Clomethiazole/Cloral Hydrate
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Title 16. Crimes and Offenses Chapter 13. Controlled Substances Article 1
TITLE 16. CRIMES AND OFFENSES CHAPTER 13. CONTROLLED SUBSTANCES ARTICLE 1. GENERAL PROVISIONS § 16-13-1. Drug related objects (a) As used in this Code section, the term: (1) "Controlled substance" shall have the same meaning as defined in Article 2 of this chapter, relating to controlled substances. For the purposes of this Code section, the term "controlled substance" shall include marijuana as defined by paragraph (16) of Code Section 16-13-21. (2) "Dangerous drug" shall have the same meaning as defined in Article 3 of this chapter, relating to dangerous drugs. (3) "Drug related object" means any machine, instrument, tool, equipment, contrivance, or device which an average person would reasonably conclude is intended to be used for one or more of the following purposes: (A) To introduce into the human body any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (B) To enhance the effect on the human body of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (C) To conceal any quantity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; or (D) To test the strength, effectiveness, or purity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state. (4) "Knowingly" means having general knowledge that a machine, instrument, tool, item of equipment, contrivance, or device is a drug related object or having reasonable grounds to believe that any such object is or may, to an average person, appear to be a drug related object. -

Clinical Trial of the Neuroprotectant Clomethiazole in Coronary Artery Bypass Graft Surgery a Randomized Controlled Trial Robert S
Anesthesiology 2002; 97:585–91 © 2002 American Society of Anesthesiologists, Inc. Lippincott Williams & Wilkins, Inc. Clinical Trial of the Neuroprotectant Clomethiazole in Coronary Artery Bypass Graft Surgery A Randomized Controlled Trial Robert S. Kong, F.R.C.A.,* John Butterworth, M.D.,† Wynne Aveling, F.R.C.A.,‡ David A. Stump, M.D.,† Michael J. G. Harrison, F.R.C.P.,§ John Hammon, M.D.,ʈ Jan Stygall, M.Sc.,# Kashemi D. Rorie, Ph.D.,** Stanton P. Newman, D.Phil.†† Background: The neuroprotective property of clomethiazole THE efficacy of coronary artery bypass surgery in the has been demonstrated in several animal models of global and relief of angina and in some circumstances in enhancing Downloaded from http://pubs.asahq.org/anesthesiology/article-pdf/97/3/585/335909/0000542-200209000-00011.pdf by guest on 29 September 2021 focal brain ischemia. In this study the authors investigated the life expectation is now accepted. It is a tribute to the low effect of clomethiazole on cerebral outcome in patients under- mortality of the procedure that interest is now focused going coronary artery bypass surgery. Methods: Two hundred forty-five patients scheduled for on the neurologic and neuropsychological complica- 1–3 coronary artery bypass surgery were recruited at two centers tions. Adverse neurologic outcomes have been found and prospectively randomized to clomethiazole edisilate to occur in 2–6% of patients and neuropsychological (0.8%), 225 ml (1.8 mg) loading dose followed by a maintenance deficits in 10–30%.4–6 These complications are consid- dose of 100 ml/h (0.8 mg/h) during surgery, or 0.9% NaCl ered to be ischemic in nature, being a consequence of (placebo) in a double-blind trial. -
A Retrospective Comparison of Inappropriate Prescribing Of
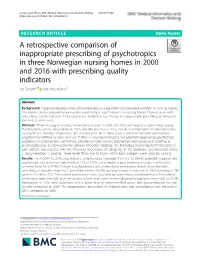
Schjøtt and Aßmus BMC Medical Informatics and Decision Making (2019) 19:102 https://doi.org/10.1186/s12911-019-0821-0 RESEARCHARTICLE Open Access A retrospective comparison of inappropriate prescribing of psychotropics in three Norwegian nursing homes in 2000 and 2016 with prescribing quality indicators Jan Schjøtt1,2* and Jörg Aßmus3 Abstract Background: Inappropriate prescribing of psychotropics is a persistent and prevalent problem in nursing homes. The present study compared inappropriate prescribing of psychotropics in nursing homes 16 years apart with prescribing quality indicators. The purpose was to identify any change in inappropriate prescribing of relevance for medical informatics. Methods: Three Norwegian nursing homes were audited in 2000 and 2016 with regard to prescribing quality. Psychotropics among 386 patients in 2000, and 416 patients in 2016, included combinations of antidepressants, antipsychotics, anxiolytics-hypnotics, and antiepileptics. Prescribing quality indicators included psychotropic polypharmacy (defined as concurrent use of three or more psychotropics) and potential inappropriate psychotropic substances or combinations. Furthermore, potential clinically relevant psychotropic interactions were classified as pharmacodynamic or pharmacokinetic using an interaction database. The first ranked (most important) interaction in each patient was selected with the following importance of categories in the database; recommended action > documentation > severity. Three levels (from low to high) within each category were used for ranking. Results: From 2000 to 2016, psychotropic polypharmacy increased from 6.2 to 29.6%, potential inappropriate psychotropic substances was reduced from 17.9 to 11.3% and potential inappropriate psychotropic combinations increased from 7.8 to 27.9%. Changes in polypharmacy and combinations were predominantly associated with prescribing of anxiolytics-hypnotics. -

