Construction of a Molecular Assay for Detection of Drug Resistant Tuberculosis Using Improved Linear-After-The-Exponential PCR
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Population Dynamics
FOCUS ON BACTERIAL GROWTH EDITORIAL Population dynamics This Focus issue on bacterial growth, highlights the versatility and adaptability with which bacterial cells respond to their environmental and community context. Bacteria have an immense capacity to grow. As men- antagonizing each other; for example, by the secretion of tioned by Megan Bergkessel, David Basta and Dianne toxins or through the type VI secretion system. By con- Newman on page 549, if Escherichia coli were to con- trast, mutualistic clonemates growing next to each other tinue exponential growth, a single bacterial “cell would often cooperate; for example, through the secretion of grow to a population with the mass of the Earth within 2 public goods. days”. However, bacteria rarely encounter perfect growth To regulate cooperative behaviour, bacteria use quo- conditions outside of the laboratory: nutrients are lim- rum sensing, whereby the concentrations of secreted sig- ited, the bacteria have to compete with other cells for nalling molecules inform bacteria about the surrounding resources or they are under attack by other bacterial population density. On page 576, Bonnie Bassler and Kai species, host defences or antimicrobial therapy. Thus, Papenfort review quorum sensing systems in Gram- bacteria have developed a wide variety of mechanisms negative bacteria, highlighting the different signalling that enable them to optimize their growth patterns molecules, receptors and response networks. They also according to the surrounding conditions. This Focus describe the broad effects that quorum sensing can have issue explores factors that influence bacterial growth by not only enabling communication between members dynamics and how bacterial populations respond to of one bacterial species but also between species, gen- them; for example, by forming biofilms and produc- era and even kingdoms; for example, between the gut ing a structured extracellular matrix, by executing microbiota and the mammalian host. -

Real-Time Egg Laying Dynamics in Caenorhabditis Elegans
UNIVERSITY OF CALIFORNIA, IRVINE Real-time egg laying dynamics in Caenorhabditis elegans DISSERTATION submitted in partial satisfaction of the requirements for the degree of DOCTOR OF PHILOSOPHY in Biomedical Engineering by Philip Vijay Thomas Dissertation Committee: Professor Elliot Hui, Chair Professor Olivier Cinquin Professor Abraham Lee 2015 c 2015 Philip Vijay Thomas TABLE OF CONTENTS Page LIST OF FIGURES iv ACKNOWLEDGMENTS v CURRICULUM VITAE vi ABSTRACT OF THE DISSERTATION viii 1 Introduction and motivation 1 1.1 The impact of C. elegans in aging and lifespan studies along with current limitations . 1 1.2 Starvation and its effect on worms . 4 1.3 Microfabricated systems for C. elegans biology . 5 2 Real-time C. elegans embryo cytometry to study reproductive aging 7 2.1 High capacity low-weight passive bubble trap . 8 2.2 Microfluidic device layout . 10 2.3 Tuning habitat exit sizes to flush out embryos while retaining worms . 11 2.4 Equal flow resistance to make identical habitats . 12 2.5 Video enumeration of eggs . 13 2.6 Switching between discrete and continuously varying media concentrations . 15 3 Optimizing worm health in C. elegans microfluidics 17 3.1 E. coli densities of 1010 cells/mL maintain egg-laying in liquid worm culture 18 3.2 E. coli biofilms in devices . 19 3.3 Amino acid addition to S-media, γ irradiation of bacteria, and elevated syringe temperatures are ineffective in reducing biofilms in devices . 20 3.4 Use of a curli major subunit deletion strain significantly reduces biofilm in S-media . 23 4 Conclusions and future directions 26 Bibliography 30 ii A Appendix Title 41 A.1 Methods . -

