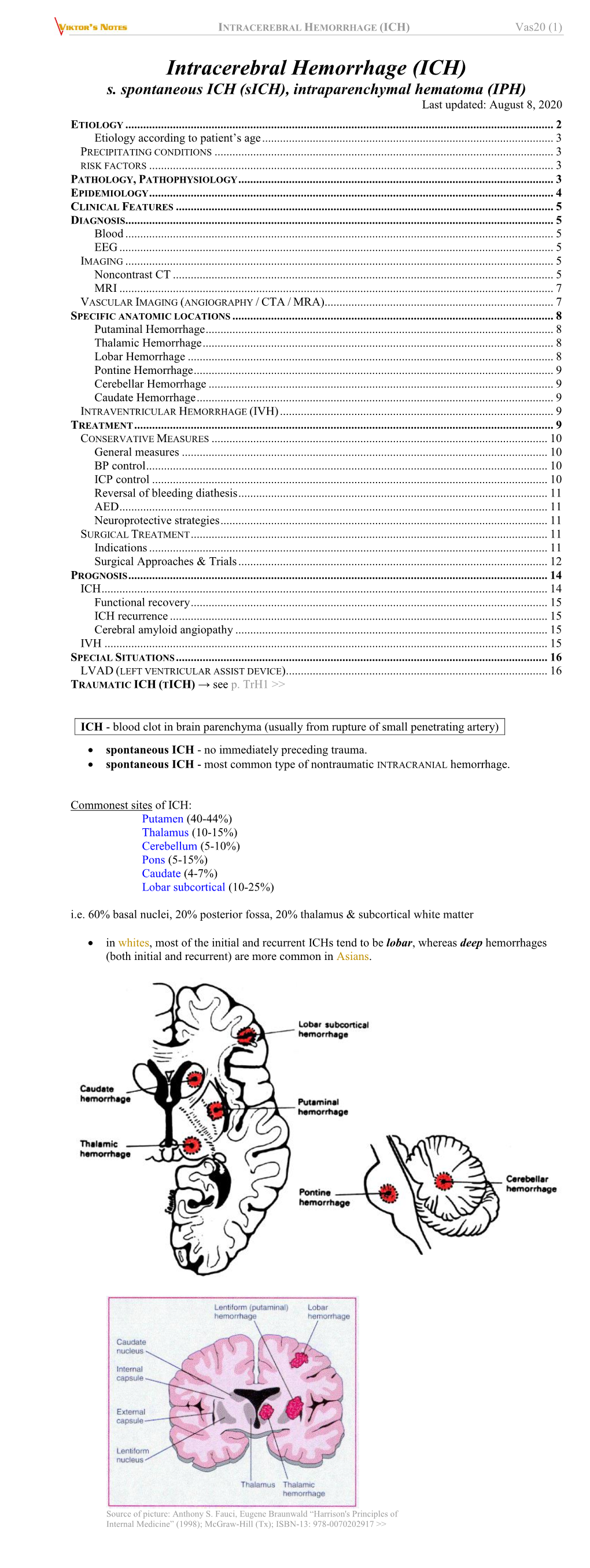
INTRACEREBRAL HEMORRHAGE (ICH) Vas20 (1)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

A Bilateral Cortico-Striate Projection
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.28.1.71 on 1 February 1965. Downloaded from J. Neurol. Neurosurg. Psychiat., 1965, 28, 71 A bilateral cortico-striate projection J. B. CARMAN, W. M. COWAN, T. P. S. POWELL, AND K. E. WEBSTER From the Departments of Anatomy, University of Oxford, and University College, London During the course of studies on the projection of the ined, and evidence for a bilateral projection has been cerebral cortex upon the striatum in the rabbit found in 20 animals. The evidence for this projec- (Carman, Cowan, and Powell, 1963) and the cat tion depends upon the collective findings in several (Webster, 1964) degeneration was seen bilaterally in brains, but only a few typical examples will be Nauta preparations of the striatum in some, but not described in full. The findings in the remaining all, animals. For two main reasons this observation experiments will be summarized in composite was not included in the earlier study. First, because figures. of the difficulty of interpreting any findings of Experiment R30 is representative of the rabbit bilateral degeneration in silver preparations, and, brains in which a projection to the contralateral particularly as it is well known that the striatum striatum was found after a lesion involving the sen- commonly shows pseudo-degeneration, it was im- sori-motor cortex. The cortical damage in this brain perative to exclude this possibility by the prepara- is in the form of a broad strip along the dorsal guest. Protected by copyright. tion of further material using both the frozen and surface of the hemisphere from just behind the paraffin Nauta methods. -

Rhesus Monkey Brain Atlas Subcortical Gray Structures
Rhesus Monkey Brain Atlas: Subcortical Gray Structures Manual Tracing for Hippocampus, Amygdala, Caudate, and Putamen Overview of Tracing Guidelines A) Tracing is done in a combination of the three orthogonal planes, as specified in the detailed methods that follow. B) Each region of interest was originally defined in the right hemisphere. The labels were then reflected onto the left hemisphere and all borders checked and adjusted manually when necessary. C) For the initial parcellation, the user used the “paint over function” of IRIS/SNAP on the T1 template of the atlas. I. Hippocampus Major Boundaries Superior boundary is the lateral ventricle/temporal horn in the majority of slices. At its most lateral extent (subiculum) the superior boundary is white matter. The inferior boundary is white matter. The anterior boundary is the lateral ventricle/temporal horn and the amygdala; the posterior boundary is lateral ventricle or white matter. The medial boundary is CSF at the center of the brain in all but the most posterior slices (where the medial boundary is white matter). The lateral boundary is white matter. The hippocampal trace includes dentate gyrus, the CA3 through CA1 regions of the hippocamopus, subiculum, parasubiculum, and presubiculum. Tracing A) Tracing is done primarily in the sagittal plane, working lateral to medial a. Locate the most lateral extent of the subiculum, which is bounded on all sides by white matter, and trace. b. As you page medially, tracing the hippocampus in each slice, the superior, anterior, and posterior boundaries of the hippocampus become the lateral ventricle/temporal horn. c. Even further medially, the anterior boundary becomes amygdala and the posterior boundary white matter. -

The Embryology and Fiber Tract Connections of the Corpus Striatum in the Albino Rat
