Effects of Body Position on Ventilation/Perfusion Matching
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hypothermia Brochure
Visit these websites for more water safety and hypothermia prevention in- formation. What is East Pierce Fire & Rescue Hypothermia? www.eastpiercefire.org Hypothermia means “low temperature”. Washington State Drowning When your body is exposed to cold tem- Prevention Coalition Hypothermia www.drowning-prevention.org perature, it tries to protect itself by keeping a normal body temperature of 98.6°F. It Children’s Hospital & tries to reduce heat loss by shivering and Regional Medical Center In Our Lakes moving blood from your arms and legs to www.seattlechildrens.org the core of your body—head, chest and and Rivers abdomen. Hypothermia Prevention, Recognition and Treatment www.hypothermia.org Stages of Hypothermia Boat Washington Mild Hypothermia www.boatwashington.org (Core body temperature of 98.6°— 93.2°F) Symptoms: Shivering; altered judg- ment; numbness; clumsiness; loss of Boat U.S. Foundation dexterity; pain from cold; and fast www.boatus.com breathing. Boat Safe Moderate Hypothermia www.boatsafe.com (Core body temperature of 93.2°—86°F) Symptoms: Semiconscious to uncon- scious; shivering reduced or absent; lips are blue; slurred speech; rigid n in muscles; appears drunk; slow Eve breathing; and feeling of warmth can occur. mer! Headquarters Station Sum Severe Hypothermia 18421 Old Buckley Hwy (Core body temperature below 86°F) Bonney Lake, WA 98391 Symptoms: Coma; heart stops; and clinical death. Phone: 253-863-1800 Fax: 253-863-1848 Email: [email protected] Know the water. Know your limits. Wear a life vest. By choosing to swim in colder water you Waters in Western Common Misconceptions Washington reduce your survival time. -

Maximum Expiratory Flow Rates in Induced Bronchoconstriction in Man
Maximum expiratory flow rates in induced bronchoconstriction in man A. Bouhuys, … , B. M. Kim, A. Zapletal J Clin Invest. 1969;48(6):1159-1168. https://doi.org/10.1172/JCI106073. Research Article We evaluated changes of maximum expiratory flow-volume (MEFV) curves and of partial expiratory flow-volume (PEFV) curves caused by bronchoconstrictor drugs and dust, and compared these to the reverse changes induced by a bronchodilator drug in previously bronchoconstricted subjects. Measurements of maximum flow at constant lung inflation (i.e. liters thoracic gas volume) showed larger changes, both after constriction and after dilation, than measurements of peak expiratory flow rate, 1 sec forced expiratory volume and the slope of the effort-independent portion of MEFV curves. Changes of flow rates on PEFV curves (made after inspiration to mid-vital capacity) were usually larger than those of flow rates on MEFV curves (made after inspiration to total lung capacity). The decreased maximum flow rates after constrictor agents are not caused by changes in lung static recoil force and are attributed to narrowing of small airways, i.e., airways which are uncompressed during forced expirations. Changes of maximum expiratory flow rates at constant lung inflation (e.g. 60% of the control total lung capacity) provide an objective and sensitive measurement of changes in airway caliber which remains valid if total lung capacity is altered during treatment. Find the latest version: https://jci.me/106073/pdf Maximum Expiratory Flow Rates in Induced Bronchoconstriction in Man A. Bouiuys, V. R. HuNTr, B. M. Kim, and A. ZAPLETAL From the John B. Pierce Foundation Laboratory and the Yale University School of Medicine, New Haven, Connecticut 06510 A B S T R A C T We evaluated changes of maximum ex- rates are best studied as a function of lung volume. -

