Health Impact Assessment, Finningley Airport
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Planning Committee
PLANNING COMMITTEE AGENDA Meeting to be held in The Ceres Suite, Worksop Town Hall, S80 2AH on Wednesday, 13th September 2017 at 6.30 p.m. (Please note time and venue) Please turn mobile telephones to silent during meetings. In case of emergency, Members/officers can be contacted on the Council's mobile telephone: 07940 001 705. In accordance with the Openness of Local Government Bodies Regulations 2014, audio/visual recording and photography at Council meetings is permitted in accordance with the Council’s protocol ‘Filming of Public Meetings’. 1 PLANNING COMMITTEE Membership 2017/18 Councillors D. K. Brett, H. Burton, G. Clarkson, S. Fielding, G. Freeman, K. H. Isard, G. A. N. Oxby, D. G. Pidwell, M. W. Quigley, S. Scotthorne, A. K. Smith and T. Taylor. Substitute Members: None Quorum: 3 Members Lead Officer for this Meeting Fiona Dunning Administrator for this Meeting Julie Hamilton NOTE FOR MEMBERS OF THE PUBLIC (a) Please do not take photographs or make any recordings during the meeting without the prior agreement of the Chair. (b) Letters attached to Committee reports reflect the views of the authors and not necessarily the views of the District Council. 2 PLANNING COMMITTEE Wednesday, 13th September 2017 AGENDA 1. APOLOGIES FOR ABSENCE 2. DECLARATIONS OF INTEREST BY MEMBERS AND OFFICERS * (pages 5 - 6) (Members’ and Officers’ attention is drawn to the attached notes and form) (a) Members (b) Officers 3. MINUTES OF MEETING HELD ON 16TH AUGUST 2017 * (pages 7 - 14) 4. MINUTES OF PLANNING CONSULTATION GROUP MEETINGS HELD BETWEEN 17th AND 31ST JULY 2017* (pages 15 - 26) 5. -

Thorne Moors :A Palaeoecological Study of A
T...o"..e MO<J "S " "",Ae Oe COlOOIC'" S T<.OY OF A e"ONZE AGE slTE - .. "c euc~ , A"O a • n ,• THORNE MOORS :A PALAEOECOLOGICAL STUDY OF A BRONZE AGE SITE A contribution to the history of the British Insect fauna P.c. Buckland, Department of Geography, University of Birmingham. © Authors Copyright ISBN ~o. 0 7044 0359 5 List of Contents Page Introduction 3 Previous research 6 The archaeological evidence 10 The geological sequence 19 The samples 22 Table 1 : Insect remains from Thorne Moors 25 Environmental interpretation 41 Table 2 : Thorne Moors : Trackway site - pollen and spores from sediments beneath peat and from basal peat sample 42 Table 3 Tho~ne Moors Plants indicated by the insect record 51 Table 4 Thorne Moors pollen from upper four samples in Sphagnum peat (to current cutting surface) 64 Discussion : the flooding mechanism 65 The insect fauna : notes on particular species 73 Discussion : man, climate and the British insect fauna 134 Acknowledgements 156 Bibliography 157 List of Figures Frontispiece Pelta grossum from pupal chamber in small birch, Thorne Moors (1972). Age of specimen c. 2,500 B.P. 1. The Humberhead Levels, showing Thorne and Hatfield Moors and the principal rivers. 2 2. Thorne Moors the surface before peat extraction (1975). 5 3. Thorne Moors the same locality after peat cutting (1975). 5 4. Thorne Moors location of sites examined. 9 5. Thorne Moors plan of trackway (1972). 12 6. Thorne Moors trackway timbers exposed in new dyke section (1972) • 15 7. Thorne Moors the trackway and peat succession (1977). -

