The Management of Squint
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Official Scientific Journal of the Delhi Ophthalmologycal Society DJO Vol
DJO Vol.20, No. 2, October-December 09 DJO Vol.20, No. 2, October-December 09 October-December 2, No. Vol.20, DJO The Official Scientific Journal of the Delhi Ophthalmologycal Society DJO Vol. 20, No. 2, October-December, 2009 Delhi Journal of Ophthalmology Editor Editorial Board Rohit Saxena Rajvardhan Azad Ramanjit Sihota Managing Editor Vimla Menon Divender Sood Rajesh Sinha Atul Kumar Rishi Mohan Ashok K Grover Namrata Sharma Editorial Committee Mahipal S Sachdev Tanuj Dada Parijat Chandra M.Vanathi Lalit Verma Rajinder K hanna Tushar Agarwal Prakash Chand Agarwal Sharad Lakhotia Harbans Lal Chandrashekhar Kumar Swati Phuljhele P V Chaddha Amit Khosla Shibal Bhartiya Reena Sharma Dinesh Talwar B Ghosh Munish Dhawan Twinkle Parmar K.P.S Malik Kirti Singh Harinder Sethi Varun Gogia Pradeep Sharma B P Guliani Raghav Gupta Sashwat Ray V P Gupta S P Garg Ashish Kakkar Saptrishi Majumdar S. Bharti Arun Baweja General Information Delhi Journal of Ophthalmology (DJO), once called Visiscan, is a quarterly journal brought out by the Delhi Opthalmological Society. The journal aims at providing a platform to its readers for free exchange of ideas and information in accordance with the rules laid out for such publication. The DJO aims to become an easily readable referenced journal which will provide the specialists with up to date data and the residents with articles providing expert opinions supported with references. Contribution Methodology Delhi Journal of Opthalmology (DJO) is a quarterly journal. Author/Authors must have made significant contribution in carrying out the work and it should be original. It should be accompanied by a letter of transmittal. -

Duane Retraction Syndrome
Med. J. Cairo Univ., Vol. 78, No. 1, June: 331-336, 2010 www.medicaljournalofcairouniversity.com Duane Retraction Syndrome KARIMA L. SHALABY, M.D.* and MOSTAFA BAHGAT, M.D.** The Pediatric Ophthalmology Section*, Tripoli Eye Hospital and the Department of Ophthalmology**, Faculty of Medicine, Cairo University. Abstract Electromyography studies have shown paradox- ical innervations of Lateral rectus muscle and Purpose of Study: To evaluate and to manage if manage- anomalous synergistic innervations of medial rec- ment indicated for cases of Duane retraction syndrome. tus, inferior rectus, superior rectus and oblique Patients and Methods: 15 Duane retraction syndrome muscles [7,8] . (DRS) patients seen in Pediatric clinic in Tripoli Eye Hospital in period from January 2006-December 2006. Complete In most cases of DRS the entire 6 th nerve atro- ophthalmic examination including ortho-optic assessment for phy instead of post half of 6 th nerve (without all cases. specific teratogenic stimulus) 95% of DRS cases Results: Patients age ranged 1 year to 20 years in this this is the only initial abnormality. In about 5% of group of study, females were affected more than males with cases other abnormalities seen (e.g. nerve deafness). 2 to 1 ratio. Type 1 (esotropic) is the most common 80% of cases. Left eye was affected more than right eye. Bilateral in Most cases of DRS are sporadic [5,9] . 13.3% of cases. DRS clinical picture varies widely, surgical intervention will not eliminate the abnormality but will lessen Etiology: it. Two cases were operated upon to improve alignment in Etiology of DRS has been proposed by several primary position. -

