Laryngitis What Is Laryngitis?
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Report of Two Cases Presenting with Acute Abdominal Symptoms
Journal of Accident and Tension pneumothorax: report of two cases presenting J Accid Emerg Med: first published as 10.1136/emj.11.1.43 on 1 March 1994. Downloaded from Emergency Medicine 1993 with acute abdominal symptoms 10, 43-44 G.W. HOLLINS,1 T. BEATTIE,1 1. HARPER2 & K. LITTLE2 Departments of Accident and Emergency 1 Aberdeen Royal Infirmary, Foresterhill, Aberdeen and 2Royal Infirmary of Edinburgh, Lauriston Place, Edinburgh INTRODUCTION diagnoses were peptic ulcer disease or acute pancreatitis. Work-up appropriate to these diag- Tension pneumothorax constitutes a medical noses was commenced. An erect chest radiograph emergency and rapid diagnosis should be possible revealed a large pneumothorax with mediastinal on the basis of history and clinical examination. shift to the left. Following drainage using a large Following treatment with the delivery of high con- bore needle there was immediate resolution of his centration oxygen and the insertion of a large bore symptoms and all abdominal signs. An intercostal needle into the pleural space of the affected side, chest drain was formally sited and full expansion of the diagnosis can be confirmed radiologically and his right lung was achieved after 36 h. He was dis- an intercostal chest drain formally sited.1'2 We report charged home after 3 days. two cases where diagnosis was not made on the basis of history and examination alone. Both cases Case 2 presented with symptoms and signs suggestive of an acute intra-abdominal pathology and the diag- A 37-year-old male computer operator presented nosis was only made on radiological grounds. with a 1-week history of general malaise associated with mild neck and back pain. -

Acute Gastroenteritis
Article gastrointestinal disorders Acute Gastroenteritis Deise Granado-Villar, MD, Educational Gap MPH,* Beatriz Cunill-De Sautu, MD,† Andrea In managing acute diarrhea in children, clinicians need to be aware that management Granados, MDx based on “bowel rest” is outdated, and instead reinstitution of an appropriate diet has been associated with decreased stool volume and duration of diarrhea. In general, drug therapy is not indicated in managing diarrhea in children, although zinc supplementation Author Disclosure and probiotic use show promise. Drs Granado-Villar, Cunill-De Sautu, and Objectives After reading this article, readers should be able to: Granados have disclosed no financial 1. Recognize the electrolyte changes associated with isotonic dehydration. relationships relevant 2. Effectively manage a child who has isotonic dehydration. to this article. This 3. Understand the importance of early feedings on the nutritional status of a child who commentary does has gastroenteritis. contain a discussion of 4. Fully understand that antidiarrheal agents are not indicated nor recommended in the an unapproved/ treatment of acute gastroenteritis in children. investigative use of 5. Recognize the role of vomiting in the clinical presentation of acute gastroenteritis. a commercial product/ device. Introduction Acute gastroenteritis is an extremely common illness among infants and children world- wide. According to the Centers for Disease Control and Prevention (CDC), acute diarrhea among children in the United States accounts for more than 1.5 million outpatient visits, 200,000 hospitalizations, and approximately 300 deaths per year. In developing countries, diarrhea is a common cause of mortality among children younger than age 5 years, with an estimated 2 million deaths each year. -

Laryngitis from Reflux: Prevention for the Performing Singer
Laryngitis from Reflux: Prevention for the Performing Singer David G. Hanson, MD, FACS Jack J. Jiang, MD, PhD Laryngitis in General Laryngitis is the bane of performers and other professionals who depend on their voice for their art and livelihood. Almost every person has experienced acute laryngitis, usually associated with a viral upper- respiratory infection. Whenever there is inflammation of the vocal fold epithelium, there is an effect on voice quality and strength. Therefore, it is important to understand the factors that can cause laryngitis, especially the preventable causes of laryngitis. Laryngitis is a generic term for inflammation or irritation of the laryngeal tissues. The inflammation can be caused by any kind of injury, including infection, smoking, contact with caustic or acidic substance, allergic reaction, or direct trauma. Inflammatory response of the tissues includes leakage of fluid from blood vessels with edema or swelling, congregation of white blood cells, which release mediators of inflammation, and engorgement of the blood vessels. Most commonly laryngitis occurs from viral infection of the laryngeal epithelial lining associated with a typical cold. The viral infection is almost always quickly conquered by the body's immune system and lasts at most a few days. This kind of acute laryngitis rarely causes any long-term problem unless the vocal folds are damaged by overuse during the illness. Examination of the larynx will show whether the vocal folds are inflamed and allows some prediction of the degree of risk for damage. Other infections of the larynx are fortunately not common but include infections with bacteria and other organisms. -