The Hazards of Nitrogen Asphyxiation US Chemical Safety and Hazard Investigation Board
The Hazards of Nitrogen Asphyxiation US Chemical Safety and Hazard Investigation Board Introduction • Nitrogen makes up 78% of the air we breath; because of this it is often assumed that nitrogen is not hazardous. • However, nitrogen is safe to breath only if it is mixed with an appropriate amount of oxygen. • Additional nitrogen (lower oxygen) cannot be detected by the sense of smell. Introduction • Nitrogen is used commercially as an inerting agent to keep material free of contaminants (including oxygen) that may corrode equipment, present a fire hazard, or be toxic. • A lower oxygen concentration (e.g., caused by an increased amount of nitrogen) can have a range of effects on the human body and can be fatal if if falls below 10% Effects of Oxygen Deficiency on the Human Body Atmospheric Oxygen Concentration (%) Possible Results 20.9 Normal 19.0 Some unnoticeable adverse physiological effects 16.0 Increased pulse and breathing rate, impaired thinking and attention, reduced coordination 14.0 Abnormal fatigue upon exertion, emotional upset, faulty coordination, poor judgment 12.5 Very poor judgment and coordination, impaired respiration that may cause permanent heart damage, nausea, and vomiting <10 Inability to move, loss of consciousness, convulsions, death Source: Compressed Gas Association, 2001 Statistics on Incidents CSB reviewed cases of nitrogen asphyxiation that occurred in the US between 1992 and 2002 and determined the following: • 85 incidents of nitrogen asphyxiation resulted in 80 deaths and 50 injuries. • The majority of -

Introduction to Airway Resistance Measurements
Introduction to airway resistance measurements Dr. David Kaminsky Department of Medicine The University of Vermont VT 05405 Burlington UNITED STATES OF AMERICA [email protected] AIMS Review physiology of airway resistance Survey measures of airway resistance Provide examples of clinical applications Highlight research applications SUMMARY Airway resistance (Raw) is one of the fundamental features of the mechanics of the respiratory system. While the flow-volume loop offers insight into the volume and flow of air, it is limited in terms of specific information regarding lung mechanics. Airway resistance is the ratio of driving pressure divided by flow through the airways. It specifies the pressure required to achieve a flow of air with a velocity of 1L/sec. If the airway is represented by a simple, rigid tube, with laminar flow of air through it, the airway resistance Raw = (8 x L x )/ r4, where L = length of the tube, = viscosity of the gas, and r = radius of the tube. It is important to note that the r4 relationship demonstrates how sensitive resistance is to the size of the tube, varying inversely with the 4th power of the radius. The inner diameter of the airway is itself determined by many factors, including airway smooth muscle contractile state, airway wall thickness (related to inflammation, edema and remodeling), airway wall buckling and formation of mucosal folds, the interdependence, or linkage, of airway and surrounding lung parenchyma, and the intrinsic elastic recoil of the lung parenchyma, which serves as a load on the airway and variably resists bronchoconstriction. Of course, the airways are not rigid tubes, and in fact flow is a complex process involving both laminar and turbulent conditions, so this calculation of Raw is an approximation only. -