Bacteria Podcast.Pages
podcasts Encyclopedia of Life eol.org Bacteria Podcast and Scientist Interview Bacillus subtilis Roberto Kolter of Harvard explains the relationship between one bacterium, Bacillus subtilis, and the majestic trees outside his office windows at Harvard Medical School. There’s a lot going on, down among the roots. Transcript Ari: From the Encyclopedia of Life, this is One Species at a Time. I’m Ari Daniel Shapiro. Over the last few years, we’ve created more than 60 episodes for this series. But there’s one group we’ve neglected – the bacteria. Kolter: The most spectacular aspect of life on the planet Earth is the stuff we don’t see! Ari: Roberto Kolter is a bacteria fanatic. He’s a microbiologist, after all. Ari: Kolter lifts the blinds of one of his office windows at the Harvard Medical School. He looks outside, and he says everything he sees – depends on bacteria. The people bundled up on the street below rely on the bacteria in their guts to digest their food. There’s the dirt… Kolter: A lot of that soil is actually produced by bacterial activity. Ari: Even the trees dotting the landscape. Kolter: Without the microbes, none of those trees would make it. Ari: And it’s this last point – that most plants really benefit from a remarkable relationship with bacteria – that Kolter’s especially interested in. To explain, let’s focus on a particular bacteria – a tiny rod-shaped cell called Bacillus subtilis. This little guy is everywhere on the planet. Kolter: Glaciers in Alaska, deserts in Africa, swamps in South America – just to mention a few. -
Thesis Submitted for the Degree of Doctor of Philosophy
University of Bath PHD An investigation into the strength and thickness of biofouling deposits to optimise chemical, water and energy use in industrial process cleaning Peck, Oliver Award date: 2017 Awarding institution: University of Bath Link to publication Alternative formats If you require this document in an alternative format, please contact: [email protected] General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ? Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Download date: 07. Oct. 2021 An investigation into the strength and thickness of biofouling deposits to optimise chemical, water and energy use in industrial process cleaning Oliver Philip Wayland Peck A thesis submitted for the degree of Doctor of Philosophy University of Bath Department of Chemical Engineering March 2017 COPYRIGHT Attention is drawn to the fact that copyright of this thesis/portfolio rests with the author and copyright of any previously published materials included may rest with third parties. -

Roberto Kolter Knowing I’M One of the Points,” He Says
CAREERS Dodd chose to shift his research focus elsewhere. “I sometimes found it weird to be in the lab,” he says. He was one of TURNING POINT several patients who had the mutation, yet no symptoms, and so had MRI scans in their lab. “It was weird to see a bar graph, Roberto Kolter knowing I’m one of the points,” he says. The research could be emotionally taxing. “It would feel odd to work on, for example, Roberto Kolter set up his microbiology a mouse with the same genetic mutation laboratory at Harvard Medical School in as me, and wonder if I would respond Boston, Massachusetts, in 1983. Postdocs EINAT SEGEV EINAT similarly,” he says. But he did want to keep worldwide hope to join his lab because of his working on the heart, so he is now a postdoc career-targeted training philosophy, but with studying the cardiac effects of diabetes, a rare exceptions, he brings in only those who disease that his grandfather had. already have a fellowship. SPOTLIGHT SCARS Why do you accept postdocs only if they have The emotional toll can be especially intense their own funding? when media attention forces the scientist I focus on those whom I believe have a fan- into the public eye. Wartman felt the land- tastic chance of getting their own funding as a scape shift after a high-profile piece about principal investigator. I think it’s unfair for me him appeared in the New York Times in 2012. to interview those who have very little chance He is happy that patients find his personal of getting their own funding, considering how perspective helpful, but regrets that the deci- competitive the academic job market is and sion to share his story no longer rests with how important it is to show independence. -