Loyola University Chicago Loyola eCommons Master's Theses Theses and Dissertations 1935 The Embryology and Fiber Tract Connections of the Corpus Striatum in the Albino Rat James K. L. Choy Loyola University Chicago Follow this and additional works at: https://ecommons.luc.edu/luc_theses Part of the Anatomy Commons Recommended Citation Choy, James K. L., "The Embryology and Fiber Tract Connections of the Corpus Striatum in the Albino Rat" (1935). Master's Theses. 22. https://ecommons.luc.edu/luc_theses/22 This Thesis is brought to you for free and open access by the Theses and Dissertations at Loyola eCommons. It has been accepted for inclusion in Master's Theses by an authorized administrator of Loyola eCommons. For more information, please contact [email protected]. This work is licensed under a Creative Commons Attribution-Noncommercial-No Derivative Works 3.0 License. Copyright © 1935 James K. L. Choy LOYOLA UNIVERSITY SCHOOl, OF MEDICINE THE EMBRYOLOGY AND FIBER TRACT CONNECTIONS OF THE CORPUS STRIATUM IN THE ALBINO RAT. A THESIS SUBMITTED TO THE FACULTY of the GRADUATE SCHOOL of LOYOLA UNIVERSITY IN CANDIDACY FOR THE DEGREE OF MASTER OF SCIENCE by James K.L. Choy, B.S.M. 1935 THE EMBRYOLOGY AND FIBER TRACT CONNECTIONS OF THE CORPUS STRIATUM IN THE ALBINO RAT. I. PREFACE Before entering upon a discussion of the problem itself, I would lil{e to take this opportunity to acknowledge the assis tance and encouragement I received in the preparation of this paper. To Dr. R. M. Strong, who suggested the problem, I am deeply obligated for his encouragement, practical guidance, and helpful suggestions in the procedure of this work. -

Marrow Stromal Cells Migrate Throughout Forebrain and Cerebellum, and They Differentiate Into Astrocytes After Injection Into Neonatal Mouse Brains
Proc. Natl. Acad. Sci. USA Vol. 96, pp. 10711–10716, September 1999 Cell Biology Marrow stromal cells migrate throughout forebrain and cerebellum, and they differentiate into astrocytes after injection into neonatal mouse brains GENE C. KOPEN,DARWIN J. PROCKOP, AND DONALD G. PHINNEY* Center for Gene Therapy, MCP Hahnemann University, 245 North 15th Street, Philadelphia, PA 19102-1192 Contributed by Darwin J. Prockop, July 16, 1999 ABSTRACT Stem cells are a valuable resource for treat- cell lineages after transplantation into the hematopoietic ing disease, but limited access to stem cells from tissues such system of irradiated hosts (11). Together, these findings sug- as brain restricts their utility. Here, we injected marrow gest that it may be possible to reconstitute a tissue by using stromal cells (MSCs) into the lateral ventricle of neonatal stem cells from a separate dermal origin. To determine mice and asked whether these multipotential mesenchymal whether mesenchymal stem cells can adopt neural cell fates, we progenitors from bone marrow can adopt neural cell fates injected a purified population of murine MSCs into the lateral when exposed to the brain microenvironment. By 12 days ventricles of neonatal mice and examined the fate of these cells postinjection, MSCs migrated throughout the forebrain and by immunohistochemistry. cerebellum without disruption to the host brain architecture. Some MSCs within the striatum and the molecular layer of the MATERIALS AND METHODS hippocampus expressed glial fibrillary acidic protein and, therefore, differentiated into mature astrocytes. MSCs also Isolation and Purification of MSCs. Murine MSC cultures populated neuron rich regions including the Islands of were established from the bone marrow of FVB͞N mice (The Calleja, the olfactory bulb, and the internal granular layer of Jackson Laboratory) and were cultured for 7 days (12). -

Features of the Cerebral Vascular Pattern That Predict Vulnerability to Perfusion Or Oxygenation Deficiency: an Anatomic Study