G:\All Users\Sally\COVD Journal\COVD 37 #3\Maples
Essay Treating the Trinity of Infantile Vision Development: Infantile Esotropia, Amblyopia, Anisometropia W.C. Maples,OD, FCOVD 1 Michele Bither, OD, FCOVD2 Southern College of Optometry,1 Northeastern State University College of Optometry2 ABSTRACT INTRODUCTION The optometric literature has begun to emphasize One of the most troublesome and long recognized pediatric vision and vision development with the advent groups of conditions facing the ophthalmic practitioner and prominence of the InfantSEE™ program and recently is that of esotropia, amblyopia, and high refractive published research articles on amblyopia, strabismus, error/anisometropia.1-7 The recent institution of the emmetropization and the development of refractive errors. InfantSEE™ program is highlighting the need for early There are three conditions with which clinicians should be vision examinations in order to diagnose and treat familiar. These three conditions include: esotropia, high amblyopia. Conditions that make up this trinity of refractive error/anisometropia and amblyopia. They are infantile vision development anomalies include: serious health and vision threats for the infant. It is fitting amblyopia, anisometropia (predominantly high that this trinity of early visual developmental conditions hyperopia in the amblyopic eye), and early onset, be addressed by optometric physicians specializing in constant strabismus, especially esotropia. The vision development. The treatment of these conditions is techniques we are proposing to treat infantile esotropia improving, but still leaves many children handicapped are also clinically linked to amblyopia and throughout life. The healing arts should always consider anisometropia. alternatives and improvements to what is presently The majority of this paper is devoted to the treatment considered the customary treatment for these conditions. -

Sixth Nerve Palsy
COMPREHENSIVE OPHTHALMOLOGY UPDATE VOLUME 7, NUMBER 5 SEPTEMBER-OCTOBER 2006 CLINICAL PRACTICE Sixth Nerve Palsy THOMAS J. O’DONNELL, MD, AND EDWARD G. BUCKLEY, MD Abstract. The diagnosis and etiologies of sixth cranial nerve palsies are reviewed along with non- surgical and surgical treatment approaches. Surgical options depend on the function of the paretic muscle, the field of greatest symptoms, and the likelihood of inducing diplopia in additional fields by a given procedure. (Comp Ophthalmol Update 7: xx-xx, 2006) Key words. botulinum toxin (Botox®) • etiology • sixth nerve palsy (paresis) Introduction of the cases, the patients had hypertension and/or, less frequently, Sixth cranial nerve (abducens) palsy diabetes; 26% were undetermined, is a common cause of acquired 5% had a neoplasm, and 2% had an horizontal diplopia. Signs pointing aneurysm. It was noted that patients toward the diagnosis are an who had an aneurysm or neoplasm abduction deficit and an esotropia had additional neurologic signs or increasing with gaze toward the side symptoms or were known to have a of the deficit (Figure 1). The diplopia cancer.2 is typically worse at distance. Measurements are made with the Anatomical Considerations uninvolved eye fixing (primary deviation), and will be larger with the The sixth cranial nerve nuclei are involved eye fixing (secondary located in the lower pons beneath the deviation). A small vertical deficit may fourth ventricle. The nerve on each accompany a sixth nerve palsy, but a side exits from the ventral surface of deviation over 4 prism diopters the pons. It passes from the posterior Dr. O’Donnell is affiliated with the should raise the question of cranial fossa to the middle cranial University of Tennessee Health Sci- additional pathology, such as a fourth fossa, ascends the clivus, and passes ence Center, Memphis, TN. -

Strabismus: a Decision Making Approach
Strabismus A Decision Making Approach Gunter K. von Noorden, M.D. Eugene M. Helveston, M.D. Strabismus: A Decision Making Approach Gunter K. von Noorden, M.D. Emeritus Professor of Ophthalmology and Pediatrics Baylor College of Medicine Houston, Texas Eugene M. Helveston, M.D. Emeritus Professor of Ophthalmology Indiana University School of Medicine Indianapolis, Indiana Published originally in English under the title: Strabismus: A Decision Making Approach. By Gunter K. von Noorden and Eugene M. Helveston Published in 1994 by Mosby-Year Book, Inc., St. Louis, MO Copyright held by Gunter K. von Noorden and Eugene M. Helveston All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise, without prior written permission from the authors. Copyright © 2010 Table of Contents Foreword Preface 1.01 Equipment for Examination of the Patient with Strabismus 1.02 History 1.03 Inspection of Patient 1.04 Sequence of Motility Examination 1.05 Does This Baby See? 1.06 Visual Acuity – Methods of Examination 1.07 Visual Acuity Testing in Infants 1.08 Primary versus Secondary Deviation 1.09 Evaluation of Monocular Movements – Ductions 1.10 Evaluation of Binocular Movements – Versions 1.11 Unilaterally Reduced Vision Associated with Orthotropia 1.12 Unilateral Decrease of Visual Acuity Associated with Heterotropia 1.13 Decentered Corneal Light Reflex 1.14 Strabismus – Generic Classification 1.15 Is Latent Strabismus -

