Glomerular Disease and Glomerulonephritis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Extrarenal Complications of the Nephrotic Syndrome
Kidney International, Vol. 33 (/988), pp. 1184—1202 NEPHROLOGY FORUM Extrarenal complications of the nephrotic syndrome Principal discussant: DAVID B. BERNARD The University Hospital and Boston University Sc/zoo!ofMedicine, Boston, Massachusetts present and equal. The temperature was 100°F. The blood pressure was 110/70 mm Hg in the right arm with the patient supine and standing. The Editors patient had no skin rashes, peteehiae, clubbing, or jaundice. Examina- JORDANJ. COHEN tion of the head and neck revealed intact cranial nerves and normal fundi. Ears, nose, and throat were normal. The jugular venous pressure Jot-IN T. HARRtNOTON was not increased. No lymph glands were palpable in the neck or JEROME P. KASSIRER axillae, and the trachea was midline, cardiac examination was normal. NICOLA05 E. MAmAs Examination of the lungs revealed coarse rales at the right base but no other abnormalities. Abdominal examination revealed aseites, but no Editor abdominal guarding, tenderness, or rigidity. The liver and spleen were Managing not palpable and no masses were present. The urine contained 4± CHERYL J. ZUSMAN protein; microscopic examination revealed free fat droplets, many oval fat bodies, and numerous fatty casts. Five to 10 red blood cells were seen per high-power field, but no red blood cell casts were present. A Universityof'Chicago Pritzker School of Medicine 24-hr urine collection contained 8 g of protein. The BUN was 22 mg/dl; creatinine, 2.0 mg/dl; and electrolytes were and normal. Serum total calcium was 7.8 mg/dl, and the phosphorus was 4.0 Taf is University School of' Medicine mg/dl. -

Glomerulonephritis Management in General Practice
Renal disease • THEME Glomerulonephritis Management in general practice Nicole M Isbel MBBS, FRACP, is Consultant Nephrologist, Princess Alexandra lomerular disease remains an important cause Hospital, Brisbane, BACKGROUND Glomerulonephritis (GN) is an G and Senior Lecturer in important cause of both acute and chronic kidney of renal impairment (and is the commonest cause Medicine, University disease, however the diagnosis can be difficult of end stage kidney disease [ESKD] in Australia).1 of Queensland. nikky_ due to the variability of presenting features. Early diagnosis is essential as intervention can make [email protected] a significant impact on improving patient outcomes. OBJECTIVE This article aims to develop However, presentation can be variable – from indolent a structured approach to the investigation of patients with markers of kidney disease, and and asymptomatic to explosive with rapid loss of kidney promote the recognition of patients who need function. Pathology may be localised to the kidney or further assessment. Consideration is given to the part of a systemic illness. Therefore diagnosis involves importance of general measures required in the a systematic approach using a combination of clinical care of patients with GN. features, directed laboratory and radiological testing, DISCUSSION Glomerulonephritis is not an and in many (but not all) cases, a kidney biopsy to everyday presentation, however recognition establish the histological diagnosis. Management of and appropriate management is important to glomerulonephritis (GN) involves specific therapies prevent loss of kidney function. Disease specific directed at the underlying, often immunological cause treatment of GN may require specialist care, of the disease and more general strategies aimed at however much of the management involves delaying progression of kidney impairment. -