UCLA Electronic Theses and Dissertations
UCLA UCLA Electronic Theses and Dissertations Title Bacterial motility on abiotic surfaces Permalink https://escholarship.org/uc/item/87j0h2w3 Author Gibiansky, Maxsim Publication Date 2013 Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California University of California Los Angeles Bacterial motility on abiotic surfaces A dissertation submitted in partial satisfaction of the requirements for the degree Doctor of Philosophy in Bioengineering by Maxsim L. Gibiansky 2013 c Copyright by Maxsim L. Gibiansky 2013 Abstract of the Dissertation Bacterial motility on abiotic surfaces by Maxsim L. Gibiansky Doctor of Philosophy in Bioengineering University of California, Los Angeles, 2013 Professor Gerard C. L. Wong, Chair Bacterial biofilms are structured microbial communities which are widespread both in nature and in clinical settings. When organized into a biofilm, bacteria are extremely resistant to many forms of stress, including a greatly heightened antibiotic resistance. In the early stages of biofilm formation on an abiotic sur- face, many bacteria make use of their motility to explore the surface, finding areas of high nutrition or other bacteria to form microcolonies. They use motility ap- pendages, including flagella and type IV pili (TFP), to navigate the near-surface environment and to attach to the surface. Bacterial motility has previously been studied on a large scale, describing collective motility modes involving large ag- gregates of cells such as swarming and twitching. This dissertation provides an in-depth look at bacterial motility at the single-cell level, focusing on Pseudomonas aeruginosa and Myxococcus xanthus, two commonly-studied organisms; in addi- tion, it describes particle tracking algorithms and methodology used to analyze single-bacterium behaviors from flow cell microscopy video. -
18.5 N&V Feature Greenbe#822F58
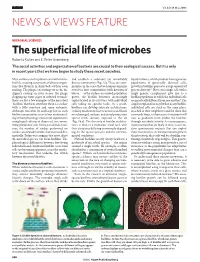
18.5 N&V Feature Greenbe#822F58 12/5/06 6:34 PM Page 300 Vol 441|18 May 2006 NEWS & VIEWS FEATURE MICROBIAL SCIENCES The superficial life of microbes Roberto Kolter and E. Peter Greenberg The social activities and organization of bacteria are crucial to their ecological success. But it is only in recent years that we have begun to study these secret societies. Most surfaces on this planet teem with micro- and establish a sedentary yet remarkably liquid cultures, which produce homogeneous bial life, creating ecosystems of diverse organ- diverse community (Fig. 1a). These are com- populations of genetically identical cells, isms that flourish in slimy beds of their own munities in the sense that we humans organize growth in biofilms generates a large amount of making. The plaque encrusting our teeth, the ourselves into communities with division of genetic diversity 2. How can a single cell, with a slippery coating on river stones, the gunge labour — as the surface-associated population single genetic complement, give rise to a clogging up water pipes or infected wounds: grows, the biofilm becomes increasingly biofilm population in which the individual cells these are just a few examples of the microbial sophisticated in its activities, with individual are genetically different from one another? The ‘biofilms’ that form anywhere there is a surface cells taking on specific tasks. As a result, simplest explanation may be that in any biofilm, with a little moisture and some nutrients. biofilms can develop intricate architectures; individual cells are stuck in the same place, Although microbes by and large live in such striking mushroom-like structures can bloom attached to their neighbours and the slime that biofilm communities, most of our understand- on submerged surfaces, and aerial projections surrounds them, so their access to nutrients will ing of their physiology stems from experiments sprout from surfaces exposed to the air vary as gradients form within the biofilms using liquid cultures of dispersed, free-swim- (Fig. -

