Refraction As a Basis for Screening Children for Squint and Amblyopia R
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Advanced Anatomy & Physiology of The
By Diane F. Drake, LDO, ABOM, NCLEM, FNAO Introduction Terminology Presbyopia Anatomy Muscle Imbalances Refractive Errors Unequal refractive errors Spherical Correction Visualizing the Rx Cylindrical Correction Visual Angle and Minimum Visual Angle Minimum Visual Angle Visual Angle Subtend To extend under or to be opposite to The angle which is opposite the object being observed Minimum Detail The detail that must be detected on an object to positively identify or distinguish the object Minimum Detail E Minimum Detail Resolution The ability to detect minimum detail The resolving power of the normal eye is a minimum visual angle of 1 minute E The minimum visual angle of the letter is 1 minute The visual angle of the letter is 5 minutes Visual Acuity The measure of the angle subtended by the outer limits of rays of light coming from the minimum detail of an object as they enter the eye 20/20 or 6/6 Snell’s Law of Refraction n1 sin i = n2 sin r The Snellen Fraction The distance at which the test is made divided by the distance at which the smallest letter read subtends an angle of 5 minutes Snellen Letters Snellen Letters Minimum Angle of Resolution Landolt Ring (C) and the Illiterate E Contrast Sensitivity Terminology Emmetropia Ametropia Myopia Hyperopia Terminology Astigmatism Simple myopic Corneal astigmatism astigmatism Lenticular astigmatism Compound myopic Regular astigmatism astigmatism Irregular astigmatism Simple hyperopic astigmatism Compound hyperopic astigmatism Terminology Presbyopia Greek Presby -

Guidelines for Universal Eye Screening in Newborns Including RETINOPATHY of Prematurity
GUIDELINES FOR UNIVERSAL EYE SCREENING IN NEWBORNS INCLUDING RETINOPATHY OF PREMATURITY RASHTRIYA BAL SWASthYA KARYAKRAM Ministry of Health & Family Welfare Government of India June 2017 MESSAGE The Ministry of Health & Family Welfare, Government of India, under the National Health Mission launched the Rashtriya Bal Swasthya Karyakram (RBSK), an innovative and ambitious initiative, which envisages Child Health Screening and Early Intervention Services. The main focus of the RBSK program is to improve the quality of life of our children from the time of birth till 18 years through timely screening and early management of 4 ‘D’s namely Defects at birth, Development delays including disability, childhood Deficiencies and Diseases. To provide a healthy start to our newborns, RBSK screening begins at birth at delivery points through comprehensive screening of all newborns for various defects including eye and vision related problems. Some of these problems are present at birth like congenital cataract and some may present later like Retinopathy of prematurity which is found especially in preterm children and if missed, can lead to complete blindness. Early Newborn Eye examination is an integral part of RBSK comprehensive screening which would prevent childhood blindness and reduce visual and scholastic disabilities among children. Universal newborn eye screening at delivery points and at SNCUs provides a unique opportunity to identify and manage significant eye diseases in babies who would otherwise appear healthy to their parents. I wish that State and UTs would benefit from the ‘Guidelines for Universal Eye Screening in Newborns including Retinopathy of Prematurity’ and in supporting our future generation by providing them with disease free eyes and good quality vision to help them in their overall growth including scholastic achievement. -

Anatomy & Physiology of The
Anatomy & Physiology of The Eye 2017-2018 Done By: 433 Team Abdullah M. Khattab Important Doctor’s Notes Extra Abdullah AlOmair Resources: Team 433, Doctors Notes, Vaughan & Asbury’s General ophthalmology. Editing File Embryology of The Eye ............................................................................................. 2 ● Defects: ........................................................................................................................... 2 Development of The Eye After Birth .......................................................................... 3 ● Refractive power depends on two factors: ...................................................................... 3 The Orbit ................................................................................................................... 4 ● Seven bones contribute the bony orbit and surrounded by nasal sinuses. .................... 4 ● The orbital wall, pear-like shaped, formed by: ................................................................ 4 ● Structures Passing Through the Optic Openings: ........................................................... 4 Extraocular Muscles .................................................................................................. 1 ● Anatomy .......................................................................................................................... 1 ● Notes: .............................................................................................................................. 1 ● Field of action: -