Medical Terminology Abbreviations Medical Terminology Abbreviations
34 MEDICAL TERMINOLOGY ABBREVIATIONS MEDICAL TERMINOLOGY ABBREVIATIONS The following list contains some of the most common abbreviations found in medical records. Please note that in medical terminology, the capitalization of letters bears significance as to the meaning of certain terms, and is often used to distinguish terms with similar acronyms. @—at A & P—anatomy and physiology ab—abortion abd—abdominal ABG—arterial blood gas a.c.—before meals ac & cl—acetest and clinitest ACLS—advanced cardiac life support AD—right ear ADL—activities of daily living ad lib—as desired adm—admission afeb—afebrile, no fever AFB—acid-fast bacillus AKA—above the knee alb—albumin alt dieb—alternate days (every other day) am—morning AMA—against medical advice amal—amalgam amb—ambulate, walk AMI—acute myocardial infarction amt—amount ANS—automatic nervous system ant—anterior AOx3—alert and oriented to person, time, and place Ap—apical AP—apical pulse approx—approximately aq—aqueous ARDS—acute respiratory distress syndrome AS—left ear ASA—aspirin asap (ASAP)—as soon as possible as tol—as tolerated ATD—admission, transfer, discharge AU—both ears Ax—axillary BE—barium enema bid—twice a day bil, bilateral—both sides BK—below knee BKA—below the knee amputation bl—blood bl wk—blood work BLS—basic life support BM—bowel movement BOW—bag of waters B/P—blood pressure bpm—beats per minute BR—bed rest MEDICAL TERMINOLOGY ABBREVIATIONS 35 BRP—bathroom privileges BS—breath sounds BSI—body substance isolation BSO—bilateral salpingo-oophorectomy BUN—blood, urea, nitrogen -

Innovative Care for Chronic Conditions
Innovative Care for Chronic Conditions Building Blocks for Action global report Noncommunicable Diseases and Mental Health World Health Organization WHO Library Cataloging-in-Publication Data Innovative care for chronic conditions: building blocks for action: global report 1. Chronic disease 2. Delivery of health care, Integrated 3. Long-term care 4. Public policy 5. Consumer participation 6. Intersectoral cooperation 7. Evidence-based medicine I. World Health Organization. Health Care for Chronic Conditions Team. ISBN 92 4 159 017 3 (NLM classification: WT 31) This publication is a reprint of material originally distributed as WHO/MNC/CCH/02.01 © World Health Organization 2002 All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). Requests for permission to repro- duce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to Publications, at the above address (fax: +41 22 791 4806; email: [email protected]). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -
Hoarseness a Guide to Voice Disorders
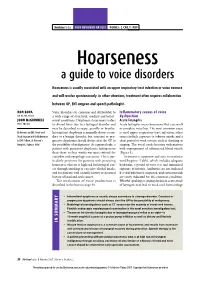
MedicineToday PEER REVIEWED ARTICLE POINTS: 2 CPD/1 PDP Hoarseness a guide to voice disorders Hoarseness is usually associated with an upper respiratory tract infection or voice overuse and will resolve spontaneously. In other situations, treatment often requires collaboration between GP, ENT surgeon and speech pathologist. RON BOVA Voice disorders are common and attributable to Inflammatory causes of voice MB BS, MS, FRACS a wide range of structural, medical and behav- dysfunction JOHN McGUINNESS ioural conditions. Dysphonia (hoarseness) refers Acute laryngitis FRCS, FDS RCS to altered voice due to a laryngeal disorder and Acute laryngitis causes hoarseness that can result may be described as raspy, gravelly or breathy. in complete voice loss. The most common cause Dr Bova is an ENT, Head and Intermittent dysphonia is normally always secon - is viral upper respiratory tract infection; other Neck Surgeon and Dr McGuinness dary to a benign disorder, but constant or pro- causes include exposure to tobacco smoke and a is ENT Fellow, St Vincent’s gressive dysphonia should always alert the GP to short period of vocal overuse such as shouting or Hospital, Sydney, NSW. the possibility of malignancy. As a general rule, a singing. The vocal cords become oedematous patient with persistent dysphonia lasting more with engorgement of submucosal blood vessels than three to four weeks warrants referral for (Figure 3). complete otolaryngology assessment. This is par- Treatment is supportive and aims to maximise ticularly pertinent for patients with persisting vocal hygiene (Table), which includes adequate hoarseness who are at high risk for laryngeal can- hydration, a period of voice rest and minimised cer through smoking or excessive alcohol intake, exposure to irritants. -