An Individual-Based Model for Biofilm Formation at Liquid Surfaces Arxiv
An individual-based model for biofilm formation at liquid surfaces Maxime Ardré+,∗,o, Hervé Henry+, Carine Douarche∗, Mathis Plapp+ + Laboratoire PMC, Ecole Polytechnique CNRS, Palaiseau, France ∗ Laboratoire de Physique des Solides, Université Paris-Sud CNRS, Orsay, France o Laboratoire de Physique Statistique, ENS CNRS, Paris, France May 7, 2018 Abstract The bacterium Bacilus subtilis frequently forms biofilms at the interface between the culture medium and the air. We develop a mathematical model that couples a description of bacteria as individ- ual discrete objects to the standard advection-diffusion equations for the environment. The model takes into account two different bacte- rial phenotypes. In the motile state, bacteria swim and perform a run-and-tumble motion that is biased toward regions of high oxygen concentration (aerotaxis). In the matrix-producer state they excrete extracellular polymers, which allows them to connect to other bacteria and to form a biofilm. Bacteria are also advected by the fluid, and can trigger bioconvection. Numerical simulations of the model reproduce all the stages of biofilm formation observed in laboratory experiments. Finally, we study the influence of various model parameters on the dy- namics and morphology of biofilms. 1 Introduction arXiv:1512.04697v1 [q-bio.CB] 15 Dec 2015 Bacteria are unicellular prokaryotic microorganisms. They are ubiquitous and constitute a large part of the terrestrial biomass. Bacteria can live as individual cells during the planktonic phase. However, most of the time, they are part of self-organized communities of complex architecture adsorbed on interfaces: the biofilms. Besides the bacteria themselves, biofilms are mostly made of an extracellular matrix composed of macromolecules [1, 2, 3] that are produced by the bacteria and lead to cohesive interactions between them 1 [4, 5]. -

Starvation in Bacteria Starvation in Bacteria
Starvation in Bacteria Starvation in Bacteria Edited by Staffan Kjelleberg University 0/ Göteborg Göteborg, Sweden and University 0/ New South Wales Sydney, Australia SPRINGER SCIENCE+BUSINESS MEDIA, LLC Library of Congress Cataloging-In-Publication Data Starvation 1n bacteria / edited by Staffan Kjeiieberg. p. cm. Includes bibliographical references and Index. 1. M1crob1al netaboHsn. 2. Starvation. I. Kjeileberg, Staffan. QR88.S7 1993 589.9" 0133—dc 20 93-21918 CIP This limited facsimile edition has been issued for the purpose of keeping this title available to the scientific community. 10 98765432 ISBN 978-0-306-44430-2 ISBN 978-1-4899-2439-1 (eBook) DOI 10.1007/978-1-4899-2439-1 © Springer Science+Business Media New York 1993 Originally published by Plenum Press, New York in 1993 Softcover reprint of the hardcover 1st edition 1993 All rights reserved No part of this book may be reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, microfilming, recording, or otherwise, without written permission from the Publisher Preface Concerted efforts to study starvation and survival of nondifferentiating vegeta tive heterotrophic bacteria have been made with various degrees of intensity, in different bacteria and contexts, over more than the last 30 years. As with bacterial growth in natural ecosystem conditions, these research efforts have been intermittent, with rather long periods of limited or no production in between. While several important and well-received reviews and proceedings on the topic of this monograph have been published during the last three to four decades, the last few years have seen a marked increase in reviews on starvation survival in non-spore-forming bacteria. -

American Association for the Advancement of Science
Bridging Science and Society aaas annual report | 2010 The American Association for the Advancement of Science (AAAS) is the world’s largest general scientific society and publisher of the journal Science (www.sciencemag.org) as well as Science Translational Medicine (www.sciencetranslationalmedicine.org) and Science Signaling (www.sciencesignaling.org). AAAS was founded in 1848 and includes some 262 affiliated societies and academies of science, serving 10 million individuals. Science has the largest paid circulation of any peer- reviewed general science journal in the world, with an estimated total readership of 1 million. The non-profit AAAS (www.aaas.org) is open to all and fulfills its mission to “advance science and serve society” through initiatives in science policy; international programs; science education; and more. For the latest research news, log onto EurekAlert!, www.eurekalert.org, the premier science- news Web site, a service of AAAS. American Association for the Advancement of Science 1200 New York Avenue, NW Washington, DC 20005 USA Tel: 202-326-6440 For more information about supporting AAAS, Please e-mail [email protected], or call 202-326-6636. The cover photograph of bridge construction in Kafue, Zambia, was captured in August 2006 by Alan I. Leshner. Bridge enhancements were intended to better connect a grass airfield with the Kafue National Park to help foster industry by providing tourists with easier access to new ecotourism camps. [FSC MixedSources logo / Rainforest Alliance Certified / 100 percent green -

