How to Use a Metered Dose Inhaler (MDI)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Spirometry Protocol and Software Training Handout
SPIROMETRY PROTOCOL AND SOFTWARE TRAINING HANDOUT Spirometry Protocol Key Points in Performing Spirometry ▪ Always demonstrate the maneuver ▪ Prompt the participant to BLAST out the air ▪ Continue by having the participant PUSH out the air ▪ Continue until the balloon bursts or at least six seconds Getting ready to do Spirometry Subjects will be instructed to not use any bronchodilator medicines for at least 4 hours prior to the appointment (in the case of salmeterol [Serevent] or Fomoterol (foradil)or Tritoprium (Spiriva) avoid for 12 hours prior to the test). Bronchodilator medicines include: Short acting bronchodilators Albuterol (ventolin, proventil, airet, volmax tablet) Levalbuterol (xopenex) Metaproterenol (alupent) Pirbuterol (maxair) Terbutaline (brethaire, brethine, bricanyl) Isoetharine (bronkosol) Ipratropium (atrovent) Ipratropium and albuterol combination (Combivent) Isoproteranol (isuprel) Primatine 1 CHW Educational Protocols – Spirometry Protocol and Software Training Handout Bitolterol (tornalate) Long acting bronchodilator Salmeterol (serevent) Fomoterol (foradil) Tritoprium (Spiriva) Bronchodilators should be avoided because they can affect the spirometry results. If the patient is having symptoms from asthma and needs to use the medicine, ask that the medicine be used 4 hours before the visit, so that the next dose is due during the visit. Patients can then do the spirometry and then the patient can take the medicine after the test is completed. When scheduling the follow-up spirometry visit, if at all possible, try to make the visit at the same time as the initial baseline visit. 1. Preparing the Computer 1. Check to see if the time and date on the lower right hand corner is current. If the date and time is NOT, the spirometer will NOT sync with the computer or the Easy One software. -

Comparison of Intramuscular Betamethasone and Oral
Color profile: Disabled Composite Default screen 100 ORIGINAL ARTICLE 100 95 95 75 75 25 25 5 5 0 Comparison of intramuscular 0 betamethasone and oral prednisone in the prevention of relapse of acute asthma John S Chan MD1, Robert L Cowie MD1, Gerald C Lazarenko MD2, Cinde Little RRT1, Sandra Scott RRT1, Gordon T Ford MD FCCP1 1Division of Respiratory Medicine and 2Department of Emergency Medicine, University of Calgary, Calgary, Alberta JS Chan, RL Cowie, GC Lazarenko, C Little, S Scott, tively) and use of inhaled corticosteroids (46% versus 64.3% GT Ford. Comparison of intramuscular betamethasone respectively) (P<0.05). Using intention-to-treat analysis, the and oral prednisone in the prevention of relapse of acute relapse rates for betamethasone and prednisone at day 7 were asthma. Can Respir J 2001;8(3):147-152. 14.9% (13 of 87 patients) and 25% (21 of 84 patients), respectively (P=0.1), and at day 21, the rates were 36.8% (32 OBJECTIVE: To compare the relapse rate after a single intra- of 87 patients) and 31% (26 of 84 patients), respectively muscular injection of a long acting corticosteroid, betametha- (P=0.4). There were no differences in symptom score, peak sone, with oral prednisone in patients discharged from the flows and adverse effects between the two groups at days 7 emergency department (ED) for acute exacerbations of and 21. asthma. CONCLUSIONS: A single dose of intramuscular betametha- PATIENTS AND METHODS: Patients with acute exacer- sone 12 mg was safe and as efficacious as prednisone in pre- bations of asthma who were suitable for discharge from the venting the relapse of acute asthma. -