Pharmacological Treatments in Insomnia
Pharmacological treatments in insomnia Sue Wilson Centre for Neuropsychopharmacology, Division of Brain Sciences, Imperial College, London Drugs used in insomnia Licensed for insomnia •GABA-A positive allosteric modulators •melatonin (modified release) •promethazine •diphenhydramine •doxepin (USA) Unlicensed prescribed frequently •antihistamines (and OTC) •antidepressants Sometimes prescribed drugs for psychosis Some GABA-A positive allosteric modulators Drugs acting at the GABA-A benzodiazepine receptor zopiclone zolpidem zaleplon benzodiazepines eg temazepam, lorazepam (safe in overdose, as long as no other drug involved) Drugs acting at the barbiturate/alcohol receptor chloral hydrate/chloral betaine clomethiazole (dangerous in overdose) GABA calms the brain Gamma aminobutyic acid (GABA) is the main inhibitory transmitter in the mammalian central nervous system. It plays the principal role in reducing neuronal excitability and its receptors are prolific throughout the brain, in cortex, limbic system, thalamus and cerebellum sedative Increase anticonvulsant GABA anxiolytic function ataxia, memory effects Effects of GABA-A positive allosteric modulators •These drugs enhance the effect of GABA, the main inhibitory neurotransmitter in the brain •They all produce sedation, sleep promotion, ataxia, muscle relaxation, effects on memory, anticonvulsant effects •Therefore for insomnia the duration of action of the drug is important – these effects are unwanted during the day Effects of these GABA-ergic drugs on sleep EEG/PSG • Appearance of -

Boendedok 2020 Manual För Intervjuformulären
BoendeDOK 2020 Manual för intervjuformulären Mikael Dahlberg Mats Anderberg Helen Falck Innehållsförteckning Introduktion ___________________________________________________ 4 BoendeDOK __________________________________________________ 6 Inskrivningsintervju __________________________________________ 6 Avstämningsintervju __________________________________________ 7 Utskrivningsintervju __________________________________________ 7 Frågeområden i BoendeDOK ___________________________________ 7 Hantering och förvaring av DOK-material _________________________ 8 Kontaktpersonens roll _________________________________________ 8 Kodning i BoendeDOK ________________________________________ 9 Tidsintervaller ______________________________________________ 10 Frågor om förändring ________________________________________ 10 Att i efterhand ändra intervjusvar _______________________________ 11 Inför intervjun - Klientens samtycke ____________________________ 11 Under intervjun _____________________________________________ 12 Återkoppling av Inskrivningsintervjun ___________________________ 12 BoendeDOK Inskrivningsformulär ________________________________ 16 Intervjuinformation __________________________________________ 16 A. Administrativa uppgifter ___________________________________ 16 B. Bakgrundsinformation _____________________________________ 17 C. Boende _________________________________________________ 17 D. Relationer _______________________________________________ 20 E. Myndighets- och vårdkontakter ______________________________ 21 -