Accreditation Scheme for Museums and Galleries in the United Kingdom: Collections Development Policy
Accreditation Scheme for Museums and Galleries in the United Kingdom: Collections development policy 1 Collections development policy Name of museum: Doncaster Museum Service Name of governing body: Doncaster Metropolitan Borough Council Date on which this policy was approved by governing body: January 24th 2013 Date at which this policy is due for review: January 2018 1. Museum’s statement of purpose The Museum Service primarily serves those living in the Doncaster Metropolitan Borough area and those connected to the King‟s Own Yorkshire Light Infantry* and believes that its purpose can by summed up in four words : Engage, Preserve, Inspire, Communicate * The King‟s Own Yorkshire Light Infantry Museum has its own Collections Development Policy, but is included in the 2013-16 Forward Plan and therefore the Museum Service‟s statement of purpose. 2. An overview of current collections. Existing collections, including the subjects or themes and the periods of time and /or geographic areas to which the collections relate 2.0 At present (2012) the following collections have a member of staff with expertise in that particular field. Social History (including costume and photographs) Archaeology (Including Antiquities) World Cultures Fine and Decorative Arts Other collections are not supported by in-house expertise. For these we would actively look to recruit volunteers or honorary curators with knowledge relevant to these collections. We would also look to apply for grants to take on a temporary staff member to facilitate the curation of these collections. We would also look at accessing external expertise and working in partnership with other organisations and individuals. -

Thorne Inset Campsall and Norton Inset Mexborough Inset Doncaster's
M L B D a S o Elmsa South Elmsall n s e s W ay ll L o T w 496 to Wakefield e T 408 405 For continuation of 301 to Askern 84b to Sykehouse u e n he d n a A Kirk 2 bb L Thorne Road e w a A1 L e n A L 51 B ’s W C a D Kirkton La E 409 407.X45 M 8877 d o A alk C 87a87a Field Lane e services in this area see n E For continuation of a r 6 t g h r Thorne Inset Northgate 3 a e Bramwith a o t h 303 51a n Burghwallis R u o r 8 g a 412 ckley 84 s R h i 301 s r Lan Campsall and Norton inset right r t e h c services in this area 303 a G 84b d 8 r h R 8 Ha L l D t H R 84b ig 303 e o o S 84a a h 8a o ll R a H n n 8787 see Thorne inset right fi c a d t 8a d M 84a e 8 8a 87 87a a St. a 496 d La . a gh s 303 Owston ne 84b z t e e id d 87a87a H 8877 r Thorpe 84 l e d 84 a R l o R n o 301 e R 87a87a d . 87a87a . L a a ne Skellow r d a a in Balne e L M n 301 t L A e s La e Hazel i a Stainforth l 6 t ll . -

Publications List
Doncaster & District Family History Society Publications List August 2020 Parishes & Townships in the Archdeaconry of Doncaster in 1914 Notes The Anglican Diocese of Sheffield was formed in 1914 and is divided into two Archdeaconries. The map shows the Parishes within the Archdeaconry of Doncaster at that time. This publication list shows Parishes and other Collections that Doncaster & District Family History Society has transcribed and published in the form of Portable Document Files (pdf). Downloads Each Parish file etc with a reference number can be downloaded from the Internet using: www.genfair.co.uk (look for the Society under suppliers) at a cost of £6 each. Postal Sales The files can also be supplied by post on a USB memory stick. The cost is £10 each. The price includes the memory stick, one file and postage & packing. (The memory stick can be reused once you have loaded the files onto your own computer). Orders and payment by cheque through: D&DFHS Postal Sales, 18 Newbury Way, Cusworth, Doncaster, DN5 8PY Additional files at £6 each can be included on a single USB memory stick (up to a total of 4 files depending on file sizes). Example: One USB memory stick with “Adlingfleet” Parish file Ref: 1091 = £10. 1st Additional file at £6: the above plus “Adwick le Street” Ref: 1112 = Total £16. 2nd Additional file at £6: “The Poor & the Law” Ref: 1125 = Total £22 Postage included. We can also arrange payment by BACs, but for card and non-sterling purchases use Genfair While our limited stocks last we will also supply files in the form of a CD at £6 each plus postage. -