Thèse De Doctorat De L'université Pierre Et Marie Curie Laboratoire
Thèse de doctorat de l’université Pierre et Marie Curie Ecole doctorale de Chimie Physique et Chimie Analytique de Paris-Centre Laboratoire Colloïdes et Matériaux Divisés Sujet de thèse : Cultures multi-parallélisées en millifluidique digitale : diversité et sélection artificielle Présentée par : Jean-Baptiste Dupin Soutenue le 15 juin 2018 Devant le Jury composé de : M. Jean-Marie François Rapporteur M. Pascal Panizza Rapporteur Mme Valérie Pichon Présidente du Jury Mme Silvia De Monte Examinatrice M. Hicham Ferhout Invité M. Jérôme Bibette Directeur de thèse M. Jean Baudry Co-encadrant 2 Remerciements Un long chemin a été parcouru pendant ces trois ans et demi de thèse au Laboratoire Colloïdes et Matériaux Divisés et je souhaite ici remercier toutes les personnes que j’ai pu rencontrer au cours de mes recherches, qui m’ont conseillé et entouré au laboratoire comme en dehors. Je remercie tout d’abord Jérôme Bibette pour m’avoir accueilli au LCMD sur un sujet, certes risqué, mais qui me motivait énormément. En tant que directeur de thèse, il a su me guider dans les directions que devaient prendre ma thèse tout en me laissant une très grande autonomie. Son accompagnement bienveillant et sa confiance m’ont laissé apprécier les avancées concluantes des travaux et m’ont ainsi fait progresser dans ma réflexion scientifique. Je tiens aussi à remercier Jean Baudry et Nicolas Bremond de qui le suivi continu et les échanges autour de la biologie, de l’instrumentation et de l’hydrodynamique m’ont été très profitables. Je remercie ensuite chacun des membres du jury de ma soutenance de thèse pour leur lecture critique et l’appréciation précieuse qu’ils ont porté sur ce travail mêlant physico-chimie, théorie de l’évolution et microbiologie : Valérie Pichon pour m’avoir fait l’honneur de présider mon jury, Jean-Marie François et Pascal Panizza pour avoir accepté la tâche d’être rapporteurs, et enfin Silvia De Monte et Hicham Ferhout pour l’intérêt qu’ils ont porté à mon travail. -

Isolation and Characterization of an Escherichia Coli Mutant Defective in Resuming Growth After Starvation
Downloaded from genesdev.cshlp.org on September 27, 2021 - Published by Cold Spring Harbor Laboratory Press Isolation and characterization of an Escherichia coli mutant defective in resuming growth after starvation Deborah A. Siegele 1,2 and Roberto Kolter ~ 2Department of Biology, Texas A&M University, College Station, Texas 77843-3258 USA; 3Department of Microbiology and Molecular Genetics, Harvard Medical School, Boston, Massachusetts 02115 USA To understand the mechanisms that allow the enteric bacterium Escherichia coli to make the transitions between growth and stationary phase and to maintain cell viability during starvation, we have looked for mutants defective in stationary-phase survival (a Sur- phenotype). In this paper we describe a conditional E. coli mutant, surB1, that grows normally and remains viable during stationary phase but is unable to exit stationary phase and resume aerobic growth at high temperature. Thus, the surB gene product is not required for cell survival per se but, rather, it is required for starved cells to reinitiate growth under restrictive conditions. Once growth has started, SurB function is no longer required. Mutant cells sense and respond to fresh medium but appear to arrest growth before the first cell division. The surB gene was mapped to 19.5 rain on the E. coli chromosome, cloned, and sequenced. The surB gene product is predicted to be an integral membrane protein with multiple membrane-spanning regions and is homologous to the ATP-binding cassette (ABC) family of transporters, a large family of transport proteins found in both prokaryotic and eukaryotic cells. An open reading frame, designated ybjA, was found immediately upstream of surB and may be in an operon with surB.