.200 11 Shri Ramadevaral CB 0.750 12 Subramanya CB 0.500 13 Bhadragiri Shimoga CB M/S Bhadragiri Power 4.500 14 Hemagiri MHS Mandya CB Trishul Power 1x4000 4.000 19.08.2005 15 Kalmala-Koppal Belagavi CB KPCL 1x400 0.400 1990 16 Sirwar Belagavi CB KPCL 1x1000 1.000 24.01.1990 17 Ganekal Belagavi CB KPCL 1x350 0.350 19.11.1993 18 Mallapur Belagavi DB KPCL 2x4500 9.000 29.11.1992 19 Mani dam Raichur DB KPCL 2x4500 9.000 24.12.1993 20 Bhadra RBC Shivamogga CB KPCL 1x6000 6.000 13.10.1997 21 Shivapur Koppal DB BPCL 2x9000 18.000 29.11.1992 22 Shahapur I Yadgir CB BPCL 1x1300 1.300 18.03.1997 23 Shahapur II Yadgir CB BPCL 1x1301 1.300 18.03.1997 24 Shahapur III Yadgir CB BPCL 1x1302 1.300 18.03.1997 25 Shahapur IV Yadgir CB BPCL 1x1303 1.300 18.03.1997 26 Dhupdal Belagavi CB Gokak 2x1400 2.800 04.05.1997 AHEC-IITR/SHP Data Base/July 2016 141 S.No. Name of Project District Type Capacity(MW) Commissioned Date 27 Anwari Shivamogga CB Dandeli Steel 2x750 1.500 04.05.1997 28 Chunchankatte Mysore ROR Graphite India 2x9000 18.000 13.10.1997 Karnataka State 29 Elaneer ROR Council for Science and 1x200 0.200 01.01.2005 Technology 30 Attihalla Mandya CB Yuken 1x350 0.350 03.07.1998 31 Shiva Mandya CB Cauvery 1x3000 3.000 10.09.1998 -

Franchisees in the State of Karnataka (Other Than Bangalore)
Franchisees in the State of Karnataka (other than Bangalore) Sl. Place Location Franchisee Name Address Tel. No. No. Renuka Travel Agency, Opp 1 Arsikere KEB Office K Sriram Prasad 9844174172 KEB, NH 206, Arsikere Shabari Tours & Travels, Shop Attavara 2 K.M.C M S Shabareesh No. 05, Zephyr Heights, Attavar, 9964379628 (Mangaluru) Mangaluru-01 No 17, Ramesh Complex, Near Near Municipal 3 Bagepalli S B Sathish Municipal Office, Ward No 23, 9902655022 Office Bagepalli-561207 New Nataraj Studio, Near Private Near Private Bus 9448657259, 4 Balehonnur B S Nataraj Bus Stand, Iliyas Comlex, Stand 9448940215 Balehonnur S/O U.N.Ganiga, Barkur 5 Barkur Srikanth Ganiga Somanatheshwara Bakery, Main 9845185789 (Coondapur) Road, Barkur LIC policy holders service center, Satyanarayana complex 6 Bantwal Vamanapadavu Ramesh B 9448151073 Main Road,Vamanapadavu, Bantwal Taluk Cell fix Gayathri Complex, 7 Bellare (Sulya) Kelaginapete Haneef K M 9844840707 Kelaginapete, Bellare, Sulya Tq. Udayavani News Agent, 8 Belthangady Belthangady P.S. Ashok Shop.No. 2, Belthangady Bus 08256-232030 Stand, Belthangady S/O G.G. Bhat, Prabhath 9 Belthangady Belthangady Arun Kumar 9844666663 Compound, Belthangady 08282 262277, Stall No.9, KSRTC Bus Stand, 10 Bhadravathi KSRTC Bus Stand B. Sharadamma 9900165668, Bhadravathi 9449163653 Sai Charan Enterprises, Paper 08282-262936, 11 Bhadravathi Paper Town B S Shivakumar Town, Bhadravathi 9880262682 0820-2562805, Patil Tours & Travels, Sridevi 2562505, 12 Bramhavara Bhramavara Mohandas Patil Sabha bhavan Building, N.H. 17, 9845132769, Bramhavara, Udupi Dist 9845406621 Ideal Enterprises, Shop No 4, Sheik Mohammed 57A, Afsari Compound, NH 66, 8762264779, 13 Bramhavara Dhramavara Sheraj Opposite Dharmavara 9945924779 Auditorium Brahmavara-576213 M/S G.R Tours & Travels, 14 Byndur Byndoor Prashanth Pawskar Building, N.H-17, 9448334726 Byndoor Sl. -

Karnataka: State Geology and Mineral Maps – Geological Survey of India
GOVERNMENT OF INDIA GEOLOGICAL SURVEY OF INDIA MISCELLANEOUS PUBLICATION NO. 30 GEOLOGY AND MINERAL RESOURCES OF THE STATES OF INDIA PART VII – Karnataka & Goa Compiled By GeologicalOPERATION :Survey Karnataka & Goa of India Bangalore 2006 CONTENTS Page No. Section-1: Geology and Mineral Resources of Karnataka I. Introduction 1 II. Physiography 1 III. Geology 2 Sargur Group 5 Peninsular Gneissic Complex and Charnockite 5 Greenstone belts 7 Closepet Granite 10 Mafic-ultramafic complexes 11 Dyke Rocks 12 Proterozoic (Purana) Basins 12 Deccan Trap 13 Warkali Beds 13 Laterite 13 Quaternary Formations 14 Recent alluvial soil and rich alluvium 14 IV. Structure 14 Folds 15 Shear zones, Faults and Lineaments 15 V. Mineral Resources Antimony 16 Asbestos 17 Barytes 17 Basemetals (Cu, Pb, Zn) 18 Bauxite 18 Chromite 21 Clay 22 Corundum 23 Diamond 24 Dolomite 25 Feldspar 25 GeologicalFuller's Earth Survey of India25 Garnet 26 Gemstones 26 Gold 28 Graphite 33 Gypsum 33 Iron Ore 33 Kyanite and sillimanite 35 ii Limestone 35 Lithium 37 Magnesite 38 Manganese ores 38 Molybdenite 40 Nickel 40 Ochre 40 Ornamental stones and dimension stones 41 Felsite, fuchsite quartzite 43 Phosphorite 43 Platinoids 43 Quartz 44 Silica sand 44 Radioactive and Rare Earth Minerals 45 Steatite (Soap stone) 45 Tin 46 Titaniferous & vanadiferous magnetite 46 Tungsten 47 Vermiculite 47 Section 2 Geology and Mineral Resources of Goa I. Introduction 48 II. Physiography 48 III. Geology 49 IV. Mineral Resources 51 Bauxite 51 Chromite 52 Clay 52 Iron Ore 52 Limestone 53 Manganese