FINNINGLEY QUARRY EXTENSION Finningley Proposed 56 Hectare
FINNINGLEY QUARRY EXTENSION Finningley Proposed 56 hectare Extension Landscape and Visual Impact Assessment December 2013 FINNINGLEY QUARRY EXTENSION Finningley Proposed 56 hectare Extension Landscape and Visual Impact Assessment December 2013 Prepared by: Sarah Brooks CMLI Brooks Landscape Architecture Tel: 07582 470459 Email: [email protected] Prepared for: Lafarge Tarmac Southfield Lane Whitwell Worksop Nottinghamshire S80 3LJ © Sarah Brooks 2013 No part of this document may be reproduced by any means without the prior permission of the author. Finningley Quarry Extension - Landscape and Visual Impact Assessment BLA _______________________________________________________________________________________ FINNINGLEY QUARRY EXTENSION Finningley Proposed 56 hectare Extension Landscape and Visual Impact Assessment December 2013 CONTENTS 1.1 Introduction 1 1.2 Approach and Methods 1 1.3 Site Description and Development Proposals 4 1.4 Regulatory / Policy Framework 7 1.5 Baseline Conditions 12 1.6 Potential Effects and Mitigation 22 1.7 Significance of Landscape and Visual Effects 24 1.8 Summary 27 Appendix 1 Landscape and Visual Assessment Criteria Appendix 2 Landscape Impact Assessment Table Appendix 3 Visual Impact Assessment Table Appendix 4 Figures and Plates Figure 1 Landscape Context Figure 2 Landscape Character Figure 3 Visual Impact Assessment Plates 1 to 5 Viewpoints 1 to 10 _____________________________________________________________________________________ LVIA report (finala)/ December 2013 Finningley Quarry Extension - Landscape and Visual Impact Assessment BLA _______________________________________________________________________________________ 1.1 Introduction 1.1.1 A landscape and visual impact assessment (LVIA) has been undertaken as part of an Environmental Impact Assessment (EIA) to accompany a planning application by LafargeTarmac (the Applicant) for a 56 hectare (ha) extension to the existing Finningley Quarry sand and gravel pit (also referred to as the ‘Application Area’) near Doncaster. -

The Doncaster Green Infrastructure Strategy 2014- 2028
The Doncaster Green Infrastructure Strategy 2014- 2028 Creating a Greener, Healthier & more Attractive Borough Adoption Version April 2014 Doncaster Council Service Improvement & Policy (Regeneration & Environment) 0 1 the potential of the Limestone Valley, which runs through the west of the borough. Did you know that Doncaster has 65 different woodlands which cover an area in excess of 521 hectares? That’s about the equivalent to over 1,000 football pitches. There are 88 different formal open spaces across the borough, which include football, rugby and cricket pitches, greens, courts and athletics tracks. Doncaster is also home to 12 golf courses. The Trans-Pennine Trail passes through Doncaster and is integral to the extensive footpath and cycle network that link the borough’s communities with the countryside, jobs and recreation opportunities. There are so Foreword from the many more features across Doncaster and these are covered within this Strategy document. Portfolio Holder… Despite this enviable position that communities in Doncaster enjoy, there is always so much more that can be done to make the borough’s GI even greater. The Strategy sets out a framework As Portfolio Holder for Environment & Waste at for ensuring maximum investment and funding Doncaster Council, I am delighted to introduce is being channelled, both by the Council and the the Doncaster Green Infrastructure Strategy vast array of important partners who invest so 2014-2028: Creating a Greener, Healthier & much time and resources, often voluntarily, into more Attractive Borough. making our GI as good as it can be. As the largest metropolitan Borough in the This Strategy will help deliver a better country, covering over 220 square miles, connected network of multi-purpose spaces and Doncaster has an extensive green infrastructure provide the opportunity for the coordination (GI) network which includes numerous assets and delivery of environmental improvements and large areas that are rural in character. -