Advanced Anatomy & Physiology of The
By Diane F. Drake, LDO, ABOM, NCLEM, FNAO Introduction Terminology Presbyopia Anatomy Muscle Imbalances Refractive Errors Unequal refractive errors Spherical Correction Visualizing the Rx Cylindrical Correction Visual Angle and Minimum Visual Angle Minimum Visual Angle Visual Angle Subtend To extend under or to be opposite to The angle which is opposite the object being observed Minimum Detail The detail that must be detected on an object to positively identify or distinguish the object Minimum Detail E Minimum Detail Resolution The ability to detect minimum detail The resolving power of the normal eye is a minimum visual angle of 1 minute E The minimum visual angle of the letter is 1 minute The visual angle of the letter is 5 minutes Visual Acuity The measure of the angle subtended by the outer limits of rays of light coming from the minimum detail of an object as they enter the eye 20/20 or 6/6 Snell’s Law of Refraction n1 sin i = n2 sin r The Snellen Fraction The distance at which the test is made divided by the distance at which the smallest letter read subtends an angle of 5 minutes Snellen Letters Snellen Letters Minimum Angle of Resolution Landolt Ring (C) and the Illiterate E Contrast Sensitivity Terminology Emmetropia Ametropia Myopia Hyperopia Terminology Astigmatism Simple myopic Corneal astigmatism astigmatism Lenticular astigmatism Compound myopic Regular astigmatism astigmatism Irregular astigmatism Simple hyperopic astigmatism Compound hyperopic astigmatism Terminology Presbyopia Greek Presby -

Guidelines for Universal Eye Screening in Newborns Including RETINOPATHY of Prematurity
GUIDELINES FOR UNIVERSAL EYE SCREENING IN NEWBORNS INCLUDING RETINOPATHY OF PREMATURITY RASHTRIYA BAL SWASthYA KARYAKRAM Ministry of Health & Family Welfare Government of India June 2017 MESSAGE The Ministry of Health & Family Welfare, Government of India, under the National Health Mission launched the Rashtriya Bal Swasthya Karyakram (RBSK), an innovative and ambitious initiative, which envisages Child Health Screening and Early Intervention Services. The main focus of the RBSK program is to improve the quality of life of our children from the time of birth till 18 years through timely screening and early management of 4 ‘D’s namely Defects at birth, Development delays including disability, childhood Deficiencies and Diseases. To provide a healthy start to our newborns, RBSK screening begins at birth at delivery points through comprehensive screening of all newborns for various defects including eye and vision related problems. Some of these problems are present at birth like congenital cataract and some may present later like Retinopathy of prematurity which is found especially in preterm children and if missed, can lead to complete blindness. Early Newborn Eye examination is an integral part of RBSK comprehensive screening which would prevent childhood blindness and reduce visual and scholastic disabilities among children. Universal newborn eye screening at delivery points and at SNCUs provides a unique opportunity to identify and manage significant eye diseases in babies who would otherwise appear healthy to their parents. I wish that State and UTs would benefit from the ‘Guidelines for Universal Eye Screening in Newborns including Retinopathy of Prematurity’ and in supporting our future generation by providing them with disease free eyes and good quality vision to help them in their overall growth including scholastic achievement. -