Long-Term Budesonide Or Nedocromil Mineral Accretion Over a Period of Years
term inhaled corticosteroid (ICS) treatment on bone Long-term Budesonide or Nedocromil mineral accretion over a period of years. Treatment, Once Discontinued, Does Not Alter the Course of Mild to Moderate Asthma in STUDY POPULATION. Cohort follow-up study for a median Children and Adolescents of 7 years with 877 children 5 to 12 years of age who Strunk RC, Sternberg AL, Szefler SJ, et al. J Pediatr. had mild-to-moderate asthma and initially were ran- 2009;154(5):682–687 domly assigned in the Childhood Asthma Management Program. PURPOSE OF THE STUDY. To determine whether long-term, METHODS. Serial dual-energy x-ray absorptiometry scans continuous use of inhaled antiinflammatory medications of the lumbar spine to assess bone mineral density were affects asthma outcomes in children with mild-to-mod- performed for all patients. Annual bone mineral accre- erate asthma after use is discontinued. tion was calculated for 531 boys and 346 girls. STUDY POPULATION. A total of 941 children, 5 to 12 years of RESULTS. Oral corticosteroid bursts produced dose- age, who had previously participated in the Childhood dependent reductions in bone mineral accretion (0.052, Asthma Management Program (CAMP). 0.049, and 0.046 g/cm2 per year with 0, 1–4, and Ն5 courses, respectively) and increases in the risk for osteo- METHODS. During the CAMP trial, subjects received treat- penia (10%, 14%, and 21%, respectively) in boys but ment with budesonide, nedocromil, or placebo for 4.3 not girls. Cumulative ICS use was associated with a small years. During the posttrial period, asthma manage- decrease in bone mineral accretion in boys but not girls ment was provided by primary care physicians ac- but no increased risk for osteopenia. -

Us Anti-Doping Agency
2019U.S. ANTI-DOPING AGENCY WALLET CARDEXAMPLES OF PROHIBITED AND PERMITTED SUBSTANCES AND METHODS Effective Jan. 1 – Dec. 31, 2019 CATEGORIES OF SUBSTANCES PROHIBITED AT ALL TIMES (IN AND OUT-OF-COMPETITION) • Non-Approved Substances: investigational drugs and pharmaceuticals with no approval by a governmental regulatory health authority for human therapeutic use. • Anabolic Agents: androstenediol, androstenedione, bolasterone, boldenone, clenbuterol, danazol, desoxymethyltestosterone (madol), dehydrochlormethyltestosterone (DHCMT), Prasterone (dehydroepiandrosterone, DHEA , Intrarosa) and its prohormones, drostanolone, epitestosterone, methasterone, methyl-1-testosterone, methyltestosterone (Covaryx, EEMT, Est Estrogens-methyltest DS, Methitest), nandrolone, oxandrolone, prostanozol, Selective Androgen Receptor Modulators (enobosarm, (ostarine, MK-2866), andarine, LGD-4033, RAD-140). stanozolol, testosterone and its metabolites or isomers (Androgel), THG, tibolone, trenbolone, zeranol, zilpaterol, and similar substances. • Beta-2 Agonists: All selective and non-selective beta-2 agonists, including all optical isomers, are prohibited. Most inhaled beta-2 agonists are prohibited, including arformoterol (Brovana), fenoterol, higenamine (norcoclaurine, Tinospora crispa), indacaterol (Arcapta), levalbuterol (Xopenex), metaproternol (Alupent), orciprenaline, olodaterol (Striverdi), pirbuterol (Maxair), terbutaline (Brethaire), vilanterol (Breo). The only exceptions are albuterol, formoterol, and salmeterol by a metered-dose inhaler when used -