431 Features of the Cerebral Vascular Pattern That Predict Vulnerability to Perfusion or Oxygenation Deficiency: An Anatomic Study D. M. Moody1 In an ongoing study of brain microvasculature in humans at autopsy, we had the 1 2 M.A. Bell · opportunity to analyze the overall scheme of this vascular supply. The native endothelial V. R. Challa3 membrane enzyme, alkaline phosphatase, is used to precipitate black lead sulfide salt in the vessel wall, rendering the brain microvasculature visible by both light microscopy and microradiography. There are six distinct patterns of intraparenchymal afferent blood supply to the supratentorial brain: short arterioles from a single source (e.g., those in the cortex); short- to intermediate-length arterioles, single source (anterior two-thirds of the corpus callosum); short- to intermediate-length arterioles and arteries, dual source (subcortical U fibers); intermediate-length arterioles and arteries, triple source (extreme/ external capsule and claustrum); long arteries and arterioles, single source (centrum semiovale); and large, long muscular arteries, single source (thalamus and basal ganglia). The nature of this arrangement offers some protection to certain regions of the cerebrum from circulatory challenges such as hypotension, while leaving other areas vulnerable. The distal arterioles supplying two of these protected regions, the U-fiber area and the extreme/external capsule and claustrum area, also exhibit the feature of interdigitation, which can offer additional collateral potential from one arteriolar territory to the next. Aging, hypertension, diabetes mellitus, and atherosclerosis can have a significant impact on brain microcirculation. The way in which vascular patterns dictate the distribution of these effects is discussed. The ability to stain the cerebral microvessels and demonstrate the finer points of their patterns in sections and microradiographs has enabled us to resolve some long-standing questions about vascular connections and directions. -
Neuroprotection of the Hypoxic-Ischemic Mouse Brain By
www.nature.com/scientificreports OPEN Neuroprotection of the hypoxic- ischemic mouse brain by human CD117+CD90+CD105+ amniotic Received: 14 November 2017 Accepted: 23 January 2018 fuid stem cells Published: xx xx xxxx Michelangelo Corcelli1, Kate Hawkins1, Filipa Vlahova1, Avina Hunjan1, Kate Dowding1, Paolo De Coppi2, Anna L. David 1,3, Donald Peebles1, Pierre Gressens4, Henrik Hagberg4,5, Mariya Hristova1 & Pascale V. Guillot1 Human amniotic fuid contains two morphologically-distinct sub-populations of stem cells with regenerative potential, spindle-shaped (SS-hAFSCs) and round-shaped human amniotic fuid stem cells (RS-hAFSCs). However, it is unclear whether morphological diferences correlate with functionality, and this lack of knowledge limits their translational applications. Here, we show that SS-hAFSCs and RS-hAFSCs difer in their neuro-protective ability, demonstrating that a single contralateral injection of SS-hAFSCs into hypoxic-ischemic P7 mice conferred a 47% reduction in hippocampal tissue loss and 43–45% reduction in TUNEL-positive cells in the hippocampus and striatum 48 hours after the insult, decreased microglial activation and TGFβ1 levels, and prevented demyelination. On the other hand, RS-hAFSCs failed to show such neuro-protective efects. It is possible that SS-hAFSCs exert their neuroprotection via endoglin-dependent inhibition of TGFβ1 signaling in target cells. These fndings identify a sub-population of CD117+CD90+CD105+ stem cells as a promising source for the neuro- protection of the developing brain. Human fetal stem cells present a number of advantageous characteristics over their adult counterparts, such as faster growth kinetics, longer telomeres and higher diferentiation potential1, thus presenting an intermediate phenotype between adult mesenchymal stem cells and embryonic stem cells2. -