124.210 Schedule IV — Substances Included. 1
1 CONTROLLED SUBSTANCES, §124.210 124.210 Schedule IV — substances included. 1. Schedule IV shall consist of the drugs and other substances, by whatever official name, common or usual name, chemical name, or brand name designated, listed in this section. 2. Narcotic drugs. Unless specifically excepted or unless listed in another schedule, any material, compound, mixture, or preparation containing any of the following narcotic drugs, or their salts calculated as the free anhydrous base or alkaloid, in limited quantities as set forth below: a. Not more than one milligram of difenoxin and not less than twenty-five micrograms of atropine sulfate per dosage unit. b. Dextropropoxyphene (alpha-(+)-4-dimethylamino-1,2-diphenyl-3-methyl-2- propionoxybutane). c. 2-[(dimethylamino)methyl]-1-(3-methoxyphenyl)cyclohexanol, its salts, optical and geometric isomers and salts of these isomers (including tramadol). 3. Depressants. Unless specifically excepted or unless listed in another schedule, any material, compound, mixture, or preparation which contains any quantity of the following substances, including its salts, isomers, and salts of isomers whenever the existence of such salts, isomers, and salts of isomers is possible within the specific chemical designation: a. Alprazolam. b. Barbital. c. Bromazepam. d. Camazepam. e. Carisoprodol. f. Chloral betaine. g. Chloral hydrate. h. Chlordiazepoxide. i. Clobazam. j. Clonazepam. k. Clorazepate. l. Clotiazepam. m. Cloxazolam. n. Delorazepam. o. Diazepam. p. Dichloralphenazone. q. Estazolam. r. Ethchlorvynol. s. Ethinamate. t. Ethyl Loflazepate. u. Fludiazepam. v. Flunitrazepam. w. Flurazepam. x. Halazepam. y. Haloxazolam. z. Ketazolam. aa. Loprazolam. ab. Lorazepam. ac. Lormetazepam. ad. Mebutamate. ae. Medazepam. af. Meprobamate. ag. Methohexital. ah. Methylphenobarbital (mephobarbital). -

Assessment Report
12 October 2017 EMA/833636/2017 Committee for Medicinal Products for Human Use (CHMP) Assessment report Referral under Article 29(4) of Directive 2001/83/EC Alcover (granules in sachet) and associated names INN: Sodium oxybate Procedure number: EMEA/H/A-29(4)/1451 Note: Assessment report as adopted by the CHMP with all information of a commercially confidential nature deleted. 30 Churchill Place ● Canary Wharf ● London E14 5EU ● United Kingdom Telephone +44 (0)20 3660 6000 Facsimile +44 (0)20 3660 5555 Send a question via our website www.ema.europa.eu/contact An agency of the European Union © European Medicines Agency, 2018. Reproduction is authorised provided the source is acknowledged. Table of contents 1. Background Information ......................................................................... 3 2. Scientific discussion ................................................................................ 3 2.1. Introduction ...................................................................................................... 3 2.2. Assessment of the issues raised as a potential serious risk to public health............... 4 3. Benefit-risk assessment ........................................................................ 11 3.1. 3.1 Initial benefit-risk balance assessment ......................................................... 11 3.2. 3.2 Re-examination procedure .......................................................................... 13 3.2.1. CHMP discussion on grounds for re-examination ................................................. -
Uniform Classification Guidelines for Foreign Substances and Recommended Penalties Model Rule
DRUG TESTING STANDARDS AND PRACTICES PROGRAM. Uniform Classification Guidelines for Foreign Substances And Recommended Penalties Model Rule. January, 2018 (V.13.4) Ó ASSOCIATION OF RACING COMMISSIONERS INTERNATIONAL – 2018. Association of Racing Commissioners International 1510 Newtown Pike, Lexington, Kentucky, United States www.arci.com Page 1 of 61 Preamble to the Uniform Classification Guidelines of Foreign Substances The Preamble to the Uniform Classification Guidelines was approved by the RCI Drug Testing and Quality Assurance Program Committee (now the Drug Testing Standards and Practices Program Committee) on August 26, 1991. Minor revisions to the Preamble were made by the Drug Classification subcommittee (now the Veterinary Pharmacologists Subcommittee) on September 3, 1991. "The Uniform Classification Guidelines printed on the following pages are intended to assist stewards, hearing officers and racing commissioners in evaluating the seriousness of alleged violations of medication and prohibited substance rules in racing jurisdictions. Practicing equine veterinarians, state veterinarians, and equine pharmacologists are available and should be consulted to explain the pharmacological effects of the drugs listed in each class prior to any decisions with respect to penalities to be imposed. The ranking of drugs is based on their pharmacology, their ability to influence the outcome of a race, whether or not they have legitimate therapeutic uses in the racing horse, or other evidence that they may be used improperly. These classes of drugs are intended only as guidelines and should be employed only to assist persons adjudicating facts and opinions in understanding the seriousness of the alleged offenses. The facts of each case are always different and there may be mitigating circumstances which should always be considered. -