Clinical Management of Severe Acute Respiratory Infections When Novel Coronavirus Is Suspected: What to Do and What Not to Do
INTERIM GUIDANCE DOCUMENT Clinical management of severe acute respiratory infections when novel coronavirus is suspected: What to do and what not to do Introduction 2 Section 1. Early recognition and management 3 Section 2. Management of severe respiratory distress, hypoxemia and ARDS 6 Section 3. Management of septic shock 8 Section 4. Prevention of complications 9 References 10 Acknowledgements 12 Introduction The emergence of novel coronavirus in 2012 (see http://www.who.int/csr/disease/coronavirus_infections/en/index. html for the latest updates) has presented challenges for clinical management. Pneumonia has been the most common clinical presentation; five patients developed Acute Respira- tory Distress Syndrome (ARDS). Renal failure, pericarditis and disseminated intravascular coagulation (DIC) have also occurred. Our knowledge of the clinical features of coronavirus infection is limited and no virus-specific preven- tion or treatment (e.g. vaccine or antiviral drugs) is available. Thus, this interim guidance document aims to help clinicians with supportive management of patients who have acute respiratory failure and septic shock as a consequence of severe infection. Because other complications have been seen (renal failure, pericarditis, DIC, as above) clinicians should monitor for the development of these and other complications of severe infection and treat them according to local management guidelines. As all confirmed cases reported to date have occurred in adults, this document focuses on the care of adolescents and adults. Paediatric considerations will be added later. This document will be updated as more information becomes available and after the revised Surviving Sepsis Campaign Guidelines are published later this year (1). This document is for clinicians taking care of critically ill patients with severe acute respiratory infec- tion (SARI). -
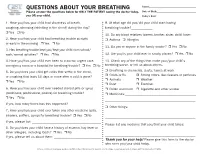
QUESTIONS ABOUT YOUR BREATHING Name:______Please Answer the Questions Below for ONLY the PATIENT Seeing the Doctor Today, Date of Birth:______You OR Your Child
QUESTIONS ABOUT YOUR BREATHING Name:_____________________________________ Please answer the questions below for ONLY THE PATIENT seeing the doctor today, Date of Birth:_______________________________ you OR your child. Today’s Date:_______________________________ 1. Have you/has your child had shortness of breath, 9. At what age did you/did your child start having coughing, wheezing (whistling in the chest) during the day? breathing trouble?_____________ r Yes r No 10. Do any blood relatives (parent, brother, sister, child) have: 2. Have you/has your child had breathing trouble at night r Asthma r Allergies or early in the morning r Yes r No 11. Do you or anyone in the family smoke? r Yes r No 3. Has breathing trouble kept you/kept your child from school/ work/normal activities? r Yes r No 12. Are you/is your child ever in smoky places? r Yes r No 4. Have you/has your child ever been to a doctor, urgent care, 13. Check any of the things that make your/your child’s emergency room or a hospital for breathing trouble? r Yes r No breathing worse, or tell us about others. 5. Do you/does your child get colds that settle in the chest, r Breathing in chemicals, dusts, fumes at work r Colds or flu r Strong odors, like cleaners or perfumes or coughing that lasts 10 days or more after a cold is gone? r Animals r Weather r Yes r No r Dust r Exercise 6. Have you/has your child ever needed steroid pills or syrup r Pollen and mold r Cigarette and other smoke (prednisone, prednisolone, prelone) for breathing trouble? r Medicines:___________________________________________ r Yes r No _______________________________________________________ If yes, how many times has this happened? ___________________ r Other things: 7. -

HANDOUT #1 CONCEPT INTRODUCTION PRESENTATION: PERFUSION Topic Description Definition of Perfusion the Passage of Oxygenated Capi
HANDOUT #1 CONCEPT INTRODUCTION PRESENTATION: PERFUSION Topic Description Definition of Perfusion The passage of oxygenated capillary blood through body tissues. Peripheral perfusion is passage (flow) of blood to the extremities of the body. Central perfusion is passage (flow) of blood to major body organs, including the heart and lungs. Scope of Perfusion Perfusion can be viewed on a continuum as adequate on one end and inadequate, decreased, or impaired on the other. Decreased Perfusion can range from minimal to severe. Ischemia refers to decreased Perfusion, while infarction is complete tissue death due to severe decreased Perfusion. Risk Factors/Populations at Risk for Examples of risk factors or populations at risk Impaired Perfusion for impaired Perfusion can be categorized as modifiable (can be changed) and nonmodifiable (cannot be changed) Modifiable factors include: • Obesity • Lack of physical activity/sedentary lifestyle • Smoking Nonmodifiable factors include age, gender, and race/ethnicity. Groups at risk for impaired Perfusion include those who are of advanced age (due to less elastic arterial vessels as a result of aging) and those who are African American and Hispanic. These racial/ethnic groups are most at risk for chronic diseases that can affect Perfusion such as diabetes mellitus, hypertension, hyperlipidemia, and peripheral vascular disease. The cause of these variations is not known, but dietary and environmental factors may contribute to the higher incidence of chronic disease in these groups. Newborns and infants who have congenital heart anomalies are also at risk for impaired central Perfusion. Many of these defects can be surgically repaired to regain adequate Perfusion. Physiologic Consequences of Impaired Consequences of impaired Perfusion vary Perfusion depending on the degree of impairment. -