Parent's Guide to a Sore Throat
Contact your GP (or call 111) Useful contacts: again Your GP surgery on:....................................... Although in most cases the sore throat (Please insert surgery number here) improves in few days, please contact the GP if any of the following occurs: GP Out of Hours: (After 6.30pm and before 8am). Ring 111 and you can speak to a 1. Your child persistently refuses oral fl uids doctor. If necessary, your child can be seen and has not passed urine for over 18 at one of their centres. Parent’s guide hours. Bristol City Walk-in Centre at Broadmead 2. The fever does not settle within four or to a sore throat Medical Centre located in Boots fi ve days. (Mon-Sat 8am-8pm, Sundays and Bank Holidays 11am-5pm) on: 0117 954 9828 3. Your child develops diffi culty in swallowing despite regular paracetamol South Bristol NHS Community Hospital or ibuprofen. Urgent Care Centre (Every day 8am-8pm) on: 0117 342 9692 4. Your child starts drooling because they Visit www.nhs.uk to fi nd your nearest cannot swallow their saliva. centre. Call 999 If your child is seriously ill, you may be asked to attend the Children’s Hospital If your child develops severe breathing emergency department. diffi culties For further copies of this leafl et, or if you would like it in other formats or languages, please contact 0117 900 2384. Produced in partnership with Bristol Clinical Commissioning Group, North Bristol NHS Trust and University Hospitals Bristol NHS Foundation Trust. End date: June 2016 Your child has been diagnosed with a sore What is the treatment of a sore throat which is very common in children. -

Digital Medicine's March on Chronic Disease
RE-IMAGINING MEDICINE COMMENTARY Digital medicine’s march on chronic disease Joseph C Kvedar, Alexander L Fogel, Eric Elenko & Daphne Zohar Digital medicine offers the possibility of continuous monitoring, behavior modification and personalized interventions at low cost, potentially easing the burden of chronic disease in cost-constrained healthcare systems. hronic disease affects approximately half surgeries—successfully addressed leading well as 86% of healthcare costs3–5. The United Cof all adult Americans, accounting for at causes of morbidity and mortality of the time States has the highest disease burden of any least seven of the ten leading causes of death (Table 1)1. In contrast, the most pressing issues developed country6. Trends in the above data and 86% of all healthcare spending. The US facing healthcare in the twenty-first century are expected to worsen in the near future. The healthcare system is ill-equipped to handle our are chronic diseases (e.g., respiratory disor- growth in chronic disease prevalence means epidemic of chronic disease. This is because ders, heart disease and diabetes), and many are that, despite increases in average life span, we most chronic disorders develop outside preventable (e.g., through smoking cessation may be experiencing a decrease in average healthcare settings, and patients with these and diet; Table 1; Fig. 1)2. The increase in the health span (the period of a person’s life spent conditions require continuous intervention prevalence of chronic disease is the primary in generally good health)7. to make the behavioral and lifestyle changes contributor to skyrocketing healthcare costs Why are we continuing to lose ground needed to effectively manage disease. -

Crohn's Disease Manifesting As Acute Appendicitis: Case Report and Review of the Literature
Case Report World Journal of Surgery and Surgical Research Published: 20 Jan, 2020 Crohn's Disease Manifesting as Acute Appendicitis: Case Report and Review of the Literature Terrazas-Espitia Francisco1*, Molina-Dávila David1, Pérez-Benítez Omar2, Espinosa-Dorado Rodrigo2 and Zárate-Osorno Alejandra3 1Division of Digestive Surgery, Hospital Español, Mexico 2Department of General Surgery Resident, Hospital Español, Mexico 3Department of Pathology, Hospital Español, Mexico Abstract Crohn’s Disease (CD) is one of the two clinical presentations of Inflammatory Bowel Disease (IBD) which involves the GI tract from the mouth to the anus, presenting a transmural pattern of inflammation. CD has been described as being a heterogenous disorder with multifactorial etiology. The diagnosis is based on anamnesis, physical examination, laboratory finding, imaging and endoscopic findings. There have been less than 200 cases of Crohn’s disease confined to the appendix since it was first described by Meyerding and Bertram in 1953. We present the case of a 24 year old male, who presented with acute onset, right lower quadrant pain, mimicking acute appendicitis with histopathological report of Crohn’s disease confined to the appendix. Introduction Crohn’s Disease (CD) is a chronic entity which clinical diagnosis represents one of the two main presentations of Inflammatory Bowel Disease (IBD), and it occurs throughout the gastrointestinal tract from the mouth to the anus, presenting a transmural pattern of inflammation of the gastrointestinal wall and non-caseating small granulomas. The exact origin of the disease remains OPEN ACCESS unknown, but it has been proposed as an interaction of genetic predisposition, environmental risk *Correspondence: factors and immune dysregulation of intestinal microbiota [1,2]. -