Förordning Om Ändring I Förordningen (1992:1554) Om Kontroll Av Narkotika;
Príloha 11 k rozhodnutiu švédskych úradov vlády 22. februára 2018 § 79 1. ------IND- 2018 0079 S-- SK- ------ 20180302 --- --- PROJET Zbierka zákonov Švédska SFS Published on issued on 1 March 2018. The government hereby lays down1 that Annex 1 to the Ordinance (1992:1554) on the control of narcotic drugs2 shall read as set out below. This ordinance shall enter into force on 10 April 2018. On behalf of the Government ANNIKA STRANDHÄLL Lars Hedengran (Ministry of Health and Social Affairs) 1 See Directive (EU) 2015/1535 of the European Parliament and of the Council of 9 September 2015 laying down a procedure for the provision of information in the field of technical regulations and of rules on Information Society services. 2 Ordinance reprinted as 1993:784. 1 SFS Annex 13 List of substances to be considered narcotic drugs according to the Narcotic Drugs Punishments Act Stimulants of the central nervous system ethylamphetamine (2-ethylamino-1-phenylpropane) fenethylline [1-phenyl-1-piperidyl-(2)-methyl]acetate 1-phenyl-2-butylamine N-hydroxyamphetamine propylhexedrine 4-methylthioamphetamine (4-MTA) modafinil 4-methoxy-N-methylamphetamine (PMMA, 4-MMA) 2,5-dimethoxy-4-ethylthiophenethylamine (2C-T-2) 2,5-dimethoxy-4-(n)-propylthiophenethylamine (2C-T-7) 4-iodo-2,5-dimethoxyphenethylamine (2C-I) 2,4,5-trimethoxyamphetamine (TMA-2) 4-methylmethcathinone (mephedrone) 4-fluoramphetamine 1-(4-methoxyphenyl)-2-(methylamino)propan-1-one (methedrone) 1-(1,3-benzodioxol-5-yl)-2-pyrrolidin-1-yl-pentan-1-one (MDPV) 1-(1,3-benzodioxol-5-yl)-2-(methylamino)butan-1-one -

Drug and Medication Classification Schedule
KENTUCKY HORSE RACING COMMISSION UNIFORM DRUG, MEDICATION, AND SUBSTANCE CLASSIFICATION SCHEDULE KHRC 8-020-1 (11/2018) Class A drugs, medications, and substances are those (1) that have the highest potential to influence performance in the equine athlete, regardless of their approval by the United States Food and Drug Administration, or (2) that lack approval by the United States Food and Drug Administration but have pharmacologic effects similar to certain Class B drugs, medications, or substances that are approved by the United States Food and Drug Administration. Acecarbromal Bolasterone Cimaterol Divalproex Fluanisone Acetophenazine Boldione Citalopram Dixyrazine Fludiazepam Adinazolam Brimondine Cllibucaine Donepezil Flunitrazepam Alcuronium Bromazepam Clobazam Dopamine Fluopromazine Alfentanil Bromfenac Clocapramine Doxacurium Fluoresone Almotriptan Bromisovalum Clomethiazole Doxapram Fluoxetine Alphaprodine Bromocriptine Clomipramine Doxazosin Flupenthixol Alpidem Bromperidol Clonazepam Doxefazepam Flupirtine Alprazolam Brotizolam Clorazepate Doxepin Flurazepam Alprenolol Bufexamac Clormecaine Droperidol Fluspirilene Althesin Bupivacaine Clostebol Duloxetine Flutoprazepam Aminorex Buprenorphine Clothiapine Eletriptan Fluvoxamine Amisulpride Buspirone Clotiazepam Enalapril Formebolone Amitriptyline Bupropion Cloxazolam Enciprazine Fosinopril Amobarbital Butabartital Clozapine Endorphins Furzabol Amoxapine Butacaine Cobratoxin Enkephalins Galantamine Amperozide Butalbital Cocaine Ephedrine Gallamine Amphetamine Butanilicaine Codeine -