Disclosure Ocular Anatomy and Motility Ocular Anatomy Overview the Human Vision System the Human Vision System Lids and Lacrimal
10/19/2012 Disclosure Ocular Anatomy and Motility Jenean Carlton BA, ABOC, NCLC 9President, Carlton & Associates, LLC – Carlton and Associates, 6 Course #214 Monterey Symposium LLC provides communications and educational materials for the optical industry 9Contributing Editor for Refractive Eyecare magazine. 6 Jenean Carlton BA, ABOC, NCLC 9Contributing Author Eyecare Business magazine. 9Communications Committee member OWA. 9Has been in the optical industry for 30 years with more than half of this time working in practices. 9Vision Monday’s Most Influential Women Award in Optical 2005 1 Ocular Anatomy Overview The Human Vision System 9 The eye is an amazing organ that works like a camera. 9 Think of the cornea and crystalline lens as the lenses of a camera, the iris as the shutter, and the retina as the photographic film. The Human Vision System Lids and Lacrimal System Vision takes place in the occipital lobe of The tear film has 3 layers: the brain Outer: the lipid layer (meibomian 9The brain can be glands in lids) is the oil layer. thought of as the development Middle: the aqueous layer center because it (lacrimal glands) is mainly water and provides oxygen converts and nutrients. electrical signals from the retina Inner: the mucin layer (goblet cells in conjunctiva) helps the tears into vision. adhere to the cornea. It is the mucus layer. 1 10/19/2012 Dry Eye Syndrome Lid Disorders What causes dry eyes? Ectropion= Out Treatments Entropion= In Ptosis- a drooping of the lid. Lids can have other problems too like turning out, in. Lids Disorders Lid Disorders Blepharitis is a chronic Hordeolum (stye) - inflammation- not an acute inflammation of a infection. -
Squints Occur When the Eyes Do Not Work As a Team
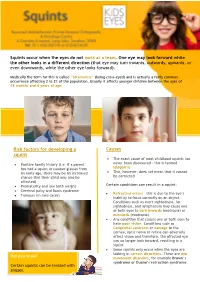
Squints occur when the eyes do not work as a team. One eye may look forward while the other looks in a different direction (that eye may turn inwards, outwards, upwards, or even dow nwards, while the other eye looks forward). Medically the term for this is called “Strabismus” (being cross-eyed) and is actually a fairly common occurrence affecting 2 to 3% of the population. Usually it affects younger children between the ages of 18 months and 4 years of age. Risk factors for developing a Causes squint • The exact cause of most childhood squints has • Positive family history (i.e. if a parent never been discovered – this is termed has had a squint or needed glasses from idiopathic an early age, there may be an increased • This, however, does not mean that it cannot chance that their child may also be be corrected affect ed) • Prematurity and low birth weight Certain conditions can result in a squint: • Cerebral palsy and Down syndrome • Refractive errors – this is due to the eye’s • Tumours (in rare cases) inability to focus correctly on an object. Conditions such as short sightedness, far sightedness, and astigmatism may cause one or both eyes to turn inwards (esotropia) or outwards (exotropia). • Any condition that causes one or both eyes to have poor vision. Conditions such as Congenital cataracts or damage to the cornea, optic nerve or retina can adversely affect vision and therefore, the affected eye can no longer look forward, resulting in a squint • Some squints only occur when the eyes are looking in certain directions. -

Squint (Strabismus)
What is a Squint? What can cause a squint? Treatment Your Orthoptist is available to As not all squints are the same, In some cases there may be no answer any further questions treatment will vary from case to obvious reason for a squint. about childhood squints, and case, and your Orthoptist will However, often a squint is due to a relate specifically to your case as keep you informed. The majority variety of reasons such as: required. of cases require a combination of the following: A Squint affects the positioning of Congenital the eyes, and often prevents both A congenital squint means a child Glasses eyes working together as a pair. has been born with a squint. A glasses test will be performed by Types of Squints Need for Glasses the hospital Optometrist. To Some children may be long-sighted achieve the most accurate results, and need glasses. The child over eye drops are used at this appointment. If a need for glasses is Not all squints are the same. Squints focuses to see clearly without the found, these are given for full time may be constant, they may be there glasses and the effort required doing wear to improve the child’s eyesight. all the time, or they can be this can lead to one eye Glasses may also improve the intermittent. turning/squinting. position of the eyes, and correct or A squinting eye may turn inwards Children can also be short sighted, improve the squint. towards the nose, or turn outwards. which occasionally leads to a squint. -
Squint Information Booklet
Squint Your Questions Answered Patient Information Leaflet RVEEH, Squint January2014. Ref No: PIL 023 Version 2 What is a Squint? A squint, or strabismus, occurs when the eyes are misaligned and are no longer working as a pair. It is common in childhood, affecting 2-3% of the population. The most common types of squint occur when one eye turns inwards (a convergent squint, or esotropia), or outwards (known as a divergent squint, or exotropia). However, it is also possible to have a vertical squint (hyper- or hypotropia) or even a torsional squint, where the eye is rotated inwards or outwards. Squints in childhood should be treated early to avoid amblyopia (see below) and to try to preserve binocular vision. What causes a squint? There are many different types of squint. Childhood squints are often caused by a need for glasses. Convergent squints are the most common type and these are usually caused by hyperopia, or long-sightedness, where the effort required by the child to over-focus the eyes eventually causes one of them to turn in. The hyperopia is present since birth, but the squint usually develops between the ages of 18 months to 3 years. Esotropia in the left eye. When the long-sightedness is corrected, the eyes become straight RVEEH, Squint January2014. Ref No: PIL 023 Version 2 Childhood squints can be hereditary. They often start off intermittently, especially when the child is tired or unwell. They never go away on their own, but they do often improve with time. Occasionally, they require surgery. Rarely, squints can be caused by defects at the back, or behind the eye. -