Management of Adult Minimal Change Disease
Kidney CaseCJASN Conference: ePress. Published on April 5, 2019 as doi: 10.2215/CJN.01920219 How I Treat Management of Adult Minimal Change Disease Stephen M. Korbet and William L. Whittier Clin J Am Soc Nephrol 14: ccc–ccc, 2019. doi: https://doi.org/10.2215/CJN.01920219 Introduction Initial Treatment and Course in Adult Minimal Minimal change disease is responsible for idiopathic Change Disease Division of nephrotic syndrome in .75% of children and up to Minimal change disease in adults is highly steroid Nephrology, 30% of adults (1–5). Although secondary causes of sensitive, but steroid resistance is seen in 5%–20% of Department of Medicine, Rush minimal change disease (i.e., nonsteroidal anti- adult patients (1–6). When steroid resistance is ob- fl University Medical in ammatory drugs, lithium, and lymphoproliferative served, the patient often has FSGS on re-examination Center, Chicago, disorders) are uncommon in children, they account of the initial biopsy or on rebiopsy (1,3,6). Although Illinois for up to 15% of minimal change disease in adults 95% of children attain a remission with steroid (1,3). Thus, it is important to assess adults with therapy by 8 weeks, only 50%–75% of adults do so Correspondence: minimal change disease for secondary causes as the (1–6). It is not until after 16 weeks of treatment that Dr. Stephen M. Korbet, – Division of prognosis, and therapeutic approach is determined most adults (75% 95%) enter a remission, with the Nephrology, by the underlying etiology. majority attaining a complete remission (proteinuria Department of of #300 mg/d) and a minority attaining a partial Medicine, Rush remission (proteinuria of .300 mg but ,3.5 g/d). -

Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute Staphylococcal Osteomyelitis
Diffuse Proliferative Glomerulonephritis and Acute Renal Failure Associated with Acute Staphylococcal Osteomyelitis MATTHEW D. GRIFFIN,* JOHANNES BJORNSSON,t and STEPHEN B. ERICKSON* *Department of Internal Medicine, Division of Nephrology, and tDepartment of Pathology, Mayo Clinic and Mayo Foundation, Rochester, Minnesota. Abstract. A 72-year-old man developed acute renal failure after peated surgical debridement. Spontaneous recovery of renal coronary bypass surgery that had been complicated by sternal function occurred after eradication of infection and final sur- osteomyelitis caused by the Staphylococcus aureus bacterium. gical wound repair. The relationship between acute bacterial Bacteremia and sepsis were not present. Renal biopsy demon- infections and glomerulonephritis and, in particular, the causal strated a florid, diffuse, proliferative glomerulonephritis with role of staphylococcal antigens in the pathogenesis of such glomerular immune complex deposition. Management in- lesions is discussed. (J Am Soc Nephrol 8: 1633-1639, 1997) cluded hemodialysis, prolonged antibiotic therapy, and re- Coagulase-positive staphylococcus (Staphylococcus aureus) is mg/dl]) and in the immediate postoperative period. Over the the most common causative organism in acute osteomyelitis following days, the patient’s serum creatinine concentration (1). Along with coagulase-negative staphylococcal species, it increased progressively, and hemodialysis was instituted on has also been implicated in the pathogenesis of immune com- day 23 after CABG. There was no past or family history of plex (IC)-mediated diffuse proliferative glomerulonephritis renal disease and no known drug allergies. Prior medical (DPGN) in a variety of infections. These include bacterial history had included degenerative disc disease, stable abdom- endocarditis, ventriculoatrial shunt infections, pneumonia, and inal aortic aneurysm, stable benign prostatic hyperplasia, and visceral abscesses with or without septicemia (2-6). -

T Cells and Minimal Change Disease
EDITORIALS J Am Soc Nephrol 13: 1409–1411, 2002 T Cells and Minimal Change Disease ROBYN CUNARD AND CAROLYN J. KELLY Research Service, VA San Diego Healthcare System; and Department of Medicine, University of California, San Diego, California. It is one of the ironies of medical practice that as physicians we the lymphokine may exert a direct effect on the GBM or can competently and confidently treat diseases of whose patho- activate mesangial cells to produce a factor that altered glo- genesis we remain woefully ignorant. merular permeability (2). Such is the case with minimal change disease, the most This publication preceded by over a decade the molecular common diagnosis associated with the nephrotic syndrome in definition of the T cell antigen receptor as a heterodimeric children (MCNS). The disease manifestations of nephrotic- structure derived from gene rearrangements (3) and the cloning range proteinuria, hypoalbuminemia, and hyperlipidemia in of the first cytokine or lymphokine (4). It preceded by several such patients are typically reversible with corticosteroid ther- years the earliest attempts to characterize subsets of T lympho- apy. MCNS has, by definition, no abnormalities apparent on cytes by their functional and phenotypic heterogeneity (5,6). analysis of kidney biopsy specimens by light microscopy. Shalhoub’s hypothesis has resurfaced multiple times since Humoral components of the immune system, such as Ig and 1974, as clinical investigators take advantage of increased complement, are absent on immunofluorescent analysis of cor- knowledge about immunology and technical breakthroughs to tical kidney sections. The sole abnormalities seen in the kidney reexamine the role of T cells in MCNS. -