ADD/ADHD: Strattera • Allergy/Anti-Inflammatories
EXAMPLES OF PERMITTED MEDICATIONS - 2015 ADD/ADHD: Strattera Allergy/Anti-Inflammatories: Corticosteroids, including Decadron, Depo-Medrol, Entocort, Solu-Medrol, Prednisone, Prednisolone, and Methylprednisolone Anesthetics: Alcaine, Articadent, Bupivacaine HCI, Chloroprocaine, Citanest Plain Dental, Itch-X, Lidocaine, Marcaine, Mepivacaine HCI, Naropin, Nesacaine, Novacain, Ophthetic, Oraqix, Paracaine, Polocaine, Pontocaine Hydrochloride, PrameGel, Prax, Proparacaine HCI, Ropivacaine, Sarna Ultra, Sensorcaine, Synera, Tetracaine, Tronothane HCI, and Xylocaine Antacids: Calci-Chew, Di-Gel, Gaviscon, Gelusil, Maalox, Mintox Plus, Mylanta, Oyst-Cal 500, Rolaids, and Tums Anti-Anxiety: Alprazolam, Atarax, Ativan, Buspar, Buspirone HCI, Chlordiazepoxide HCI, Clonazepam, Chlorazepate Dipotassium, Diastat, Diazepam, Hydroxyzine, Klonopin, Librium, Lorazepam, Niravam, Tranxene T-tab, Valium, Vistaril, and Xanax Antibiotics: Acetasol HC, Amoxil, Ampicillin, Antiben, Antibiotic-Cort, Antihist, Antituss, Avelox, Ceftazidime, Ceftin, Cefuroxime Axetil, Ceptaz, Cleocin, Cloxapen, Cortane-B Aqueous, Cortic, Cresylate, Debrox, Doryx, EarSol-HC, Fortaz, Gantrisin, Mezlin, Moxifloxacin, Neotic, Otocain, Principen, Tazicef, Tazidime, Trioxin, and Zyvox Anti-Depressants: Adapin, Anafranil, Asendin, Bolvidon, Celexa, Cymbalata, Deprilept, Effexor, Elavil, Lexapro, Luvox, Norpramin, Pamelor, Paxil, Pristiq, Prozac, Savella, Surmontil, Tofranil, Vivactil, Wellbutrin, Zoloft, and Zyban Anti-Diabetics: Actos, Amaryl, Avandia, Glipizide, Glucophage, -

Title 16. Crimes and Offenses Chapter 13. Controlled Substances Article 1
TITLE 16. CRIMES AND OFFENSES CHAPTER 13. CONTROLLED SUBSTANCES ARTICLE 1. GENERAL PROVISIONS § 16-13-1. Drug related objects (a) As used in this Code section, the term: (1) "Controlled substance" shall have the same meaning as defined in Article 2 of this chapter, relating to controlled substances. For the purposes of this Code section, the term "controlled substance" shall include marijuana as defined by paragraph (16) of Code Section 16-13-21. (2) "Dangerous drug" shall have the same meaning as defined in Article 3 of this chapter, relating to dangerous drugs. (3) "Drug related object" means any machine, instrument, tool, equipment, contrivance, or device which an average person would reasonably conclude is intended to be used for one or more of the following purposes: (A) To introduce into the human body any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (B) To enhance the effect on the human body of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; (C) To conceal any quantity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state; or (D) To test the strength, effectiveness, or purity of any dangerous drug or controlled substance under circumstances in violation of the laws of this state. (4) "Knowingly" means having general knowledge that a machine, instrument, tool, item of equipment, contrivance, or device is a drug related object or having reasonable grounds to believe that any such object is or may, to an average person, appear to be a drug related object. -

FDA Briefing Document Pulmonary-Allergy Drugs Advisory Committee Meeting
FDA Briefing Document Pulmonary-Allergy Drugs Advisory Committee Meeting August 31, 2020 sNDA 209482: fluticasone furoate/umeclidinium/vilanterol fixed dose combination to reduce all-cause mortality in patients with chronic obstructive pulmonary disease NDA209482/S-0008 PADAC Clinical and Statistical Briefing Document Fluticasone furoate/umeclidinium/vilanterol fixed dose combination for all-cause mortality DISCLAIMER STATEMENT The attached package contains background information prepared by the Food and Drug Administration (FDA) for the panel members of the advisory committee. The FDA background package often contains assessments and/or conclusions and recommendations written by individual FDA reviewers. Such conclusions and recommendations do not necessarily represent the final position of the individual reviewers, nor do they necessarily represent the final position of the Review Division or Office. We have brought the supplemental New Drug Application (sNDA) 209482, for fluticasone furoate/umeclidinium/vilanterol, as an inhaled fixed dose combination, for the reduction in all-cause mortality in patients with COPD, to this Advisory Committee in order to gain the Committee’s insights and opinions, and the background package may not include all issues relevant to the final regulatory recommendation and instead is intended to focus on issues identified by the Agency for discussion by the advisory committee. The FDA will not issue a final determination on the issues at hand until input from the advisory committee process has been considered -