Single Vision During Ocular Deviation in Intermittent Exotropia Ignacio Serrano-Pedraza1, Michael P Clarke1,2 and Jenny CA Read1
Ophthalmic & Physiological Optics ISSN 0275-5408 REVIEW Single vision during ocular deviation in intermittent exotropia Ignacio Serrano-Pedraza1, Michael P Clarke1,2 and Jenny CA Read1 1Institute of Neuroscience, Faculty of Medical Sciences, Newcastle University, Newcastle upon Tyne, UK and 2Eye Department, Royal Victoria Infirmary, Newcastle upon Tyne, UK Citation information: Serrano-Pedraza I, Clarke MP & Read JCA. Single vision during ocular deviation in intermittent exotropia. Ophthalmic Physiol Opt 2011, 31, 45–55. doi: 10.1111/j.1475-1313.2010.00805.x Keywords: anomalus retinal correspondence, Abstract anti-diplopic mechanisms, diplopia, intermittent exotropia, strabismus, Intermittent exotropia is a common oculomotor anomaly where one eye inter- suppression mittently deviates outwards. Patients with this type of strabismus are often not aware of the exodeviation and do not usually experience diplopia. In this Correspondence: Ignacio Serrano-Pedraza review, we discuss what is known about the cortical mechanisms which achieve E-mail address: [email protected] single vision during exodeviation in this condition, and highlight some outstanding questions. Received: 4 August 2010; Accepted: 14 October 2010 binocular visual function, especially for near viewing. Introduction Indeed, their stereoacuity at near distances appears to be Intermittent exotropia [X(T)] is a disorder of binocular completely normal.5,6 eye movement control, in which one eye intermittently At far distance (6 m) stereoacuity in some patients is turns outwards, as in Figure 1. The exodeviation is most worse than that of controls.6 However, this does not likely to occur at far viewing distances, when the oculo- appear to reflect a problem with combining the two eyes’ motor convergence drive is weakest, and occurs most images in visual cortex. -

Pupillary Responses in Amblyopia Br J Ophthalmol: First Published As 10.1136/Bjo.74.11.676 on 1 November 1990
676 BritishlournalofOphthalmology, 1990,74,676-680 Pupillary responses in amblyopia Br J Ophthalmol: first published as 10.1136/bjo.74.11.676 on 1 November 1990. Downloaded from Alison Y Firth Abstract light was then alternatively switched from one Relative afferent pupillary defects (RAPD) eye to the other, giving a period of stimulation of were detected in 32*3% ofpatients with ambly- 1 to 2 seconds, and the initial pupillary con- opia by a modification ofthe swinging flashlight striction was observed. The light was then left in test and the synoptophore. After consideration front ofeach eye for a count of3 and the pupillary ofvarious clinical investigations the significant escape noted. factors identified in patients showing a RAPD If a pupillary defect was observed, a neutral were: anisometropia, early age of onset where density filter was placed in the arm of the strabismus was present, level of visual acuity synoptophore in front of the eye without the following treatment, longer period ofocclusion defect. In practice it was not found possible to therapy. These points bear similarities to the quantify the defect to within 0-1 log unit as has results of pattern electroretinograms (PERG) previously been reported,5 but merely to confirm in amblyopes, and the possibility of the its presence. Where no defect was initially causative defect being at ganglion cell level is apparent, a 0-3 log unit NDF was placed in discussed. The effect of occlusion treatment either arm in turn to produce a difference in cannot be predicted from the presence or response. In some cases this revealed a subtle absence of a RAPD. -