Portal Vein Thrombosis in Minimal Change Disease
Ewha Med J 2014;37(2):131-135 Case http://dx.doi.org/10.12771/emj.2014.37.2.131 Report pISSN 2234-3180 • eISSN 2234-2591 Portal Vein Thrombosis in Minimal Change Disease Gyuri Kim, Jung Yeon Lee, Su Jin Heo, Yoen Kyung Kee, Seung Hyeok Han Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea Among the possible venous thromboembolic events in nephrotic syndrome, renal Received October 22, 2013, Accepted January 6, 2014 vein thrombosis and pulmonary embolism are common, while portal vein thrombosis (PVT) is rare. This report describes a 26-year-old man with histologically proven mini- Corresponding author mal change disease (MCD) complicated by PVT. The patient presented with epigastric Seung Hyeok Han pain and edema. He had been diagnosed with MCD five months earlier and achieved Department of Internal Medicine, Yonsei complete remission with corticosteroids, which were discontinued one month before University College of Medicine, 50 Yonsei-ro, Seodaemun-gu, Seoul 120-752, Korea the visit. Full-blown relapsing nephrotic syndrome was evident on laboratory and clini- Tel: 82-2-2228-1975, Fax: 82-2-393-6884 cal findings, and an abdominal computed tomography revealed PVT. He immediately E-mail: [email protected] received immunosuppressants and anticoagulation therapy. An eight-week treatment resulted in complete remission, and a follow-up abdominal ultrasonography showed disappearance of PVT. In conclusion, PVT is rare and may not be easily diagnosed in patients with nephrotic syndrome suffering from abdominal pain. Early recognition of Key Words this rare complication and prompt immunosuppression and anticoagulation therapy Minimal change disease; Portal vein are encouraged to avoid a fatal outcome. -

Minimal Change Disease and Focal Segmental Glomerulosclerosis
4 Minimal Change Disease and Focal Segmental Glomerulosclerosis Agnes B. Fogo Introduction/Clinical Setting Minimal change disease (MCD) and focal segmental glomerulosclerosis (FSGS) are both common causes of the nephrotic syndrome. Minimal change disease accounts for greater than 90% of cases of nephrotic syn- drome in children, vs. 10% to 15% of adults with nephrotic syndrome (1). Focal segmental glomerulosclerosis has been increasing in incidence in the United States in both African Americans and in Hispanics, in both adult and pediatric populations (2–4). It is now the most common cause of nephrotic syndrome in adults in the U.S. Patients with FSGS may have hypertension and hematuria. Serologic studies, including complement levels, are typically within normal limits in both MCD and FSGS. Pathologic Features Light Microscopy Minimal change disease shows normal glomeruli by light microscopy (Fig. 4.1). In FSGS, sclerosis involves some, but not all, glomeruli (focal), and the sclerosis affects a portion of, but not the entire, glomerular tuft (seg- mental) (Fig. 4.2) (1,5–7). Sclerosis is defined as increased matrix with obliteration of the capillary lumen. Uninvolved glomeruli in FSGS show no apparent lesions by light microscopy; FSGS may also entail hyalinosis, caused by insudation of plasma proteins, producing a smooth, glassy (hyaline) appearance (Fig. 4.3). Adhesions (synechiae) of the capillary tuft to Bowman’s space are a very early sclerosing lesion. Focal segmental glomerulosclerosis is diagnosed when even a single glomerulus shows segmental sclerosis. Therefore, samples must be ade- quate to detect these focal and segmental lesions. A biopsy with only 10 glomeruli has a 35% probability of missing a focal (10% involved) lesion, decreasing to 12% if 20 glomeruli are sampled (8). -