What Are the Health Effects from Exposure to Carbon Monoxide?
CO Lesson 2 CARBON MONOXIDE: LESSON TWO What are the Health Effects from Exposure to Carbon Monoxide? LESSON SUMMARY Carbon monoxide (CO) is an odorless, tasteless, colorless and nonirritating Grade Level: 9 – 12 gas that is impossible to detect by an exposed person. CO is produced by the Subject(s) Addressed: incomplete combustion of carbon-based fuels, including gas, wood, oil and Science, Biology coal. Exposure to CO is the leading cause of fatal poisonings in the United Class Time: 1 Period States and many other countries. When inhaled, CO is readily absorbed from the lungs into the bloodstream, where it binds tightly to hemoglobin in the Inquiry Category: Guided place of oxygen. CORE UNDERSTANDING/OBJECTIVES By the end of this lesson, students will have a basic understanding of the physiological mechanisms underlying CO toxicity. For specific learning and standards addressed, please see pages 30 and 31. MATERIALS INCORPORATION OF TECHNOLOGY Computer and/or projector with video capabilities INDIAN EDUCATION FOR ALL Fires utilizing carbon-based fuels, such as wood, produce carbon monoxide as a dangerous byproduct when the combustion is incomplete. Fire was important for the survival of early Native American tribes. The traditional teepees were well designed with sophisticated airflow patterns, enabling fires to be contained within the shelter while minimizing carbon monoxide exposure. However, fire was used for purposes other than just heat and cooking. According to the historian Henry Lewis, Native Americans used fire to aid in hunting, crop management, insect collection, warfare and many other activities. Today, fire is used to heat rocks used in sweat lodges. -

Role of the Allergist-Immunologist and Upper Airway Allergy in Sleep-Disordered Breathing
AAAAI Work Group Report Role of the Allergist-Immunologist and Upper Airway Allergy in Sleep-Disordered Breathing Dennis Shusterman, MD, MPHa, Fuad M. Baroody, MDb, Timothy Craig, DOc, Samuel Friedlander, MDd, Talal Nsouli, MDe, and Bernard Silverman, MD, MPHf; on behalf of the American Academy of Allergy, Asthma & Immunology’s Rhinitis, Rhinosinusitis and Ocular Allergy Committee Work Group on Rhinitis and Sleep-disordered Breathing San Francisco, Calif; Chicago, Ill; Hershey, Pa; Solon, Ohio; Washington, DC; and Brooklyn, NY BACKGROUND: Sleep-disordered breathing in general and RESULTS: Survey results were returned by 339 of 4881 active obstructive sleep apnea in particular are commonly encountered members (7%). More than two-third of respondents routinely conditions in allergy practice. Physiologically, nasal (or asked about sleep problems, believed that sleep-disordered nasopharyngeal) obstruction from rhinitis, nasal polyposis, or breathing was a problem for at least a “substantial minority” adenotonsillar hypertrophy are credible contributors to snoring (10%-30%) of their adult patients, and believed that medical and nocturnal respiratory obstructive events. Nevertheless, therapy for upper airway inflammatory conditions could existing practice parameters largely relegate the role of the potentially help ameliorate sleep-related complaints. Literature allergist to adjunctive treatment in cases of continuous positive review supported the connection between high-grade nasal airway pressure intolerance. congestion/adenotonsillar hypertrophy and obstructive sleep OBJECTIVES: To survey active American Academy of Allergy, apnea, and at least in the case of pediatric patients, supported the Asthma & Immunology members regarding their perceptions use of anti-inflammatory medication in the initial management and practices concerning sleep-disordered breathing in adult and of obstructive sleep apnea of mild-to-moderate severity. -