Protective Effects of Inhaled Ipratropium Bromide on Bronchoconstriction Induced by Adenosine and Methacholine in Asthma
Eur Aesplr J 1992, 5, 56()-665 Protective effects of inhaled ipratropium bromide on bronchoconstriction induced by adenosine and methacholine In asthma N. Crimi, F. Palermo, R. Oliveri, R. Polosa, I. Settinieri, A. Mistretta Protective effects of inhaled ipratropium bromide on bronchoconstriction induced by Istituto di Malattie dell' Apparato adenosine and methacholine in asthma. N. Crimi, F. Palermo, R. Oliveri, R. Po/osa, Respiratorio e Tisiologia, Universita' di Catania, Catania, Italy. I. Seuinier~ A. Mistretta. ABSTRACT: Although adenosine-Induced bronchoconstrictlon is mainly due to Correspondence: N. Crimi mast cell mediator release, vagal reflexes have also been Implicated in this Istituto di Malattie dell' Appara.to response. Respiratorio e Tisiologia We have Investigated the effect of a speciflc muscarlnlc-receptor antagonist, Universita' di Catania ipratroplum bromide, on methacholine- and adenosine-Induced bronchoconstriction Via Passo Gravina 187 In a randomized, placebo-controlled, double-blind study of 12 asthmatic subjects. 95125 Catania Airway response was evaluated as forced expiratory volume in one second (FEV,). Italy Inhaled lpratroplum bromide (40 Jlg), administered 20 mln prior to bronchoprovocation, Increased the provocation dose of Inhaled methacholine and Keywords: Adenosine adenosine required to reduce FEV, by 20% from baseline (PD,.) from 0.11 to 0.79 asthma ipratropium bromide mg (p<O.Ol) and from 0.57 to 1.27 mg (p<0.01), respectively. The mean baseline methacholine FEV, values after administration of lpratroplum bromide were signlfkantly higher than after placebo administration (p<O.OS). However, there was no correlation Received: May 22 1991 between the degree of bronchodllatatlon and dose-ratios for methacholine and Accepted after revision January 7 1992 adenosine. -

Supplementary Materials 07/09/2017
SMART Adolescent manuscript: Supplementary materials 07/09/2017 Supplementary materials Methods Definition and calculation of severe exacerbations The first three studies conducted 10-12, defined severe exacerbations as the need for oral corticosteroid (OCS) and/or hospitalisation/emergency room care due to asthma and/or a decrease in peak expiratory flow (PEF) of ≥30% on two consecutive days compared with the run-in period. In these studies, exacerbations were to be treated with a 10-day OCS course; an exacerbation lasting >10 days was considered a new exacerbation on the 11th day. Based on this experience, the later three studies 13-15 did not include falls in PEF in the exacerbation definition, nor this stipulated OCS treatment time, defining a severe exacerbation as the need for OCS for ≥3 days and/or hospitalisation/emergency room care due to asthma worsening. For the purpose of this analysis, we defined a severe exacerbation as the need for OCS (for ≥3 days 10-12) and/or hospitalisation/emergency room care due to asthma worsening; to align with this definition, data from 3 of the included studies 13-15 were reanalysed to exclude PEF fall from the exacerbation definition. 1 SMART Adolescent manuscript: Supplementary materials 07/09/2017 Literature review to identify any additional studies We conducted a review to identify any additional randomised controlled trials (RCTs) evaluating a combination of inhaled corticosteroids (ICS) and a rapid- acting bronchodilator in a single inhaler for both maintenance and as-needed relief of symptoms -