Ecological Baseline Survey of Land at Finningley Quarry, South Yorkshire / Nottinghamshire LAF.FQ Lafarge Aggregates
Lafarge Aggregates Ltd ECOLOGICAL BASELINE SURVEY OF LAND AT FINNINGLEY QUARRY, SOUTH YORKSHIRE / NOTTINGHAMSHIRE FINAL- VERSION 2 FEBRUARY 2014 ESL (Ecological Services) Ltd, 1 Otago House, Allenby Business Village, Crofton Road, Lincoln, LN3 4NL Ecological Baseline Survey of Land at Finningley Quarry, South Yorkshire / Nottinghamshire LAF.FQ Lafarge Aggregates DOCUMENT CONTROL TITLE: Ecological Baseline Survey of Land at Finningley Quarry, South Yorkshire / Nottinghamshire VERSION: Final – Version 2 DATE: February 2014 ISSUED BY: Brian Hedley AUTHORS: Peter Morrell and Brian Hedley CHECKED BY: Andrew Malkinson APPROVED BY: Vanessa Tindale ISSUED TO: David Park Restoration Manager Lafarge Aggregates Ltd Thrislington Quarry West Cornforth County Durham DL17 9EY Paul Clarke David L Walker Limited Albion House 89 Station Road Eckington Sheffield S21 4FW This report has been prepared by ESL with all reasonable skill, care and diligence, within the terms of the contract with the Client. The report is confidential to the Client. ESL accepts no responsibility of whatever nature to third parties to whom this report may be made known. No part of this document may be reproduced without the prior written approval of ESL. ESL (Ecological Services) Ltd, 1 Otago House, Allenby Business Village, Crofton Road, Lincoln, LN3 4NL Ecological Baseline Survey of Land at Finningley Quarry, South Yorkshire / Nottinghamshire LAF.FQ Lafarge Aggregates CONTENTS Page 1 INTRODUCTION 1 2 DESK STUDY 1 3 HABITATS, PLANT COMMUNITIES AND PLANT SPECIES 3 3.1 Survey Methods -

FINNINGLEY QUARRY EXTENSION, (Phases 25, 26, 27, 29 & 30) FINNINGLEY, SOUTH YORKSHIRE and MISSON, NOTTINGHAMSHIRE
FINNINGLEY QUARRY EXTENSION, (Phases 25, 26, 27, 29 & 30) FINNINGLEY, SOUTH YORKSHIRE AND MISSON, NOTTINGHAMSHIRE An Archaeological Desktop Assessment for Lafarge Aggregates Ltd Authors: L.Elliott, L.Platt & Peter Webb 2012 (Revised 2013) © Trent and Peak Archaeology Code: FME North Nottinghamshire and Finningley 1610 Trent & Peak Archaeology © Unit 1, Holly Lane Chilwell Nottingham NG9 4AB 0115 8967400 (Tel.) 0115 925 9464 (Fax.) Trent & Peak Archaeology is a trading name of York Registered Office: A Company Limited by Guarantee Archaeological Trust Registered Charity in England and 47 Aldwark, York YO1 7BX Without Share Capital Registered Wales (No. 509060) and Scotland (No. SCO42846) in England No. 1430801 Finningley Quarry Extension 2012 SUMMARY This report comprises an assessment of the archaeological potential for the proposed areas of extraction at Finningley Quarry in line with best practice recommended within the National Planning Policy Framework Section 12 (March 2012). The five proposed extensions fall within the parishes of Finningley, South Yorkshire (phases 26, 27, 30 & part of 29) and Misson, Nottinghamshire (Phase 25 & most of 29). Phase 28 to be crossed by the haulage route to the plant site (and the subject of previous evaluation), also lies in Finningley parish, South Yorkshire. One designated heritage asset listed on the South Yorkshire SMR (SMR01832) comprising three flints and one heritage asset listed on the NMR (320789) comprising thirty flints lie within phase 26 of the proposed extension. No heritage assets listed on the Nottinghamshire HER are present within the proposed extension phases. Within the wider study area of the existing quarry and adjacent areas a number of heritage assets or themes were assessed as holding significant archaeological potential, necessitating further consideration. -
7 March 2005 3. Title: Response To
ROTHERHAM BOROUGH COUNCIL – REPORT TO MEMBERS 1. Meeting: Economic and Development Cabinet Member Delegated Powers Meeting 2. Date: 7 March 2005 3. Title: Response to the Coalfields Communities Campaign regarding the Finningley and Rossington Regeneration Route Scheme 4. Programme Area: Economic and Development Services/Chief Executive’s Office 5. Summary A request has been received from the Coalfield Communities Campaign asking for Rotherham’s views on the Finningley and Rossington Regeneration Route Scheme (FARRRS) in Doncaster. The report sets out the background and concludes that only qualified support can be given at this time. 6. Recommendations That: (a) the Council offer its qualified support to FARRRS for the reasons given in the report, and (b) a copy of this report is forwarded to Councillor S. Wright as Rotherham’s representative on the CCC. 7. Proposals and Details At the Coalfields Communities Campaign (CCC) meeting on the 21 January 2005, Doncaster Metropolitan Borough Council (DMBC) asked for the support of CCC for DMBC’s efforts to secure funding and planning approval for the Finningley and Rossington Regeneration Routes Schemes (FARRRS). Members asked for more information before taking a view and a briefing note was subsequently issued by DMBC (attached at Appendix A). The FARRRS project will provide a link road from junction 3 of the M18 motorway into Rossington and on to the Robin Hood Doncaster Sheffield Airport. It aims to facilitate the regeneration of the south east area of Doncaster and in due course enable the airport to expand. The briefing note supplied by Doncaster lists the benefits of the road scheme to the coalfield communities as follows: • Improves and enhances the growth of the airport and its role as a transformation project which assists the economic restructuring of the sub- region including numerous coalfield communities. -
Doncaster Local Plan: Archaeological Scoping Assessment
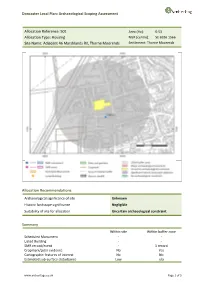
Doncaster Local Plan: Archaeological Scoping Assessment Allocation Reference: 501 Area (Ha): 0.53 Allocation Type: Housing NGR (centre): SE 6936 1566 Site Name: Adjacent 46 Marshlands Rd, Thorne Moorends Settlement: Thorne Moorends Allocation Recommendations Archaeological significance of site Unknown Historic landscape significance Negligible Suitability of site for allocation Uncertain archaeological constraint Summary Within site Within buffer zone Scheduled Monument - - Listed Building - - SMR record/event - 1 record Cropmark/Lidar evidence No Yes Cartographic features of interest No No Estimated sub-surface disturbance Low n/a www.archeritage.co.uk Page 1 of 3 Doncaster Local Plan: Archaeological Scoping Assessment Allocation Reference: 501 Area (Ha): 0.53 Allocation Type: Housing NGR (centre): SE 6936 1566 Site Name: Adjacent 46 Marshlands Rd, Thorne Moorends Settlement: Thorne Moorends Site assessment Known assets/character: The SMR does not record any features within the site. One findspot is recorded within the buffer zone, a Bronze Age flint arrowhead. No listed buildings or Scheduled Monuments are recorded within the site or buffer zone. The Magnesian Limestone in South and West Yorkshire Aerial Photographic Mapping Project records levelled ridge and furrow remains within the buffer zone. The Historic Environment Characterisation records the present character of the site as modern commercial core- suburban, probably associated with the construction of Moorends mining village in the first half of the 20th century. There is no legibility of the former parliamentary enclosure in this area. In the western part of the buffer, the landscape character comprises land enclosed from commons and drained in 1825, with changes to the layout between 1851 and 1891 in association with the construction of a new warping system. -