Dynamic Mechanics of the Lung Answer to the Last Class’S Question
Dynamic mechanics of the lung Answer to the Last class’s question Resistive (Frictional Forces) Opposing Lung Inflation Frictional opposition occurs only when the system is in motion. Frictional opposition to ventilation has the two components: 1. tissue viscous resistance 2. airway resistance. Tissue Viscous Resistance: the impedance of motion (opposition to flow) caused by displacement of tissues during ventilation that includes the lungs, rib cage, diaphragm, and abdominal organs. The frictional resistance is generated by the movement of each organ surface sliding against the other (e.g., the lung lobes sliding against each other and against the chest wall). Tissue resistance accounts for only approximately 20% of the total resistance to lung inflation. In conditions : obesity, pleural fibrosis, and ascites, the tissue viscous resistance increases the total impedance to ventilation. Airway Resistance (flow resistance) - Resistance to ventilation by the movement of gas through the airways. • accounts for approximately 80% of the frictional resistance to ventilation. • -is usually expressed in units of cm H2O/L/sec: R= ∆P/ ∆V • Airway resistance in healthy adults ranges from approximately 0.5 to 2.5 cm H2O/L/sec. • To cause gas to flow into or out of the lungs at 1 L/sec, a healthy person needs to lower his alveolar pressure 0.5 to 2.5 cm H2O below atmospheric pressure. Measurement of Airway Resistance • Airway resistance is the pressure difference between the alveoli and the mouth divided by a flow rate. Mouth pressure is easily measured with a manometer. Alveolar pressure can be deduced from measurements made in a body plethysmograph. -
Breathing Air Quality, Sampling and Testing
Breathing Air Quality, Sampling and Testing Environmental Health Laboratory Department of Environmental and Occupational Health Sciences School of Public Health University of Washington Funding and support from The State of Washington Department of Labor & Industries Safety & Health Investment Projects Medical Aid and Accident Fund Breathing Air Quality, Sampling, and Testing Environmental Health Laboratory Department of Environmental and Occupational Health Sciences School of Public Health University of Washington Funding and support from The State of Washington Department of Labor & Industries Safety & Health Investment Projects Medical Aid and Accident Funds 1 University of Washington Environmental Health Laboratory Table of Contents Overview ...............................................................................1 Background ...........................................................................2 Regulated Components of Breathing Air ...............................7 Performance of Breathing Air Testing Kits ............................9 Laboratory Accreditation .....................................................18 Guidance Summary .............................................................19 Glossary ..............................................................................20 References ...........................................................................22 List of Tables Table 1. Breathing Air Quality Specifications ........................2 Table 2. Description of Kits Tested ........................................9 -

Diving Air Compressor - Wikipedia, the Free Encyclopedia Diving Air Compressor from Wikipedia, the Free Encyclopedia
2/8/2014 Diving air compressor - Wikipedia, the free encyclopedia Diving air compressor From Wikipedia, the free encyclopedia A diving air compressor is a gas compressor that can provide breathing air directly to a surface-supplied diver, or fill diving cylinders with high-pressure air pure enough to be used as a breathing gas. A low pressure diving air compressor usually has a delivery pressure of up to 30 bar, which is regulated to suit the depth of the dive. A high pressure diving compressor has a delivery pressure which is usually over 150 bar, and is commonly between 200 and 300 bar. The pressure is limited by an overpressure valve which may be adjustable. A small stationary high pressure diving air compressor installation Contents 1 Machinery 2 Air purity 3 Pressure 4 Filling heat 5 The bank 6 Gas blending 7 References 8 External links A small scuba filling and blending station supplied by a compressor and Machinery storage bank Diving compressors are generally three- or four-stage-reciprocating air compressors that are lubricated with a high-grade mineral or synthetic compressor oil free of toxic additives (a few use ceramic-lined cylinders with O-rings, not piston rings, requiring no lubrication). Oil-lubricated compressors must only use lubricants specified by the compressor's manufacturer. Special filters are used to clean the air of any residual oil and water(see "Air purity"). Smaller compressors are often splash lubricated - the oil is splashed around in the crankcase by the impact of the crankshaft and connecting A low pressure breathing air rods - but larger compressors are likely to have a pressurized lubrication compressor used for surface supplied using an oil pump which supplies the oil to critical areas through pipes diving at the surface control point and passages in the castings.