Unusual Lesion in the Bilateral External Capsule Following Status Epilepticus: a Case Report
Unusual Lesion in the Bilateral External Capsule Following Status Epilepticus: A Case Report Case Report Kyoung Jin Hwang, Key-Chung Park, Sung Sang Yoon, Tae-Beom Ahn Journal of Epilepsy Research pISSN 2233-6249 / eISSN 2233-6257 Department of Neurology, Kyung Hee University School of Medicine, Seoul, Korea Magnetic resonance imaging (MRI) is an essential tool for determining the underlying cause of status epilepticus and can exhibit a variety of unpredictable findings. A 28-year-old woman presented with Received October 24, 2014 status epilepticus of unknown etiology. She had been recovered from status epilepticus twenty days Accepted December 4, 2014 later, but afterwards developed transient postural instability and cognitive impairment. Initial MRI Corresponding author: Tae-Beom Ahn Department of Neurology, Kyung Hee showed no abnormalities. Follow-up MRI after cessation of status epilepticus demonstrated hyper- University Medical Center, intensities lesions in the right claustrum and bilateral external capsular areas on T2 fluid attenuated 23 Kyungheedae-ro, Dongdaemun-gu, inversion recovery images. As the external capsule is a route for cholinergic and corticostriatal fibers, Seoul 130-872, Korea Tel. +82-2-958-8499 cognitive dysfunction and postural instability might be related to these fibers. (2014;4:88-90) Fax. +82-2-958-8490 E-mail; [email protected] Key words: Magnetic resonance imaging, Status epilepticus, External capsule Introduction Complete blood counts were normal. Cerebrospinal fluid was clean and contained no leukocytes, with normal glucose (73 mg/dL) Status epilepticus (SE) is a neurological emergency that may result and protein (41.5 mg/dL). The results of serologic analysis of blood in serious morbidity and mortality.1 Magnetic resonance imaging and cerebrospinal fluid (CSF), including polymerase chain reaction (MRI) is an essential tool for determining the underlying cause of SE for herpes viruses, were within normal range. -

Tbr1 Regulates Differentiation of the Preplate and Layer 6
Neuron, Vol. 29, 353±366, February, 2001, Copyright 2001 by Cell Press Tbr1 Regulates Differentiation of the Preplate and Layer 6 Robert F. Hevner,* Limin Shi,* Nick Justice,* proliferative cells of the ventricular zone (reviewed in Yi-Ping Hsueh,² Morgan Sheng,² Susan Smiga,* Allendoerfer and Shatz, 1994). Subsequent generations Alessandro Bulfone,*# Andre M. Goffinet,§ of postmitotic neurons migrate into the preplate and Anthony T. Campagnoni,³ intercalate between the inner and outer cell populations, and John L. R. Rubenstein*k to form the cortical plate. Thus, the cortical plate splits *Nina Ireland Laboratory of the preplate into superficial and deep components, Developmental Neurobiology thereafter termed the marginal zone and subplate, re- Department of Psychiatry spectively (Allendoerfer and Shatz, 1994). The cortical University of California, San Francisco plate grows in an ªinside-outº order, from layer 6, which San Francisco, California 94143 contains the earliest-born cortical plate neurons, to layer ² Howard Hughes Medical Institute and 2, which contains the latest-born neurons (Angevine and Department of Neurobiology Sidman, 1961; Caviness, 1982). Massachusetts General Hospital and The preplate is thought to function primarily as a Harvard Medical School framework for further development of the cortex, or- Boston, Massachusetts 02114 ganizing its laminar structure and some of its connec- ³ Neuropsychiatric Institute tions. In mice, preplate cells differentiate into at least UCLA Medical School two distinct types of neurons: Cajal-Retzius cells and 760 Westwood Plaza subplate cells (though other classifications have also Los Angeles, California 90024 been proposed; see Meyer et al., 1998, 1999). Cajal- § Neurobiology Unit Retzius cells express Reelin and calretinin (del RõÂoet FUNDP Medical School al., 1995; Alca ntara et al., 1998; Meyer et al., 1999) and B5000 Namur have been implicated in controlling cell migrations (re- Belgium viewed by Rice and Curran, 1999) and radial glia mor- phology (SupeÁ r et al., 2000). -