Glomerulonephritis
Adolesc Med 16 (2005) 67–85 Glomerulonephritis Keith K. Lau, MDa,b, Robert J. Wyatt, MD, MSa,b,* aDivision of Pediatric Nephrology, Department of Pediatrics, University of Tennessee Health Sciences Center, Room 301, WPT, 50 North Dunlap, Memphis, TN 38103, USA bChildren’s Foundation Research Center at the Le Bonheur Children’s Medical Center, Room 301, WPT, 50 North Dunlap, Memphis, TN 38103, USA Early diagnosis of glomerulonephritis (GN) in the adolescent is important in initiating appropriate treatment and controlling chronic glomerular injury that may eventually lead to end-stage renal disease (ESRD). The spectrum of GN in adolescents is more similar to that seen in young and middle-aged adults than to that observed in prepubertal children. In this article, the authors discuss the clinical features associated with GN and the diagnostic evaluation required to determine the specific type of GN. With the exception of hereditary nephritis (Alport’s disease), virtually all types of GN are immunologically mediated with glomerular deposition of immunoglobulins and complement proteins. The inflammatory events leading to GN may be triggered by a number of factors. Most commonly, immune complexes deposit in the glomeruli or are formed in situ with the antigen as a structural component of the glomerulus. The immune complexes then initiate the production of proinflammatory mediators, such as complement proteins and cytokines. Subsequently, the processes of sclerosis within the glomeruli and fibrosis in the tubulointerstitial cells lead to chronic or even irreversible renal injury [1]. Less commonly, these processes occur without involvement of immune complexes—so-called ‘‘pauci-immune GN.’’ * Corresponding author. -
Nephritis Fact Sheet
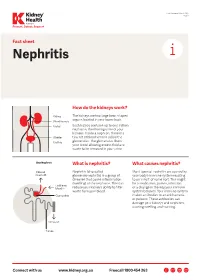
Last Reviewed March 2017 Page 1 Prevent, Detect, Support. Fact sheet Nephritis How do the kidneys work? The kidneys are two large bean-shaped organs located in your lower back. Each kidney contains up to one million nephrons, the filtering units of your kidneys. Inside a nephron, there is a tiny set of blood vessels called the glomerulus. The glomerulus filters your blood allowing excess fluid and waste to be removed in your urine. What is nephritis? What causes nephritis? Nephritis (also called Most types of nephritis are caused by glomerulonephritis) is a group of your body’s immune system reacting diseases that cause inflammation to an ‘insult’ of some sort. This might (swelling) of the nephrons. This can be a medication, poison, infection reduce your kidney’s ability to filter or a change in the way your immune waste from your blood. system behaves. Your immune system makes antibodies to attack bacteria or poisons. These antibodies can damage your kidneys and nephrons, causing swelling and scarring. Connect with us www.kidney.org.au Freecall 1800 454 363 Kidney Health Australia Nephritis Last Reviewed March 2017 Prevent, Detect, Support. Page 2 What are the different types of nephritis? There are many different types of Different types of nephritis include: Nephrotic syndrome: Damage to the nephritis. It can vary from a mild, nephrons causes them to leak large Focal nephritis: Less than a half of non-damaging condition to a serious amounts of protein into your urine your nephrons have scarring, and problem causing kidney failure. Some but little blood. Losing this protein blood and a small amount of protein types of nephritis appear mild at means your body does not have are found in your urine. -

Fibrillary Glomerulonephritis and Immunotactoid Glomerulopathy
PATHOPHYSIOLOGY of the RENAL BIOPSY www.jasn.org Fibrillary Glomerulonephritis and Immunotactoid Glomerulopathy Charles E. Alpers and Jolanta Kowalewska Department of Pathology, University of Washington, Seattle, Washington ABSTRACT extracellular accumulation of haphaz- Fibrillary glomerulonephritis is a now widely recognized diagnostic entity, occur- ardly arranged fibrils measuring ap- ring in approximately 1% of native kidney biopsies in several large biopsy series proximately 16 nm in thickness. Podo- obtained from Western countries. The distinctive features are infiltration of glo- cyte foot processes were diffusely merular structures by randomly arranged fibrils similar in appearance but larger effaced. There was no evidence of than amyloid fibrils and the lack of staining with histochemical dyes typically fibrillary deposits in the tubular base- reactive with amyloid. It is widely but not universally recognized to be distinct from ment membranes or interstitium. The immunotactoid glomerulopathy, an entity characterized by glomerular deposits of diagnosis of fibrillary glomerulone- immunoglobulin with substructural organization as microtubules and with clinical phritis was established on the basis of associations with lymphoplasmacytic disorders. The pathophysiologic basis for the ultrastructural findings in conjunc- organization of the glomerular deposits as fibrils or microtubules in these entities tion with the negative Congo Red stain remains obscure. and typical histologic and immunohis- J Am Soc Nephrol 19: 34–37, 2008. doi: -