Core Safety Profile
Core Safety Profile Active substance: Nedocromil Pharmaceutical form(s)/strength: Eye drops: 20 mg/ml, Inhalation vapour: 5 mg/ml, Pressurised inhalation: 2 mg/dose, 2mg/0,1 mg, Nebuliser solution: 10 mg/2 ml, Inhalation powder: 10 mg/dose, Nasal spray: 10 mg/ml P-RMS: CZ/H/PSUR/0016/001 Date of FAR: 09.10.2010 EU Core Safety Profile (CSP) For Nedocromil sodium NB: This CSP is combining safety information from the three existing pharmaceutical forms: Eye drops, Nasal spray and Inhaler. Information that is specific to one form is identified by a subheading. No subheading indicates that information is valid for all pharmaceuticals forms 4.3 Contraindications For eye drops <Product name> eye drops is contraindicated in patients with known hypersensitivity to nedocromil sodium, benzalkonium chloride or other constituents of the formulation. For Nasal spray and Inhaler <Product name> nasal spray or inhaler is contraindicated in patients with known hypersensitivity to any of the constituents. 4.4 Special warnings and precautions for use For eye drops Patients should be advised not to wear soft contact lenses during treatment with <product name> eye drops. Benzalkonium chloride, a constituent of the formulation, may accumulate in soft contact lenses. This preservative, when slowly released, could possibly irritate the cornea. In patients who continue to wear hard or gas permeable contact lenses during <product name> eye drops treatment, the lenses should be taken out of the eye prior to instillation of the drops. They should be inserted again not earlier than 10 minutes after administration, in order to allow an even conjunctival distribution of the solution. -

Drug Class Review Nasal Corticosteroids
Drug Class Review Nasal Corticosteroids Final Report Update 1 June 2008 The Agency for Healthcare Research and Quality has not yet seen or approved this report The purpose of this report is to make available information regarding the comparative effectiveness and safety profiles of different drugs within pharmaceutical classes. Reports are not usage guidelines, nor should they be read as an endorsement of, or recommendation for, any particular drug, use or approach. Oregon Health & Science University does not recommend or endorse any guideline or recommendation developed by users of these reports. Dana Selover, MD Tracy Dana, MLS Colleen Smith, PharmD Kim Peterson, MS Oregon Evidence-based Practice Center Oregon Health & Science University Mark Helfand, MD, MPH, Director Marian McDonagh, PharmD, Principal Investigator, Drug Effectiveness Review Project Copyright © 2008 by Oregon Health & Science University Portland, Oregon 97239. All rights reserved. Final Report Update 1 Drug Effectiveness Review Project TABLE OF CONTENTS INTRODUCTION ..........................................................................................................................5 Scope and Key Questions .......................................................................................................................7 METHODS ....................................................................................................................................9 Literature Search .....................................................................................................................................9 -
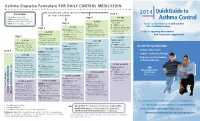
Asthma Control
Asthma Stepwise Formulary FOR DAILY CONTROL MEDICATION QuickGuide to abbreviations: step 6 2014 • ICS: inhaled corticosteroid step 5 • LABA: long-acting beta2-agonist Asthma Control HIGH-DOSE ICS • LTRA: leukotriene receptor antagonist (per step 5) • SABA: short-acting beta2-agonist step 4 LTRA (per step 4) for the care of pediatric and adult patients + LTRA (per step 4) + HIGH-DOSE ICS with established asthma step 3 (mark choice): + oral systemic steroids MEDIUM-DOSE ICS fluticasone (Flovent) MDI: (lowest dose for the shortest (per step 3; mark a choice there) 110 mcg: 2 puffs twice daily duration: 5-10 mg is A tool for ongoing assessment considered low-dose) MEDIUM-DOSE ICS + LTRA: montelukast budesonide (Pulmicort) respules: and treatment adjustment step 2 (mark choice): (Singulair) by mouth: 1.0 mg: 1 respule twice daily 4 mg: 1 tablet once daily, or fluticasone (Flovent) MDI: 1 packet oral granules once daily 110 mcg: 1 puff twice daily HIGH-DOSE ICS budesonide (Pulmicort) respules: (per step 5) LOW-DOSE ICS (mark choice): LABA (per step 3) 0.50 mg: 1 respule twice daily + LABA (per step 4) fluticasone (Flovent) MDI: + HIGH-DOSE ICS LABA (per step 3) Inside the QuickGuide... 44 mcg: 2 puffs twice daily (mark choice): + oral systemic steroids budesonide (Pulmicort) respules: + MEDIUM-DOSE ICS fluticasone (Flovent) MDI: (lowest dose for the shortest 0.25 mg: 1 respule twice daily (mark choice): • Asthma control tables step 1 110 mcg: 2 puffs twice daily duration: 5-10 mg is considered low-dose) fluticasone (Flovent)