Blaxton-Pc 10 10 2019 Redacted
The following message has been applied automatically, to promote news and information from Nottinghamshire County Council about events and services: Got a question about recycling in Nottinghamshire? Check out our Check out our frequently asked questions. #RecycleForNotts Emails and any attachments from Nottinghamshire County Council are confidential. If you are not the intended recipient, please notify the sender immediately by replying to the email, and then delete it without making copies or using it in any other way. Senders and recipients of email should be aware that, under the Data Protection Act 2018 and the Freedom of Information Act 2000, the contents may have to be disclosed in response to a request. Although any attachments to the message will have been checked for viruses before transmission, you are urged to carry out your own virus check before opening attachments, since the County Council accepts no responsibility for loss or damage caused by software viruses. You can view our privacy notice at: https://www.nottinghamshire.gov.uk/global-content/privacy Nottinghamshire County Council Legal Disclaimer. 2 PARISH COUNCILS OF AUCKLEY, BLAXTON, BRANTON-WITH-CANTLEY AND FINNINGLEY (ALL PART OF DMBC FINNINGLEY WARD). JOINT COMMENTS IN RESPONSE TO CONSULATION ON THE NOTTINGHAMSHIRE COUNTY COUNCIL DRAFT MINERALS PLAN. Summary In isolation the proposals to develop sites at Austerfield, Misson, Barnby Moor and Scrooby seem innocuous, however when considered alongside existing and proposed developments in both Nottinghamshire and the DMBC area, we have serious concerns about the impact on our communities, particularly the potential increase in Heavy Goods and other vehicles on an already busy road network in and around our villages.