Anatomy & Physiology of The
Anatomy & Physiology of The Eye 2017-2018 Done By: 433 Team Abdullah M. Khattab Important Doctor’s Notes Extra Abdullah AlOmair Resources: Team 433, Doctors Notes, Vaughan & Asbury’s General ophthalmology. Editing File Embryology of The Eye ............................................................................................. 2 ● Defects: ........................................................................................................................... 2 Development of The Eye After Birth .......................................................................... 3 ● Refractive power depends on two factors: ...................................................................... 3 The Orbit ................................................................................................................... 4 ● Seven bones contribute the bony orbit and surrounded by nasal sinuses. .................... 4 ● The orbital wall, pear-like shaped, formed by: ................................................................ 4 ● Structures Passing Through the Optic Openings: ........................................................... 4 Extraocular Muscles .................................................................................................. 1 ● Anatomy .......................................................................................................................... 1 ● Notes: .............................................................................................................................. 1 ● Field of action: -

Disclosure Ocular Anatomy and Motility Ocular Anatomy Overview the Human Vision System the Human Vision System Lids and Lacrimal
10/19/2012 Disclosure Ocular Anatomy and Motility Jenean Carlton BA, ABOC, NCLC 9President, Carlton & Associates, LLC – Carlton and Associates, 6 Course #214 Monterey Symposium LLC provides communications and educational materials for the optical industry 9Contributing Editor for Refractive Eyecare magazine. 6 Jenean Carlton BA, ABOC, NCLC 9Contributing Author Eyecare Business magazine. 9Communications Committee member OWA. 9Has been in the optical industry for 30 years with more than half of this time working in practices. 9Vision Monday’s Most Influential Women Award in Optical 2005 1 Ocular Anatomy Overview The Human Vision System 9 The eye is an amazing organ that works like a camera. 9 Think of the cornea and crystalline lens as the lenses of a camera, the iris as the shutter, and the retina as the photographic film. The Human Vision System Lids and Lacrimal System Vision takes place in the occipital lobe of The tear film has 3 layers: the brain Outer: the lipid layer (meibomian 9The brain can be glands in lids) is the oil layer. thought of as the development Middle: the aqueous layer center because it (lacrimal glands) is mainly water and provides oxygen converts and nutrients. electrical signals from the retina Inner: the mucin layer (goblet cells in conjunctiva) helps the tears into vision. adhere to the cornea. It is the mucus layer. 1 10/19/2012 Dry Eye Syndrome Lid Disorders What causes dry eyes? Ectropion= Out Treatments Entropion= In Ptosis- a drooping of the lid. Lids can have other problems too like turning out, in. Lids Disorders Lid Disorders Blepharitis is a chronic Hordeolum (stye) - inflammation- not an acute inflammation of a infection. -