Minimal Change Disease: a Case Report of an Unusual Relationship Fahad Edrees Washington University School of Medicine in St
Washington University School of Medicine Digital Commons@Becker Open Access Publications 2016 Minimal change disease: A case report of an unusual relationship Fahad Edrees Washington University School of Medicine in St. Louis Robert M. Black Saint Vincent Hospital Laszlo Leb Saint Vincent Hospital Helmut Rennke Harvard Medical School Follow this and additional works at: https://digitalcommons.wustl.edu/open_access_pubs Recommended Citation Edrees, Fahad; Black, Robert M.; Leb, Laszlo; and Rennke, Helmut, ,"Minimal change disease: A case report of an unusual relationship." Saudi Journal of Kidney Diseases and Transplantation.27,4. (2016). https://digitalcommons.wustl.edu/open_access_pubs/5287 This Open Access Publication is brought to you for free and open access by Digital Commons@Becker. It has been accepted for inclusion in Open Access Publications by an authorized administrator of Digital Commons@Becker. For more information, please contact [email protected]. Saudi J Kidney Dis Transpl 2016;27(4):816-820 © 2016 Saudi Center for Organ Transplantation Saudi Journal of Kidney Diseases and Transplantation Case Report Minimal Change Disease: A Case Report of an Unusual Relationship Fahad Edrees1, Robert M. Black2,4,Laszlo Leb3,4, Helmut Rennke5 1Department of Medicine, Division of Nephrology, Washington University School of Medicine, Barnes Jewish Hospital, Saint Louis, MO, 2Division of Renal Medicine and 3Department of Hematology Oncology, Saint Vincent Hospital, 4Reliant Medical Group, Worcester, 5Department of Renal Pathology, Harvard Medical School, Brigham and Women’s Hospital, Boston, MA, USA ABSTRACT. Kidney injury associated with lymphoproliferative disorders is rare, and the exact pathogenetic mechanisms behind it are still poorly understood. Glomerular involvement presen- ting as a nephrotic syndrome has been reported, usually secondary to membranoproliferative glomerulonephritis. -
Minimal Change Glomerulonephritis (GN)
Patient information – Minimal Change Glomerulonephritis Minimal Change Glomerulonephritis (GN) What is it? Your kidney biopsy has shown that your swelling and protein leak (nephrotic syndrome) is caused by a condition called ‘Minimal Change Glomerulonephritis’. This is an inflammation in the glomeruli (the network of blood capillaries) of the kidney, which shows very little change looking down the ordinary microscope. More specialised tests (such as electron microscopy) on the biopsy show characteristic changes to make this diagnosis. It is the commonest cause of nephrotic syndrome in children and causes about a quarter of those in adults. While the symptoms can be quite unpleasant, it does not cause long- term damage to the kidney function. While many types of nephrotic syndrome cannot be treated, Minimal Change GN will respond to steroid treatment. Initial treatment This stops the protein leak in 94 –100% of cases. The main treatment is high dose Prednisolone (steroids) tablets for up to 16 weeks (although usually less time). You will be seen every two weeks, and once the urine is clear of protein, the dose will be gradually reduced over the following six months. Prednisolone 1mg/kg of body weight (max 80mg) daily Lansoprazole 30mg daily Alendronate 70mg weekly Nystatin 1ml four times a day Septrin 480mg daily As steroids may have many side effects, you will also be given additional medication to protect you from some of the more serious ones. Some possible side effects of the steroids · Infection: Steroids make you more prone to ‘opportunist infection’ (so-called, because they only affect vulnerable people). You will be given antibiotics (Septrin and Fluconazole), to protect against thrush and pneumonia.