Your Child's Squint Surgery
Patient and Carer Information Your Child’s Squint Surgery What is a squint? A squint or strabismus occurs when the eyes are not aligned properly, e.g. one eye may turn inwards, outwards, up or down. A convergent squint refers to an eye that turn inwards, and a divergent squint refers to an eye that turn outwards. Sometimes one eye may be higher or lower than the other (vertical squint). The squint may be constant (present at all times) or occur only intermittently. Most squints are managed by prescribing appropriate glasses and in some cases patching to improve vision in the squinting eye. The aim of squint surgery in most cases is to straighten the eyes, to give a better cosmetic appearance or to correct a head posture. Surgery can sometimes improve the ability of the two eyes to work together as a pair and provide better quality vision. Surgery does not eliminate the need for glasses and does not correct your child’s vision. Two weeks prior to your child’s surgery, you will meet with the Orthoptist and the Ophthalmologist. The squint will be re-measured. You will have the opportunity to discuss the surgery and ask further questions. You will sign a consent form. We will not perform the operation if your child has a cough or cold. The operation will be deferred for at least two weeks to allow a full recovery. Please inform Woodlands ward if your child is unwell. Squint Surgery During Squint surgery, the position of one or more eye muscles is changed. -

Strabismus ,Amblyopia & Leukocoria
Strabismus ,Amblyopia & Leukocoria Objectives: ● Not given [ Color index : Important | Notes | Extra ] Resources: Slides + 434 team + Notes Done by : Abdulrahman Al-Shammari, Farrah Mendoza Revised by : Adel Al Shihri, Lina Alshehri. Abbreviations you need to know: A or Acc: ET: Esotropia X: Exophoria EOM: Extraocular accommodation XT: Exotropia BLP: Bare light movements AC/A: Accommodative X(T): Intermittent perception PD: Prism diopter convergence/accommod exotropia Va: Visual acuity BLR: Bilateral rectus ation ratio HT: Hypertropia PTO: Part-time occlusion muscle N or D: Near and distant HPO: Hypotropia RD: Retinal detachment R&R: Recess and vision resection Strabismus: ● Strabismus is ocular misalignment ● 2%-3% of children and young adults. ● Incidence is equal in males and females. ■ Strabismus:(Abnormal alignment of the eyes, the condition of having a squint). ■ A strabismus can be tropia or phoria ■ Tropia: misalignment that is always there, even when both eyes are open and attempting to work together. Large angle deviations are obvious. If small angle, you can detect it with the Cover-Uncover test. ■ Phoria: misalignment that only occurs some of the time, usually under conditions of stress, illness, fatigue or when binocular vision is interrupted i.e. when the two eyes are no longer looking at the same object such as when the synchronization between the eyes is broken by covering one eye. You can “break fusion” using the Cross-Cover test. Causes : 1. Inherited pattern. Most patients fall under this category, so it is important to ask about family history. 2. Idiopathic. 3. Neurological conditions (cerebral palsy, hydrocephalus & brain tumors). 4. Down syndrome. 5. -

Severity of Amblyopia and Its Correlation with the Amount of Refractive Error
84 Ophthalmol Ina (2015) 41:1 Original Article Severity of Amblyopia and Its Correlation with The Amount of Refractive Error Ria Sandy Deneska Refraction and Contact Lens Division, Department of Ophthalmology, Faculty of Medicine Airlangga University/ dr Soetomo General Hospital, Surabaya ABSTRACT Background: To analyze the correlation between the severity of amblyopia and the amount of refractive error Methods: Patients in outpatient clinic dr Soetomo General Hospital, who was diagnozed as amblyopia, from November 2011 – January 2013, were enrolled in this retrospective study. All subjects were evaluated for subjective refraction using Snellen Chart and objective refraction using streak retinoscopy. The severity of amblyopia determined by the BCVA and the amount of refractive error stated by the spherical equivalent and the amount of cylindrical errors. Result: The subjects of this study was 40 patients (73 eyes) with age 5-11 years old. The range of BCVA was 0,1-0,8 logMAR units, the spherical equivalent of refractive errors were minus 1,5D – 12,75D and the cylindrical errors were minus 0,50 – 5,00D. Statistically, there was correlation between the severity of amblyopia and the spherical equivalent of refractive errors, but there was no correlation with the cylindrical errors. Conclusion: The severity of amblyopia has a correlation with the amount of spherical equivalent of refractive error, but has no correlation with the amount of astigmatism. Key words: Amblyopia, Spherical Equivalent, Cylindrical Error Amblyopia, also referred by the public as “lazy following: strabismus, anisometropia or high eye”, is a unilateral or, less commonly, bilateral bilateral refractive errors (isometropia), and reduction of best-corrected visual acuity that stimulus deprivation (Rouse et al 1994, Raab et al cannot be attributed directly to the effect of any 2011, Gunawan 2012).