Vertical Rectus Transposition in Duane&Rsquo
Eye (2015) 29, 839–842 & 2015 Macmillan Publishers Limited All rights reserved 0950-222X/15 www.nature.com/eye Sir, 5 Souza-Dias C. Congenital VI nerve palsy is Duane syndrome CORRESPONDENCE Vertical rectus transposition in Duane’s syndrome: does until disproven. Binocul Vis Strabismus Q 1992; 7:70. co-contraction worsen? 6 Sharma P, Tomar R, Menon V, Saxena R, Sharma A. Evaluation of periosteal fixation of lateral rectus and partial 1 We read with interest the article by Akar et al. We would VRT for cases of exotropic Duane’s retraction syndrome. like to make the following observations/queries. Indian J Ophthalmol 2014; 62: 204–208. In patients with Duane’s retraction syndrome there is some degree of subnormal and some degree of V Bhambhwani, PK Pandey, S Sood and K Rana anomalous innervation of the lateral rectus (LR) muscle. The extent and severity of the two may be variable. Guru Nanak Eye Centre and Maulana Azad Medical Presumably, subnormal innervation may lead to deficient College, New Delhi, India abduction and anomalous innervation may lead to E-mail: [email protected] co-contraction with globe retraction, palpebral aperture narrowing, or retraction equivalents like upshoots and Eye (2015) 29, 839; doi:10.1038/eye.2014.309; downshoots. published online 6 February 2015 In their article the authors describe patients of type 1 Duane syndrome to be with esotropia of 20 pd or more, an AHP larger than 201, limited abduction, and no significant upshoots or downshoots in the adducted Sir, position. There is no objective grading used for the Reply: Vertical rectus transposition in Duane’s measurement of shoots or palpebral aperture changes. -
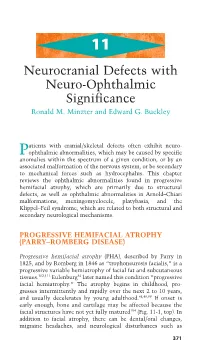
Neurocranial Defects with Neuro-Ophthalmic Significance
11 Neurocranial Defects with Neuro-Ophthalmic Significance Ronald M. Minzter and Edward G. Buckley atients with cranial/skeletal defects often exhibit neuro- Pophthalmic abnormalities, which may be caused by specific anomalies within the spectrum of a given condition, or by an associated malformation of the nervous system, or be secondary to mechanical forces such as hydrocephalus. This chapter reviews the ophthalmic abnormalities found in progressive hemifacial atrophy, which are primarily due to structural defects, as well as ophthalmic abnormalities in Arnold–Chiari malformations, meningomyelocele, platybasia, and the Klippel–Feil syndrome, which are related to both structural and secondary neurological mechanisms. PROGRESSIVE HEMIFACIAL ATROPHY (PARRY–ROMBERG DISEASE) Progressive hemifacial atrophy (PHA), described by Parry in 1825, and by Romberg in 1846 as “trophoneurosis facialis,” is a progressive variable hemiatrophy of facial fat and subcutaneous tissues.102,111 Eulenburg34 later named this condition “progressive facial hemiatrophy.” The atrophy begins in childhood, pro- gresses intermittently and rapidly over the next 2 to 10 years, and usually decelerates by young adulthood.48,49,99 If onset is early enough, bone and cartilage may be affected because the facial structures have not yet fully matured104 (Fig. 11-1, top). In addition to facial atrophy, there can be dental/oral changes, migraine headaches, and neurological disturbances such as 371 372 handbook of pediatric neuro-ophthalmology A B CD FIGURE 11-1A–D. Progressive nature of progressive hemifacial atrophy (PHA) in a patient at 8 years old (A) and again at 15 years (B), showing left-sided atrophy. Fundus photos of the normal contralateral side (C) and the ipsilateral affected side with hypopigmentary disturbances (D), par- ticularly along the inferior arcade. -
Squints Occur When the Eyes Do Not Work As a Team
Squints occur when the eyes do not work as a team. One eye may look forward while the other looks in a different direction (that eye may turn inwards, outwards, upwards, or even dow nwards, while the other eye looks forward). Medically the term for this is called “Strabismus” (being cross-eyed) and is actually a fairly common occurrence affecting 2 to 3% of the population. Usually it affects younger children between the ages of 18 months and 4 years of age. Risk factors for developing a Causes squint • The exact cause of most childhood squints has • Positive family history (i.e. if a parent never been discovered – this is termed has had a squint or needed glasses from idiopathic an early age, there may be an increased • This, however, does not mean that it cannot chance that their child may also be be corrected affect ed) • Prematurity and low birth weight Certain conditions can result in a squint: • Cerebral palsy and Down syndrome • Refractive errors – this is due to the eye’s • Tumours (in rare cases) inability to focus correctly on an object. Conditions such as short sightedness, far sightedness, and astigmatism may cause one or both eyes to turn inwards (esotropia) or outwards (exotropia). • Any condition that causes one or both eyes to have poor vision. Conditions such as Congenital cataracts or damage to the cornea, optic nerve or retina can adversely affect vision and therefore, the affected eye can no longer look forward, resulting in a squint • Some squints only occur when the eyes are looking in certain directions.