Cortical and Subcortical Anatomy: Basics and Applied
43rd Congress of the Canadian Neurological Sciences Federation Basic mechanisms of epileptogenesis and principles of electroencephalography Cortical and subcortical anatomy: basics and applied J. A. Kiernan MB, ChB, PhD, DSc Department of Anatomy & Cell Biology, The University of Western Ontario London, Canada LEARNING OBJECTIVES Know and understand: ! Two types of principal cell and five types of interneuron in the cerebral cortex. ! The layers of the cerebral cortex as seen in sections stained to show either nucleic acids or myelin. ! The types of corrtex: allocortex and isocortex. ! Major differences between extreme types of isocortex. As seen in primary motor and primary sensory areas. ! Principal cells in different layers give rise to association, commissural, projection and corticothalamic fibres. ! Cortical neurons are arranged in columns of neurons that share the same function. ! Intracortical circuitry provides for neurons in one column to excite one another and to inhibit neurons in adjacent columns. ! The general plan of neuronal connections within nuclei of the thalamus. ! The location of motor areas of the cerebral cortex and their parallel and hierarchical projections to the brain stem and spinal cord. ! The primary visual area and its connected association areas, which have different functions. ! Somatotopic representation in the primary somatosensory and motor areas. ! Cortical areas concerned with perception and expression of language, and the anatomy of their interconnections. DISCLOSURE FORM This disclosure form must be included as the third page of your Course Notes and the third slide of your presentation. It is the policy of the Canadian Neurological Sciences Federation to insure balance, independence, objectivity and scientific rigor in all of its education programs. -

Mmubn000001 115756426.Pdf
PDF hosted at the Radboud Repository of the Radboud University Nijmegen The following full text is a publisher's version. For additional information about this publication click this link. http://hdl.handle.net/2066/148580 Please be advised that this information was generated on 2021-10-03 and may be subject to change. PROMOTOR: PROF. DR. H. J. LAMMERS THE ANTERIOR COMMISSURE OF THE RABBIT Λ DESCRIPTIVE AND EXPERIMENTAL ΑΝΑΊ OMICAL STUDY WITH AN ATLAS OF THE RABBIT TELENCEPHALON IN HORIZONTAL SECTIONS PROEFSCHRIFT EER VERKRIJGING VAN DE GRAAD VAN DOCTOR IN DE GENEESKUNDE AAN DE KATHOLIEKE UNIVERSITEIT TE NIJMEGEN OP GEZAG VAN DE RECTOR MAGNIFICUS MR. S. F. L. BARON VAN WIJNBERGEN, HOOGLERAAR IN DE FACULTEITEN DER RECHTSGELEERDHEID EN DER SOCIALE WETENSCHAPPEN, VOLGENS BESLUIT VAN DE SENAAT IN HET OPENBAAR TE VERDEDIGEN OP MAANDAG 23 JUNI 1969, DES NAMIDDAGS TE 4 UUR door HENTDRIKUS AUGUSTINUS MARIA VAN ALPHEN geboren te Vcnlo 1969 H. j. w. BECHT'S UITGEVERSMAATSCHAPPIJ N.V., AMSTERDAM Dit proefschrift werd bewerkt in het lahoratonum voor anatomie en embryologie (hoofd Prof Dr H J Lammers) van de Katholieke Universiteit te Nijmegen onder supervisie van Dr A H M Lohman Het proefschrift verschijnt tevens als supplement 57 — 1 ad Vol 74 (1969) \an de 'Acta Anatomica' Voor Vader en Moeder CONTENTS General introduction . Parti Survey of the structure of the rabbit telencephalon Introduction ... Material and methods . Classification and nomenclature . The prcpiriform region . The anterior commissure . Atlas . Abbreviations . Part II Experimental anatomical study of the posterior limb terminal's component of the anterior commissure . Survey of the literature . Material and methods . -