14 Glossary of Healthcare Terms
Premera Reference Manual Premera Blue Cross 1144 GGlloossssaarryy ooff HHeeaalltthhccaarree TTeerrmmss A Accreditation: Health plan accreditation is a rigorous, comprehensive and transparent evaluation process through which the quality of the systems, processes and results that define a health plan are assessed. Acute: A condition that begins suddenly and does not last very long (e.g., broken arm). ‘acute” is the opposite of “chronic.” Acute Care: Treatment for a short-term or episodic illness or health problem. Adequacy: The extent to which a network offers the appropriate types and numbers of providers in a designated geographic distribution according to the relative availability of such providers in the area and the needs of the plan's members. Adjudication: The process of handling and paying claims. Also see Claim. Admission Notification: Hospitals routinely notify Premera of all inpatient admissions that link members to other care coordination programs, such as readmission prevention. The process includes verification of benefits and assesses any need for case management. Advance Directives: Written instructions that describe a member’s healthcare decision regarding treatment in the event of a serious medical condition which prevents the member from communicating with his/her physician; also called Living Wills. Allied Health Personnel: Specially trained and licensed (when necessary) healthcare workers other than physicians, optometrists, dentists, chiropractors, podiatrists, and nurses. Allowable: An amount agreed upon by the carrier and the practitioner as payment for covered services. Alpha Prefix: Three characters preceding the subscriber identification number on Blue Cross and/or Blue Shield plan ID cards. The alpha prefix identifies the member’s Blue Cross and/or Blue Shield plan or national account and is required for routing claims. -

Acute Conditions
Data from the Series 10 NATIONAL HEALTH SURVEY Number 6 9 Acute Conditions Incidenceand AssociatedDisability United States - July 1968-June1969 Statistics on the incidence of acute conditions and the associated days of restricted activity, bed disability, and time lost from work and school, by age, sex, calendar qunrter, residence, and geographic region, based on data collected in household interviews during the period July 196%June 1969. DHEW Publication No. (HSM) 72-1036 U.S. DEPARTMENT OF HEALTH, EDUCATION, AND WELFARE Public Health Service Health Services and Mental Health Administration National Center for Health Statistics Rockville, Md. February 1972 Vital and Health Statistics-SerieslO-No. 69 For sale by the Superintendent of Documents, U.S. Government Printing Office, Washington, D.C. 2M02- Price 65 et& NATIONAL CENTER FOR HEALTH STATISTICS THEODORE D. WOOLSEY, Director PHILIP S. LAWRENCE, Sc.D., Associate Director OSWALD K. SAGEN, Ph.D., Assistant Director for Health Statistics Development WALT R. SIMMONS, M.A., Assistant Director for Research and Scientific Development JAMES E. KELLY, D.D.S., Dental Advisor EDWARD E. MINTY, Executive Officer ALICk HAYWOOD, Information Officer DIVISION OF HEALTH INTERVIEW STATISTICS ELIJAH L. WHITE, Director ROBERT R. FUCHSBERG, Deputy Director RONALD W. WILSON, Chief. Analysis and Reports Branch KENNETH W. HAASE, Chief, Survey Methods Branch COOPERATION OF THE BUREAU OF THE CENSUS Under the legislation establishing the National Health Survey, the Public Health Service is authorized to use, insofar as possible, the services or facil ities of other Federal, State, or private agencies. In accordance with specifications established by the Health Interview Sur vey, the Bureau of the Census, under a contractual arrangement, participates in most aspects of survey planning, selects the sample, and collects the data. -

Point: the Changing Nature of Disease Implications for Health Services
POINT-COUNTERPOINT Point: The Changing Nature of Disease Implications for Health Services Barbara Starfield, MD, MPH he purpose of this commentary is to question the adequacy of characterizing illness Tdisease-by-disease. With rapidly increasing coexistence of multiple diseases within individuals, a disease-by-disease focus is becoming counter-productive to effectiveness, equity, and efficiency of health services. The sanctity of “disease” prevails in western medicine, despite the fact that diseases were never clearly distinct entities.1 Most quality of care efforts assume that early identification of risk factors for specific diseases improves health and, thereby, reduces costs, but this approach may not be suitable in meeting future healthcare needs. Diseases are heterogeneous entities.2 Many presumed “diseases,” such as diabetes, hypertension, malaria, breast cancer, chronic obstructive pulmonary disease, prostate cancer, and “heart disease,” are not distinct entities. Many are associated with other diseases. For example, people with hypothyroidism are 4 times more likely to have rheumatoid arthritis and cardiovascular diseases.2 Recognition of the heterogeneity of diseases is reflected in planning for the upcoming (11th) revision of the International Classification of Diseases, which recognizes that a disease label masks variability within diseases, including (but not limited to) causal mechanisms, clinical manifestations, and risk factors.3 Many types of prior experiences (including illnesses) predispose to a large variety of subsequent