Tert-Butanol)
EPA/635/R-13/107 Preliminary Materials www.epa.gov/iris Preliminary Materials for the Integrated Risk Information System (IRIS) Toxicological Review of tert-Butyl Alcohol (tert-Butanol) [CASRN 75-65-0] July 2013 NOTICE This document is comprised of preliminary materials, consisting of a literature search strategy, evidence tables, and exposure-response arrays. This information is distributed solely for the purpose of pre-dissemination review under applicable information quality guidelines. It has not been formally disseminated by EPA. It does not represent and should not be construed to represent any Agency determination or policy. It is being circulated for review of its technical accuracy and science policy implications. National Center for Environmental Assessment Office of Research and Development U.S. Environmental Protection Agency Washington, DC Preliminary Materials for the IRIS Toxicological Review of tert-Butanol DISCLAIMER This document is comprised of preliminary materials for review purposes only. This information is distributed solely for the purpose of pre-dissemination review under applicable information quality guidelines. It has not been formally disseminated by EPA. It does not represent and should not be construed to represent any Agency determination or policy. Mention of trade names or commercial products does not constitute endorsement or recommendation for use. This document is a draft for review purposes only and does not constitute Agency policy. ii DRAFT—DO NOT CITE OR QUOTE Preliminary Materials for the IRIS Toxicological Review of tert-Butanol CONTENTS PREFACE ........................................................................................................................................................ v 1. DRAFT LITERATURE SEARCH STRATEGY .............................................................................................. 1-1 1.1. Literature Search and Screening Strategy for tert-Butanol .......................................................... 1-1 1.2. -

2015R3015 1 Senate Bill No. 458 2
2015R3015 1 Senate Bill No. 458 2 (By Senators Stollings and Kessler) 3 ____________ 4 [Introduced February 11, 2015; referred to the Committee on Health and Human Resources; and 5 then to the Committee on the Judiciary.] 6 ____________ 7 8 9 10 A BILL to amend and reenact §60A-2-210 and §60A-2-212 of the Code of West Virginia, 1931, as 11 amended; and to amend and reenact §60A-10-2, §60A-10-4 and §60A-10-7 of said code, all 12 relating to controlling methamphetamine; requiring prescription to dispense drug products 13 that contain active ingredient ephedrine, pseudoephedrine, phenylpropanolamine and other 14 precursors of methamphetamine; moving certain drug products from Schedule V to Schedule 15 IV; providing exception for drug products that cannot be feasibly converted into 16 methamphetamine; defining terms; prohibiting pharmacies from selling certain drugs that can 17 be used in production of methamphetamine without a prescription; creating criminal offense 18 for possession of certain substances without a prescription with intent to transfer to another 19 to make methamphetamine; removing outdated language; providing criminal penalties; and 20 providing rule-making authority. 21 Be it enacted by the Legislature of West Virginia: 1 2015R3015 1 That §60A-2-210 and §60A-2-212 of the Code of West Virginia, 1931, as amended, be 2 amended and reenacted; and that §60A-10-2, §60A-10-4 and §60A-10-7 of said code be amended 3 and reenacted, all to read as follows: 4 ARTICLE 2. STANDARDS AND SCHEDULES. 5 §60A-2-210. Schedule IV.