INTERNAL CAPSULE • Projection Fibres- Internal Capsule
INTERNAL CAPSULE • Projection fibres- Internal capsule r ~OnQih..!1c:lll i~J ~asd · I.JS OOi 1n1ssur DEFINITION Rostrum ol co,pi.c:; • Projection fibres c.allosum (white matter) between nucleus • caudate nucleus and /---~.__~---- :r~~l thalamus medially capS,Jle Pos1enu1 1111-0 of 1mema1 • lentiform nucleus capsule Thalamus laterally Actf'CNeflocular part of internal capsule 10.24 Horizontal sec11u11 01 lilt cerebral hemisphere st10win9 the Ooc1pr1~• p<Jlt!' - nl lhti rnla o-n~I r~n-e-11l it • Internal Capsule- A compact bundle of fibres through which the large collections of fibres pass, including- • Thalamocortical fibres • Corticothalamic fibres • Corticopontine fibres • Corticobulbar fibres • Corticospinal fibres • The fibres project from the cerebral cortex to the various nuclei of the extrapyramidal system (e.g., the putamen and caudate nucleus). • It is a continuous sheet of fibres that forms the medial boundary of the lenticular nucleus. • It continues around posteriorly and inferiorly to partially envelop this nucleus. • Inferiorly, many of the fibres of the internal capsule funnel into the cerebral peduncles. • Superiorly, the fibres fan out into the corona radiata. • Here, they travel in the cerebral white matter to reach their cortical origins or destinations. The internal capsule is divided into 5 regions: • The anterior limb is the portion between the lenticular nucleus and the head of the caudate nucleus; • The posterior limb is the portion between the lenticular nucleus and the thalamus; • The genu is the portion at the junction of the above 2 parts and is adjacent to the interventricular foramen; • The retrolenticular part is the portion posterior to the lenticular nucleus; • The sublenticular part is the portion inferior to the lenticular nucleus. -

A Case of Striatal Hemiplegia
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.30.2.134 on 1 April 1967. Downloaded from J. Neurol. Neurosurg. Psychiat., 1967, 30, 134 A case of striatal hemiplegia D. R. OPPENHEIMER From the Department of Neuropathology, Radcliffe Infirmary, Oxford In man, pure lesions of the striatum (putamen and were: (1) half an inch of relative shortening of the left caudate nucleus) are rare. Diseases which affect the arm, with wasting of the fingers; (2) increased resistance striatum preferentially (Huntington's chorea, to passive movement at all joints on the left and tendon the Jakob- reflexes were hard to elicit because of stiffness. The left Wilson's disease, encephalopathy of plantar response was indeterminate; (3) absence of Creutzfeldt type, some forms of arterial disease) voluntary movement ofthe left fingers and toes and at the almost always involve other basal nuclei, cerebral left ankle, the power at the more proximal joints being cortex, or white matter to some extent, and the well preserved; (4) recurrent painless 'spasms', during clinical picture is more or less complicated (Martin, which the left arm was either flexed or extended at the 1959). In experimental animals, it is very difficult to shoulder, the elbow was extended, the wrist dorsiflexed achieve extensive destruction of the striatum without and the fingers flexed into a fist; (5) slight dragging of the involving other structures, in particular the pallidum left leg in walking; (6) a bruit heard over the right and the internal capsule. common carotid artery. In the case to be described here, a vascular accident A right carotid arteriogram revealed a small angio- matous malformation, drained by an enlarged venous Protected by copyright.